

INTRODUCTION
Rotator cuff repair (RCR) is one of the most common arthroscopic orthopedic procedures performed worldwide. On average, over 400,000 RCR’s are performed annually in the United States (“PearlDiver,” n.d.). However, a high number of clinical and subclinical re-tears exist post procedure. These reported rates vary tremendously within the literature, however the highest rates have been seen in large (>3cm) to massive tears and revision tears (Agrawal 2012; Galatz et al. 2004; Burkhart et al. 2007). A multitude of variables have been attributed to the risk of failure. These include: size of the tear, time to surgery, patient comorbidities, poor surgical technique, and fatty atrophy of the rotator cuff tissue (Gladstone et al. 2007).
Miller et al. looked at 22 consecutive large (>3cm) double row RCR’s and reported a 41% failure rate based upon ultrasound evaluation. 78% of these (9/22) occurred within the first 3 months (Miller et al. 2011). Chona et al. reviewed 13 articles examining re-tear rates in medium, large, and massive rotator cuff tears. Their findings demonstrated an approximate 20% re-tear rate for medium tears over the course of 15 months. Large tears had an approximate 40% re-tear rate and massive tears ranged from 20% to 60% (Chona et al. 2017).
Advances in the RCR over the past 2 decades have nearly eliminated failures related to implant (Mirzayan et al. 2019). Currently the most common mechanism of RCR failure appears to be suture “pull through” at the suture-tendon interface (Ponce et al. 2013; Ma et al. 2006). As such, the use of biologics and rotator cuff augmentation have seen significant growth in interest, both in the literature and amongst industry. As a method of decreasing RCR failure rates, the use of bio-inductive implants and dermal grafting have presented attractive surgical options for surgeons to re-inforce repairs and decrease the risk of “failure”.
The use of a type I bovine, bio-inductive implant (REGENETEN™) has shown promising results in both partial and full thickness rotator cuff repairs through the induction new tendon-like tissue (Bishai et al. 2021a; Bushnell et al. 2021). While biologically successful at the induction of new tissue, the bio-inductive implant lacks structural strength. As such the benefit of this type of implant is not necessarily realized at time zero of implantation for additional strength of the repair, but rather in the induction of new tissue to prevent future re-tear.
On the contrary, dermal allografts, (acellular dermal matrices (ADM)), when used to reinforce rotator cuff repairs, increase the load to failure across the construct at time zero of implantation (Mirzayan et al. 2019; Barber, Herbert, and Boothby 2008; Barber et al. 2012). In patients with large tears (>3cm), an 85% successful healing rate via gadolinium enhanced MRI was noted with human ADM augmentation versus a 40% healing rate in the non-augmented group (Barber et al. 2012). However, drawbacks exist with human ADM, including increased time to tissue incorporation, cost, technical difficulty with implantation, and the inherent risks of allograft tissue. The purpose of this review is to examine the potential fit for a bio-composite scaffold in rotator cuff repair augmentation in order to bridge the gaps between the currently available options.
BIO-BRACE™
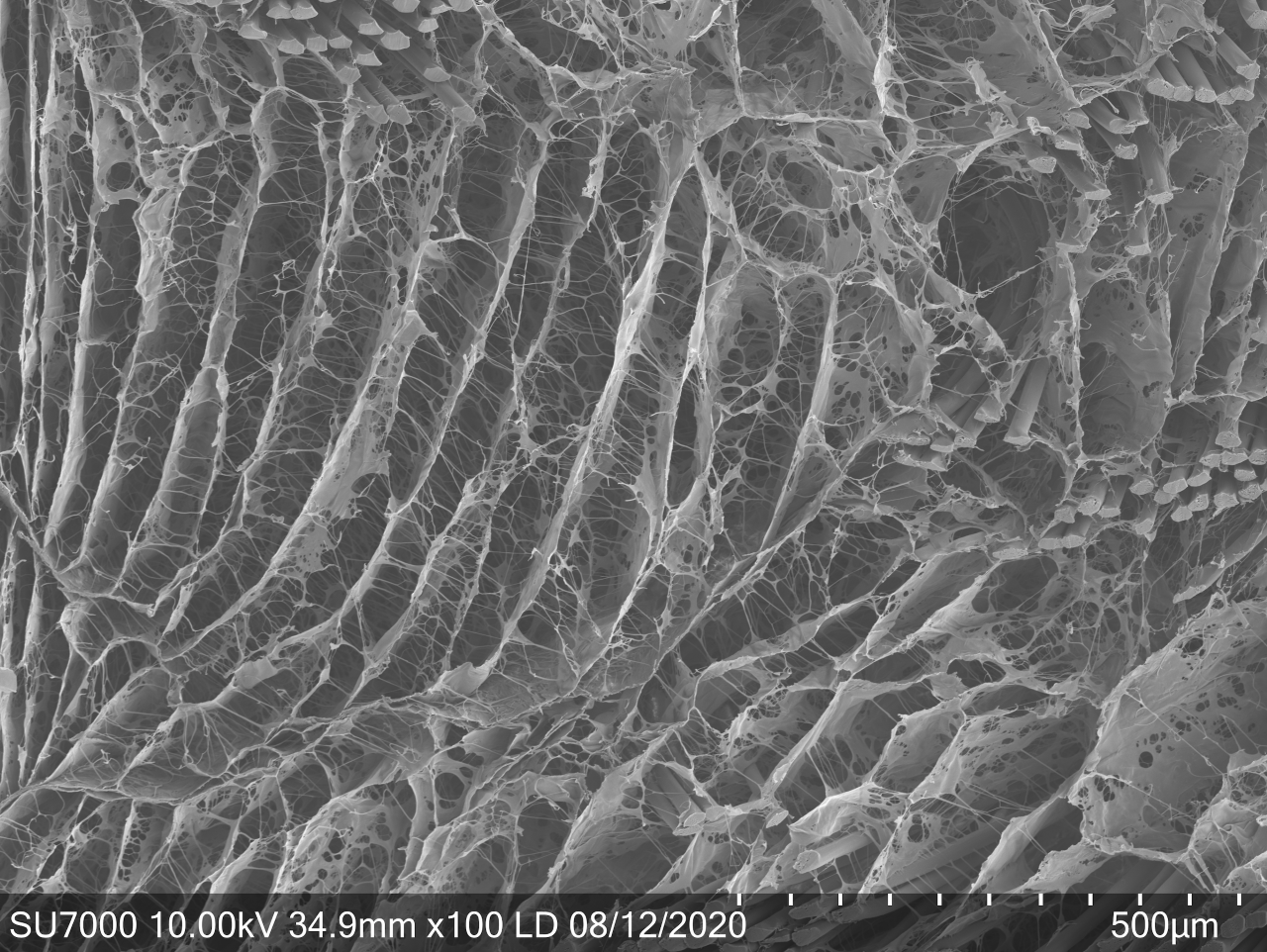
The BioBrace™ (Biorez Inc, New Haven, CT, USA) is a novel bio-inductive scaffold composed of highly porous type I collagen and bio-resorbable poly(L-Lactide) (PLLA) microfilaments intended for the augmentation of tendon and ligament repair (Figure 1). It’s open 3-D scaffold allows for induction, maturation, and remodeling of new host tissue while providing load sharing strength (141N) at the time of implantation (Figure 2) (Carter et al. 2021). In turn, gapping and re-tears prevention may occur by increasing the thickness of the tendon at time zero and beyond (Bokor et al. 2019a, 2019b; Thon et al. 2019).


The large open pores (80% porosity) of the implant allow for native soft tissue ingrowth, while maintaining structural strength provided by the bio-resorbable PLLA micro-filaments (15 micron) reinforcement.(Carter et al. 2021) The degradation curve of the PLLA micro-filaments permits the functional maturation and remodeling of host-generated repair tissue while maintaining strength for up to 24 months (Walsh et al. 2021). This provides more than sufficient time as a structural scaffold, without the concern of being a permanent implant.
The BioBrace™ for rotator cuff augmentation uniquely meets the need for the next generation of biologic rotator cuff solutions by combining the benefits from bio-inductive xenograft implants and ADM. The highly porous bio-inductive/bio-composite implant allows for a resorbable rotator cuff augment that can provide strength at time zero, rapid incorporation, and ultimate resorption of the implant while new native tissue remains. The BioBrace™ has been shown to incite a robust native healing response and the formation of regularly oriented connective tissue fibers in large animal models.(Walsh et al. 2021; Carter et al. 2021) These characteristics may lend themselves to enhanced graft/repair healing incorporation. In turn this can potentially lead to enhanced rehabilitation protocols and ultimately decreased failures.
CASE APPLICATION ALGORITHM
The lead authors’ current indication for the use of the BioBrace™ in RCR are: revision full thickness RCR, large (>3cm) and massive tears, chronic full thickness tears with Goutier classification grade 3 or 4 fatty infiltration, and full thickness tears in patients with multiple medical co-morbidities (smoking, diabetes, etc.). This is not used as a replacement for an ADM sheet in superior capsular reconstructions (SCR).
Xenograft bio-inductive implants (REGENETEN™) are reserved for high grade articular sided partial thickness RCR’s and patients with recalcitrant rotator cuff tendinopathies. ADM strips (DERMIS ON DEMAND™) have become a very efficient RCR reinforcement in medium to large RCR’s and are utilized as “rebar” and reinforcement when appropriate.
TECHNICAL PEARLS
The BioBrace™ implant for RCR comes available as a 23mm wide by 30mm length implant, with a 3 mm thickness. The implant can be trimmed if needed to allow for appropriate rotator cuff coverage. The implant is easy to work with, however the lead author recommends wetting the implant prior to passing suture through it, as this appears to decrease the suture friction. Interestingly, the BioBrace™ has the ability to “wick” when reconstituted (Figure 3). As such the individual surgeon maybe choose to soak the implant in either saline or a biologic of their choosing such as platelet rich plasma (PRP) or bone marrow aspirate concentrate (BMAC).
_the_biobrace_has_the_ability_to_act_as_a_wick_during.jpg)
Suture Passing and Delivery
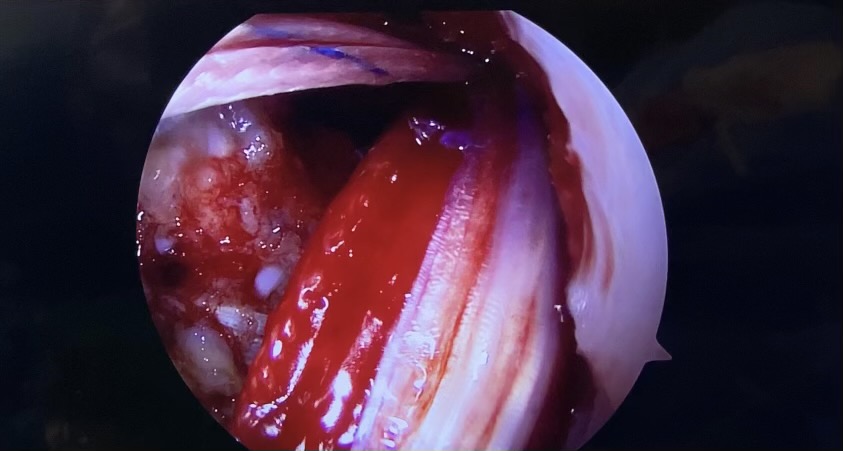
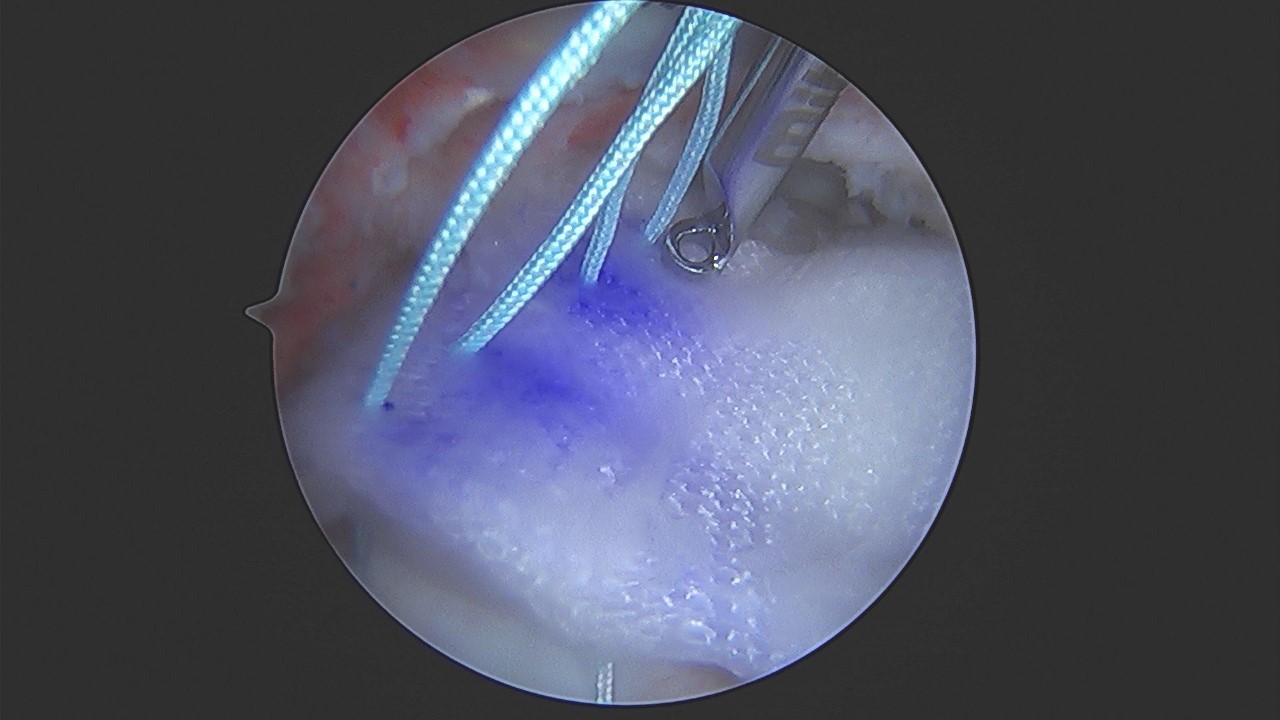
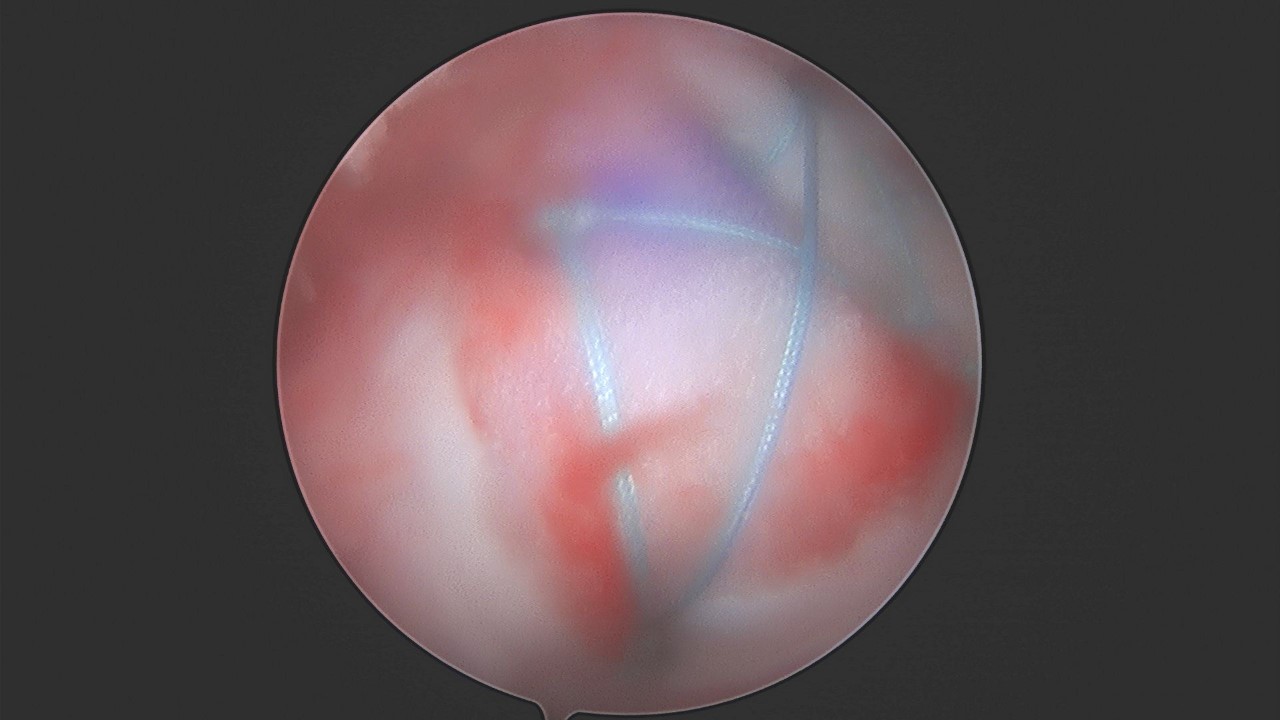
The BioBrace™ can be incorporated into either a single row, double row, or trans-osseous equivalent RCR repair. Once the RCR sutures are passed through the native tissue, the lead authors’ preference is to pass these sutures through the BioBrace™ outside the body through the lateral portal (Figure 4). Passing guns (ESPRESEW®, SCORPION™ etc.) or a simple 18G spinal needle and passing wire (CHIA®) may be used to facilitate suture passage through the scaffold. Given the strength of the implant, the sutures can be placed along the edges as desired. Once suture passing is completed along the medial margin of the implant, it can be delivered into the body by either using a “parachute technique”, a “back grasper” or any standard non-traumatic rotator cuff grasper. A 10mm or 12mm diameter cannula is recommended for passage. Marking the top-side of the implant can prove beneficial for orientation purposes (Figure 5). Once delivered the lateral aspect of the implant can be secured to the greater tuberosity through the lateral anchors Figure 6). In instances of massive cuff tears that require medialization of the footprint to the medial aspect of the tuberosity, the BioBrace™ can be used to both reinforce the repair as well as cover the bare greater tuberosity. In these cases, bone marrow venting of the greater tuberosity will allow for biologic seepage into the implant to potentially allow for enhancement of a “neo-tendon”, as has been shown by Savoie et al. in their work with xenografts (Thon et al. 2019).



DISCUSSION
Rotator cuff repairs are one of the most challenging, yet rewarding, procedures for an orthopedic surgeon. Despite good clinical successes, repeat imaging of these repairs often show sub-optimal healing and or failures (Agrawal 2012; Galatz et al. 2004; Djurasovic et al. 2001; Burkhart et al. 2007). In particular, patients undergoing revision RCR or large to massive repairs, are highly susceptible to recurrent tearing (Agrawal 2012; Galatz et al. 2004; Djurasovic et al. 2001; Burkhart et al. 2007; Gladstone et al. 2007; Miller et al. 2011; Chona et al. 2017).
The addition of RCR’s with graft augmentation has been shown to be beneficial in the literature for these challenging patients (Mirzayan et al. 2019; Bishai et al. 2021a; Bushnell et al. 2021; Barber, Herbert, and Boothby 2008; Barber et al. 2012; Bishai et al. 2021b). Nevertheless, each of the currently available augmentation options has pros and cons. Xenograft bio-inductive implants have demonstrated significant success in the partial thickness RCR cohort (Bishai et al. 2021b). However, the lack of structural strength of the implant is a drawback in the high risk full-thickness tear subset due to its inability to share tensile load at the time of implantation. ADM’s have been shown to provide load sharing ability and decreased failure rates in the literature for high risk patients (Barber, Herbert, and Boothby 2008; Barber et al. 2012). Pre-packaged ADM strips have helped reduce the challenge of delivery of the graft into the shoulder. Despite this, drawbacks exist with ADM’s, including delayed incorporation time to host, inability to differentiate into native host tissue, and the inherent risk of utilizing allograft dermis.
The BioBrace™ is a bio-composite open porous 3D scaffold that allows for augmenting RCR’s through the induction, maturation, and remodeling of new host tissue. This can prevent tissue gapping or re-tears by increasing the thickness of the tendon. Given the strength of the implant, it is able to act as rebar for the suture and help mitigate the risk of suture-tendon pull through. This has long been a known advantage of ADM’s. The ability to combine the benefits of biology and strength into a single implant, while still having the implant resorb overtime, is very appealing. Concerns over the risk of inflammatory response due to the PLLA microfilaments should be tempered at this time due to the relatively low total mass and size within the scaffold. The resorb-able nature of the PLLA microfilaments does induce a mild, localized, foreign body response. However it is minimal and typical of the normal biological response to the degradation of biodegradable material.(Hollinger and Battistone 1986) Walsh et al. similarly found this minimal inflammatory response in their animal model testing without negative outcomes or concern.(Walsh et al. 2021)
The ability to improve RCR outcomes with a bio-composite reinforced implant which allows for increased healing potential and reinforcement of surgically treated tendon holds appeal for many surgeons. The BioBrace™ construct provides a unique environment for soft tissue regeneration and mechanical support which was previously not available for surgeons. Further studies and outcome collections are of paramount importance as this technology moves forward.
Conflict of Interest
The author Ford E declares they have no conflicts of interest. Arciero RA receives educational and research funding from Arthrex and Don-Joy; is a consultant with Biorez and Smith & Nephew. McMillan S is on the scientific advisory board with Biorez, and is a consultant with Depuy Mitek, Arthrex, Smith & Nephew and Trice Medical.
Funding
None