







INTRODUCTION
The Achilles tendon is the most commonly ruptured tendon of the lower extremity. The rates of Achilles tendon rupture vary in the literature, with recent studies reporting 18 patients per 100,000 annually (Shamrock and Varacallo 2022). This injury occurs most often in middle aged men between the ages of 30 to 50 (Nordenholm et al. 2022; Rompe et al. 2007). While it is more commonly seen in those who participate in sports, less active individuals are also affected (Lin, Duan, and Yang 2019). Achilles tendon ruptures are misdiagnosed during the initial examination up to 25% of the time (Song and Hua 2019). When acute injuries are neglected and treatment is delayed, a chronic rupture is often the initial presentation. The window for acute diagnosis and treatment is generally 4-6 weeks from time of injury. Delay in presentation makes it more difficult to detect and ultimately treat chronic Achilles tendon ruptures. Upon injury onset, the ends of the tendon often retract, causing gap formation that can increase with time and fill with fibrous scar tissue, thus making the injury less noticeable. However, scar tissue is weaker and biomechanically unsound compared to native tendon tissue and can elongate over time, causing patients to experience alterations in gait (i.e. limping) and weakness in ankle plantar flexion (Malagelada, Clark, and Dega 2016).
In most cases, chronic Achilles tendon tears are treated surgically. While non-operative treatment can be considered, results are generally not as successful (Malagelada, Clark, and Dega 2016; Maffulli, Via, and Oliva 2015a). In one study, a 55% satisfaction rate was reported after conservative treatment and the patients’ conditions were notably slow to improve (Christensen 1953). If surgery is not an option, the use of ankle foot orthoses and braces can help alleviate symptoms and pain. Due to the retraction of the tendon ends, primary end-to-end repair is generally not achievable and other surgical techniques have been developed to manage chronic ruptures. The goals of these procedures are to restore tendon length and bridge the gap between the ruptured ends. Operative methods can involve repair or reconstruction, and in both strategies, there is a role for tissue augmentation. In cases where there is sufficient tissue quality to complete a repair, the elongated tendon can be shortened to restore its original length and scar tissue is incorporated into the repair.

Repairs or reconstructions can be augmented with grafts, tendon transfers, biologics and synthetic implants in order to improve healing, strength, or integrity of the construct (Barber et al. 2008). Improving the repair construct overall can be particularly beneficial during the early stages of healing and when the tissue is perceived to be of poor quality. Surgical options for repair include gastrocnemius V-Y advancement, fascial turndown flaps, and tendon transfers using tendons such as the flexor hallucis longus, flexor digitorum longus, peroneus brevis, gracilis, semitendinosus, and allografts (Malagelada, Clark, and Dega 2016; Maffulli et al. 2007). However, there is no “gold standard” surgical repair technique and these methods are not without shortcomings. V-Y advancement often has to be used in combination with other techniques and is generally only used to repair smaller defects (less than 5 cm) (Padanilam 2009). The use of turndown flaps requires long incisions and the length and width of the turndown flap itself can affect the resulting strength of the repair (Malagelada, Clark, and Dega 2016). FHL transfer, the most common tendon transfer for Achilles tendon ruptures, has been reported to lead to a loss in push-off strength, particularly in athletes (Malagelada, Clark, and Dega 2016; Koh et al. 2019). In some cases, peroneus brevis tendon transfer has been shown to lead to a loss in eversion strength (Padanilam 2009). While the use of Achilles tendon allografts has demonstrated some success, there have been reports of persistent weakness in the treated tendon compared to the uninjured side (Maffulli and Ajis 2008).
To improve healing, augmentation of Achilles tendon tears with various materials including acellular dermal matrices (GRAFTJACKET™), xenografts (Trellis Collagen Ribbon), and synthetics (Artelon graft) has been explored. These materials can be broadly split into two categories: biologics and synthetics. Biologics can aid in the healing process by increasing tissue thickness and serving as a source of collagen, but they do not reinforce repairs mechanically or structurally. Synthetics provide mechanical strength but cannot aid in healing or production of tissue. Therefore, there is a need for an implant that can bridge this gap and provide both biology and strength.
In 2021, a biocomposite scaffold, BioBrace® (CONMED, New Haven, CT), was introduced for repair and augmentation of injured tendons and soft tissue where weakness exists. BioBrace® is composed of highly porous type I collagen and bioresorbable poly(L-Lactide) (PLLA) microfilaments (McMillan, Arciero, and Ford 2021). This scaffold has been shown to encourage the induction, maturation, and remodeling of host tissue and load shares at time zero of implantation, thereby providing both biology and strength to the repair (McMillan, Arciero, and Ford 2021; Carter et al. 2021). These properties would allow BioBrace to span the gap formed by chronic Achilles tendon ruptures through the formation of new native tissue in and around the implant as early as 3 weeks (McMillan, Arciero, and Ford 2021). This case report presents the use of BioBrace to augment the repair of a chronic Achilles tendon defect.

CASE REPORT
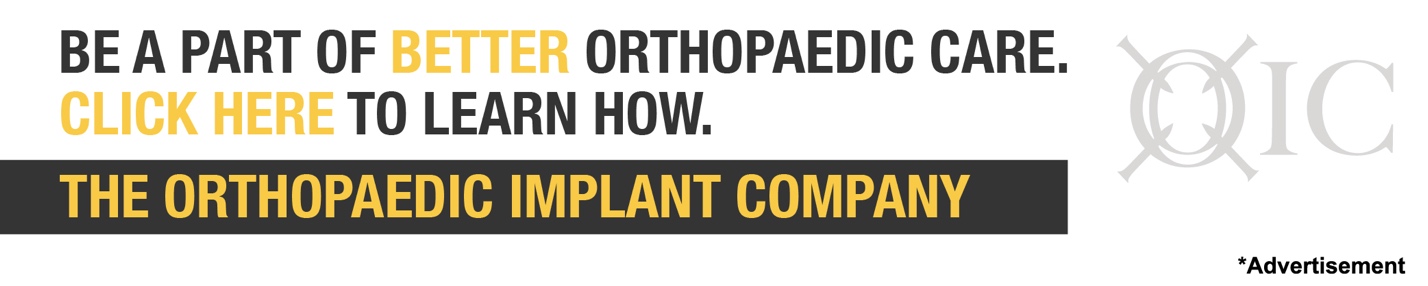
A 31-year-old male presented with a chronic tear in the midsubstance of his right Achilles tendon. The patient had no active motion and walked with a “slapping foot gait.” His pre-operative dorsiflexion was 4-/5+ and he had no strength in plantar flexion. MRI of the tendon showed cavitation and infiltration of dense fibrous tissue indicative of the chronic nature of this rupture with the likelihood of poor-quality tissue (Figure 1). The middle of the tendon consisted of degenerative, retracted tissue. Scarring was likely due to the fact that 8 weeks had elapsed since the time of injury.

The patient elected to undergo surgery to treat this injury. The repair was augmented with the BioBrace implant due to the large gap and poor tissue quality in this tendon (Figure 2). BioBrace was used to assist in the healing process of this chronic tear and to fill the tendon defect by aiding in the re-growth of native tendon tissue (McMillan, Arciero, and Ford 2021). If BioBrace had not been available, the procedure would have been completed using an autograft, allograft, or the fascia flap turndown technique.

A BioBrace 23x30mm implant was cut in half length-wise to create two strips measuring approximately 12mm x 30mm each and in order to better fit the tendon defect. These strips were placed end-to-end within the defect (Figure 3) and sutured in place using a Krackow-type stitch starting from the proximal end, progressing to the distal end, and then back up to the proximal part of the defect (Figure 4). The remaining Achilles tendon tissue was enclosed around the BioBrace to create a tubular type configuration. The repair was completed using suture tape for additional reinforcement. Whether or not a larger gap could be treated with this technique is beyond the scope of this report and could be further assessed in a future study.



Post-operatively, the ankle was placed into a short leg cast for two weeks. After suture removal, the patient was placed into a CAM walker with adjustable hinges, allowing for early progressive range of motion under the hypothesis that the strength of the repair construct with the use of BioBrace would allow for this aggressive early range of motion post-op program.
Eight weeks after surgery, the patient was taken out of his CAM walker. Examination revealed active dorsiflexion and plantarflexion of the ankle (see Video 1); the patient began a formal physical therapy program. The post-operative strength values were measured as 4+/5+ for plantar flexion and 5+/5+ for dorsiflexion. The patient had no active motion preoperatively but demonstrated 25° dorsiflexion and 35° plantar flexion for post-operative range of motion.
Six months after surgery, the patient demonstrated excellent range of motion and the ability to do a double leg hop (see Video 2). At 6-months, post-operative MRI showed the tendon defect to be almost completely filled with new tissue that was well-integrated with the underlying tendon (Figure 6).

DISCUSSION
Chronic Achilles tendon ruptures remain a challenge to treat due to the abundance of scar tissue in the injured area, poor vascularity and the gap that often exists between the ends of the ruptured tendon. Current treatment options aim to repair this gap and restore the desired length and tension to the Achilles tendon (Lin, Duan, and Yang 2019).
Traditionally, chronic Achilles tendon ruptures are treated operatively using a variety of methods including repair, tendon transfers, and V-Y advancement. No optimal treatment has been documented and the technique is generally chosen depending on the amount of tendon that can be salvaged (Lin et al. 2016). While these methods are effective, they have disadvantages. Some patients continue to report discomfort and weakness in the tendon even after surgery. In one study, strength deficits of 9%-23% were reported postoperatively after treatment with a gastrocnemius fascial turndown flap procedure (Takao et al. 2003). The use of autologous tendon transfers and autografts may be accompanied by donor site morbidity (Barber et al. 2008). Tendon transfers can lead to a loss of function and weakness from the area where the tendon was harvested. In one study, transfer of the flexor hallucis longus was associated with a decrease in push-off strength (Malagelada, Clark, and Dega 2016). Another study demonstrated a 29.5% reduction in plantar flexion power in patients treated with an FHL transfer compared to the uninjured side (Wapner et al. 1993). It is not uncommon for calf circumference in the operated leg to remain significantly smaller than the contralateral side with diminished strength as well (Maffulli, Via, and Oliva 2015b). Generally, Achilles tendon post-operative rehabilitation protocols often involve 6-8 weeks of cast immobilization. However, studies have shown that this can lead to 10% minimum strength deficit in the gastrocsoleus complex of the treated side compared to the uninjured leg after rehab. Another study showed early mobilization following operative treatment led to earlier return to sports and improved plantar flexion strength (Rettig et al. 2005). With the tenuous nature of the Achilles tendon tissue in a chronic rupture, many surgeons may be concerned about allowing an early progressive range of motion program after repair or reconstruction. However, in cases of prolonged immobilization after surgery, strength deficits and stiffness may be more profound.
A wide variety of synthetic and biologic materials have been reported in the literature to improve healing and durability of the repair. While reports with the use of these materials demonstrate some success, there remains concern surrounding the use of synthetic materials and the lack of biological integration seen in these as well as acellular dermal matrices. Synthetic materials like suture tapes that are not resorbable can be associated with postoperative infections and wound breakdown (Maffulli and Leadbetter 2005). They provide mechanical strength but cannot biologically integrate and can often stress shield the native tendon rather than load share. Another synthetic graft has been shown to significantly improve load to failure in an Achilles tendon cadaveric model (Giza et al. 2011). However, in one case report, this same graft had to be removed when the patient presented with stiffness, pain, and difficulty walking one year post-operatively. After excision of the graft, evaluation of the histology revealed acellular tissue that demonstrated a paucity of vascularization, suggesting a lack of healing due to the synthetic nature of the graft (Mohamed et al. 2019). Dermal allografts have been used to augment Achilles tendon ruptures as well and have demonstrated good results to date. However, dermal allografts do not always incorporate or transition into functional tissue. Other options such as allografts also present clinical challenges. They incorporate slower than autografts, resulting in a longer remodeling period and may also be potentially associated with disease transmission (Song and Hua 2019).
The ideal material must act as a biologic scaffold to allow for rapid integration with host tissue, load share at the time of surgical implant, and improve post-operative healing. There is a benefit to increasing the strength of the repair construct to potentially accelerate post-operative rehabilitation and return to daily activities. It has been shown that Achilles tendon repair outcomes are improved when rehabilitation and weightbearing are initiated early post-surgery (Kangas et al. 2007; Mortensen, Skov, and Jensen 1999; McWilliam and Mackay 2016). This suggests that increasing the time zero strength of the construct and improving healing by augmenting the repair may be beneficial. The BioBrace implant combines both characteristics into a single construct.
This patient presented a challenge due to the chronic nature of the tear and the large defect with cavitation. It was determined that the repair should be surgically augmented. The goal of this repair was to induce rapid host tissue ingrowth and provide load sharing strength to improve overall tendon healing via use of the BioBrace implant. Six-month post-operative imaging indicated that the defect was infiltrated with new tissue and that the BioBrace implant was integrated with surrounding host tissue. Post-operative functional tests suggest that the patient is on track towards an excellent recovery with dorsiflexion and plantar flexion strength and motion scores greatly improved compared to preoperative values. At six months post-op, the patient was back to full duty, loading and unloading heavy cargo and getting into and out of an 18-wheeler truck. As this was a worker’s compensation injury, early return was even more impressive after repair of a chronic Achilles tendon rupture. While this case report is promising, studies with more patients and longer-term follow-up are required to further evaluate the potential clinical benefits of this implant.