


INTRODUCTION
Knee disorders account for a significant portion of the orthopedic visits to health care providers (HCPs). Symptoms, pain, and functional limitations must be addressed by all stakeholders managing patients throughout the entire episode of knee care (i.e., primary care practitioners, physical therapists, and orthopedic surgeons) (Jordan et al. 2010). While some knee disorders are preceded by a single traumatic event, they are more often attributed to biomechanical pathologic dysfunctions increasing joint stress and leading to pain and functional impairments. In fact, the high prevalence of knee conditions such as anterior knee pain (Loudon 2016; Powers 2003; Manske and Davies 2016) or knee osteoarthritis (OA) (Egloff, Huegle, and Valderrabano 2012) are directly related to abnormal loading and dynamic malalignment (e.g., valgus collapse, varus thrust, flexion contracture).
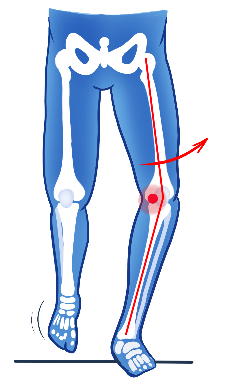
Knee OA is a condition in which faulty knee kinematics is known and recognized as risk factors for disease onset and progression (Sharma, Chang, Jackson, et al. 2017; RACGP 2018; Lane, Brandt, Hawker, et al. 2011). As an example, a patient presenting with a varus thrust, also known as a lateral thrust − which is a quick lateral movement of the knee increasing the varus malalignment − has a four-fold increase in risk for OA progression (Figure 1 and Video 1) (Sharma, Chang, Jackson, et al. 2017). Tackling such underlying improper movement is crucial as patients’ symptoms and satisfaction following conservative and surgical interventions are directly associated with residual unaddressed functional limitations (Rao et al. 2022; Hagemeister et al. 2022).
_during_loading.png)
Although practice guidelines and literature consensus recommend HCPs to assess the presence and severity of biomechanical knee dysfunction, clinicians are faced with a lack of reliable tools (Eastlack et al. 1991; Krebs, Edelstein, and Fishman 1985) to obtain this kind of clinical information in their practice. HCPs predominantly rely on visual observation, or in exceedingly rare cases, on two-dimensional video or clinical gait systems, to assess the knee dynamic behavior. While these methods provide some insight into movement patterns, they are notoriously subjective and may not reliably identify subtle changes required for understanding the exact biomechanical dysfunction and when it occurs (Eastlack et al. 1991; Krebs, Edelstein, and Fishman 1985; Michelini, Eshraghi, and Andrysek 2020). This is particularly true for the frontal/coronal (varus/valgus) and transverse/axial (internal/external rotation) planes, where the magnitude of motion is minimal, and the changes can easily be obscured by the ipsilateral joint. This is concerning as changes in the frontal and transverse planes are known to be particularly important when assessing the risk of OA progression (Sharma, Chang, Jackson, et al. 2017; Miyazaki et al. 2002; Wink, Gross, Brown, et al. 2017; Chang et al. 2004).
Furthermore, there is a need for more advanced medical devices considering that HCPs conventionally base their decision-making process on clinical examination and tools which provide a limited information of the joint behavior. In a case of knee OA, a clinician would evaluate a patient’s lower limb alignment mainly using static Hip-Knee-Ankle (‘HKA’) angles obtained during a visual assessment or with standing X-rays. While radiographs provide useful information on the joint state at a specific instant, this static assessment cannot predict the knee dynamic behavior. Indeed, notable discrepancies were found in a recent study between static X-ray alignment and dynamic alignment behavior during walking (Clément, Blakeney, Hagemeister, et al. 2019). Nearly one-quarter of individuals who demonstrated either varus or valgus alignment based on static X-rays actually exhibited an opposite coronal alignment dynamically (i.e., static varus to dynamic valgus alignment, or vice-versa). Moreover, the study found low to moderate correlations (r=0.266 to 0.553, p<0.001) between static HKA on X-rays and dynamic HKA values for varus knees and no significant correlation for valgus knees, suggesting that static radiographic images do not capture dynamic alignment. Similar results were reported by Deep et al. using a navigation system in the operating room, which confirmed that frontal plane knee deformity changes as it flexes (Deep, Picard, and Baines 2016). Additionally, there is a well-documented discordance between radiographic OA severity and patients’ symptomatology (i.e., pain and function) (Bedson and Croft 2008; Hannan, Felson, and Pincus 2000).
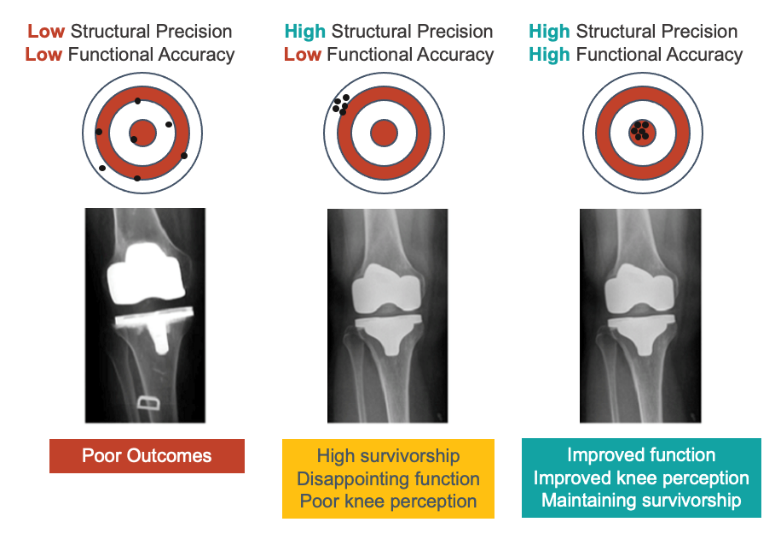
The incapacity to objectively assess knee dynamic behavior during weight-bearing activity greatly limits the support from imaging for surgeons in their decision-making. This limitation is particularly evident in the context of a total knee arthroplasty (TKA) intervention, regarding implant choice, as well as target for alignment and balancing during TKA planning. The current context, wherein up to 20% of patients remain dissatisfied after TKA, calls for the integration of innovative tools in pursuit of personalized medicine. Emerging technologies in the operating room allowed to reduce the role of low structural precision as causal factor of such poor outcomes. Now, there is a need for better functional targets to improve knee function and perception in TKA (see Figure 2). Furthermore, the addition of more objective and functional information may help to learn more about patient experience success or failure of an orthopedic intervention.

Finally, while patient well-being is the core of medical care, patient-reported outcome measures (PROMs) from questionnaires may present limitations in some cases. They are fundamentally subjective and can be unequally dependent on patient expectations, feelings towards an HCP, education, and health literacy. Moreover, these questionnaires were designed to assess cohorts of patients, rather than individual patients. At the more positive end of health state scale, ceiling effects can also be observed which limits the room to detect any possible improvements at higher functional levels. As PROMs do not constitute actionable data and, therefore, cannot guide therapeutic interventions, it becomes urgent to access purer patient-specific information, to better understand knee function and support clinical decision-making.
Performing an accurate, reliable, and objective three-dimensional (3D) knee kinematic assessment in clinical settings has proven to be a complex task. University research gait laboratories have been used to achieve the required accuracy, reproducibility, and reliability to identify and quantify the biomechanical dysfunction linked to knee pathologies, injuries, or other forms of pain. However, accessing these laboratories is limited, costly and time consuming for both the patient and HCP. While there are emerging technologies to evaluate biomechanical dysfunctions in clinical settings (i.e., marker-based systems, inertial units, mobile apps, etc.) none have shown the required accuracy, reproducibility, and reliability necessary to be used in the diagnostic or prognostic aspects of patient care or surgical planning.
The KneeKG® system is a portable, validated, FDA (510k) cleared, Health Canada Licensed and CE Marked medical device, capable of assessing the 3D knee motion for patients who have impaired movement functions of an orthopedic cause (Sati et al. 1996; Labbe et al. 2008; Südhoff et al. 2007; Ganjikia et al. 2000). This procedure, described as the Knee Kinesiography exam, provides HCPs with accurate, reliable, and real-time information about dynamic malalignment and biomechanical dysfunction through the assessment of kinematic biomechanical markers (i.e., varus thrust, dynamic flexion contracture, etc.). In contrast to conventional tools, this assessment provides objective patient-source outcome measures (PSOMs), on the knee dynamic alignment behavior, helping HCPs (i) to identify mechanisms behind the knee orthopedic pain or the mechanical changes after knee injury, and (ii) assist them in their decision-making to establish the best possible care plan (Schraeder, Terek, and Smith 2010; Calmbach and Hutchens 2003).
Building upon a 2012 review (Lustig et al. 2012) which summarized studies reporting technical validations of this exam, numerous subsequent studies have been conducted to assess its impact on clinical gaps in the management of knee OA. This work aims to present a comprehensive review of the clinical materials related to this exam which have been published since 2012. The objective is to enhance our understanding of how the Knee Kinesiography exam may improve both the non-surgical and surgical management of knee OA and TKA. Every study related to the use of the Knee Kinesiography exam or the KneeKG® system was considered. Clinical materials included data on adults (aged 16 or over) with knee osteoarthritis or matched asymptomatic/healthy controls from MEDLINE by PubMed, PubMed Central, ResearchGate, and Google Scholar databases. The review settled no restriction for the inclusion on studies based on the type of reported intervention but was limited to original research article, guidelines, reports, and conference abstracts. Letters, websites, and blogs were excluded. This review will present the system and its related approach, summarize the clinical literature related to their impact on the non-surgical and the surgical management of knee OA, and describe their health economical impacts.
THE KNEEKG® SYSTEM
The KneeKG® system assesses and quantifies the loaded knee joint motion in the sagittal (flexion and extension), frontal (varus and valgus), and transverse (internal and external rotation) planes while the patient is walking on a conventional treadmill. The exam begins with the placement of an exoskeleton fixed on the patient’s knee with respect to bony landmarks. A brief calibration process, which is very similar to the registration process of surgical navigation or robotic-assisted systems, is then conducted. Ankle, knee, and hip joint centers are calculated from a combination of anatomical landmarks identification and functional movements, known as the functional and postural method (Hagemeister et al. 2005). This is a critical component for obtaining accurate 3D joint kinematics (Kadaba, Ramakrishnan, and Wootten 1990). After approximately 10 minutes of patient preparation (described above), the actual exam, which involves familiarizing with treadmill walking at a self-determined comfortable pace while wearing the exoskeleton, and data capture process take about 5 minutes. At this stage, real-time knee motion is available and displayed in 3D on a monitor (Figure 3 and Video 2).

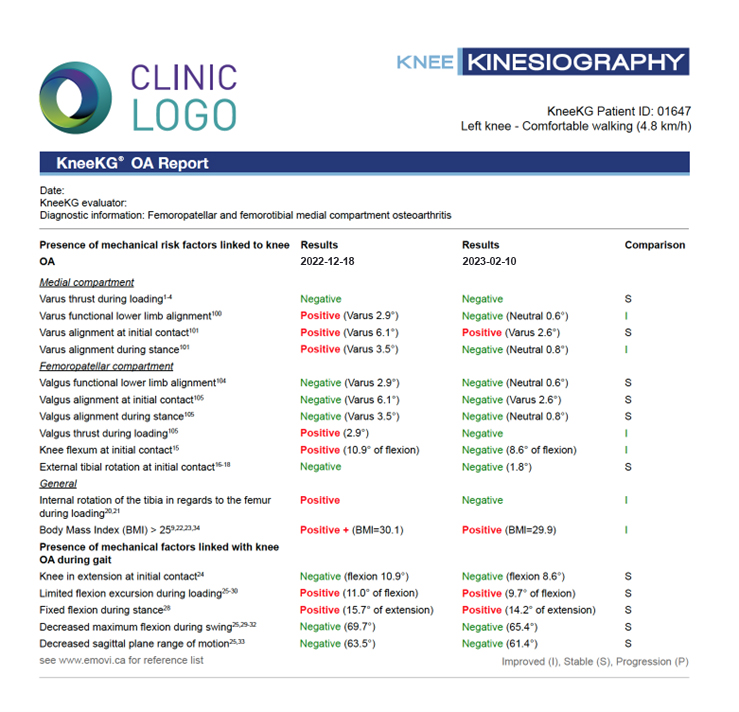
A 45-second walking recording is used to assess the presence of any potential biomechanical dysfunctions through kinematic biomechanical markers which are known to be associated with joint pain and/or OA progression, such as varus thrust (Sharma, Chang, Jackson, et al. 2017; Wink, Gross, Brown, et al. 2017; Chang et al. 2010) and reduced knee flexion excursion (Zeni et al. 2018). Such markers are automatically identified and quantified based on cut-off values obtained from the literature, and accessible through an automated report (Figure 4). This allows clinicians to better understand the specific features of the knee dynamic behavior which may play a role in the deterioration of the joint and to objectively monitor patients’ evolution during follow-up assessments to better understand the impact of their intervention.

Although traditional motion capture systems can assess knee joint kinematics, the results are challenged by movement artifacts from soft tissues upon which the reflective markers are attached to. This leads to significant inaccuracy and limitations in data reliability and reproducibility, similarly to marker-less solutions. Furthermore, some provide incomplete information as they do not assess joint kinematics in the three planes of movement (e.g., inertial sensors or marker-less technologies). As highlighted in the 2012 literature review (Lustig et al. 2012), the KneeKG® addresses these technical limitations. More specifically, all three planes of motion are quantified with an accuracy of 0.4° for adduction/abduction (varus/valgus), 2.3° for axial rotation (tibial int./ext. rotation), and 2.4 mm for AP translation (Sati et al. 1996). In this 2012 review, intra- and inter-rater reproducibility were reviewed (met or exceeded 0.8 ICC values) (Labbe et al. 2008), and differences in intra- and inter-rater reliability for joint angles were less than 1° using the functional and postural method. The KneeKG® system was also tested in a high body mass index (BMI) patient population which demonstrated its ability in reducing skin motion artifact to ensure accurate data (Lustig et al. 2012). The researchers found that soft tissue artifact, when using the validated exoskeleton, was minimal across body types. It was even lower in the obese patients, suggesting that the KneeKG® approach may be suited for patient populations known to have greater body mass indexes (e.g., knee OA patients).
The space requirements for performing a Knee Kinesiography exam are similar to the volume occupied by most clinical treadmills (which is about 10x12 feet). A comprehensive technical and clinical training is required to acquire the expertise to collect reliable objective results with the KneeKG® medical device and to interpret the outcomes. A certification must be obtained to use collected data in the diagnostic or prognostic aspects of patient care or surgical planning. While performing the procedure is resource consuming, physician assistant, physical therapist, athletic trainer, radiology technologists, nurses or other HCPs can be trained. Furthermore, the actual time required to complete the exam and the training are low compared to tools used in clinics such as electrocardiogram, echography, and others, making it easier to implement into a clinical, hospital or imaging center setting.
ENHANCING THE CLINICAL MANAGEMENT OF KNEE OSTEOARTHRITIS
Non-surgical Care
The relevance of PSOMs from the Knee Kinesiography exam to better understand and manage knee OA has been supported by clinical studies through the past ten years. Biomechanical studies, including those using the KneeKG®, have consistently revealed that patients with knee OA present with biomechanical dysfunctions compared to age-matched healthy controls (Zeni and Higginson 2009; Bytyqi et al. 2014). Patients having or at greater risk for developing symptomatic knee OA can be objectively identified in clinical settings by the assessment of dynamic malalignment in the three planes of movement (Sharma, Chang, Jackson, et al. 2017; Lane, Brandt, Hawker, et al. 2011; Chang et al. 2010). As established in a recent study (Bensalma, Hagemeister, Cagnin, et al. 2022), dynamic PSOMs from the Knee Kinesiography exam can complement the physical exam and imaging findings to establish a more comprehensive knee functional profile. This cross-sectional study with 415 patients (251 women and 164 men) showed that the PSOMs (i.e., biomechanical markers) were associated with PROMs, especially with pain and function, to a greater extent than OA radiographic severity grading (Bensalma, Hagemeister, Cagnin, et al. 2022).
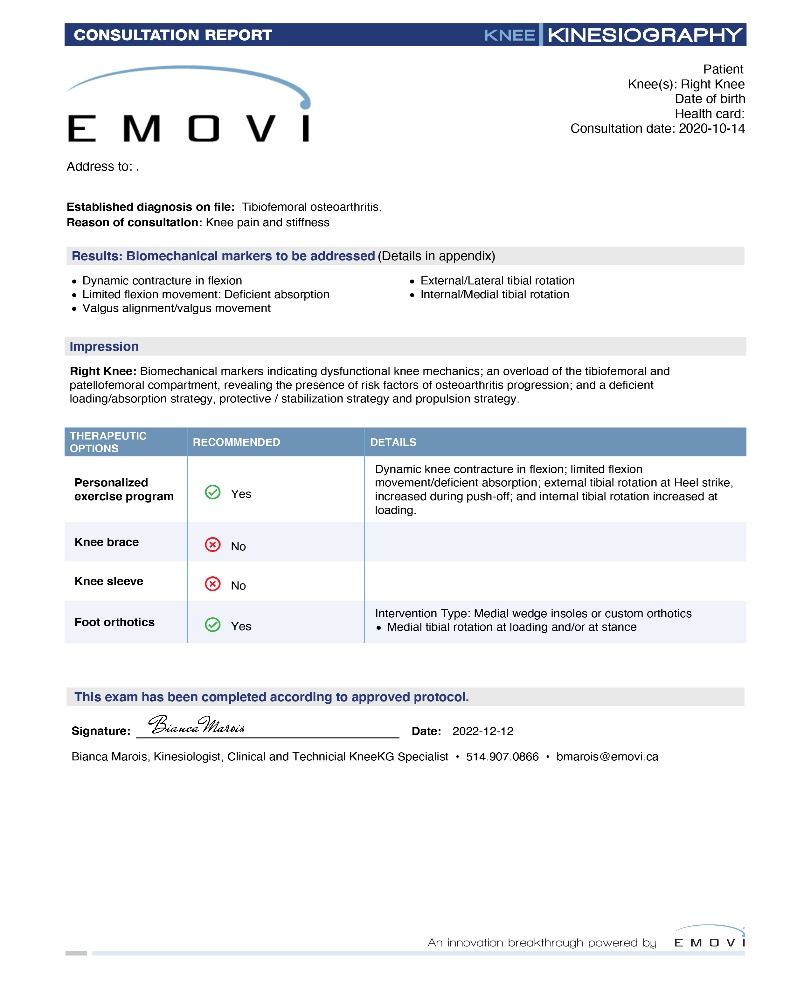
This clinical validation helps partially explain the findings of a large (i.e., N=515 patients) randomized controlled trial (RCT) which evaluated the clinical benefit of adding a Knee Kinesiography exam within knee OA episode of care (Cagnin, Choinière, Bureau, et al. 2019, 2023). Indeed, results showed at the 6-month follow-up that OA patients who received a conservative targeted program based on individual PSOMs from the Knee Kinesiography exam demonstrated statistically and significantly more pain relief and further improvement in function and satisfaction compared to the control group who followed standard of care (Figure 5). Clinicians in the intervention group benefited from the Knee Kinesiography report that not only highlighted the patient-specific dysfunctions but also provided therapeutic recommended measures to address them (Figure 6). Indeed, recommendations about specific bracing, orthotics, and home exercises are provided to the HCP to help them define the most valuable mechanical intervention to address the patient condition.


Furthermore, patients who benefited from targeted neuromuscular exercises addressing the identified PSOMs successfully changed their knee dynamic behavior through different biomechanical markers’ correction (i.e., varus thrust, flexion contracture and excessive tibia rotation at initial contact) (Cagnin et al. 2022). The education material and exercises were made available to patients on a web platform and were adapted to be integrated into their daily activities to increase the uptake (Figure 7 and Video 3). The valuable benefits in patient education made possible by the integration of the Knee Kinesiography exam within the knee OA continuum of care was recognized in the recent American Association of Orthopaedic Surgeons (AAOS, 3rd edition) practice guidelines (American Academy of Orthopaedic Surgeons 2021) for non-surgical knee OA management. While orthopedic surgeon training focuses on surgical interventions, as it should, the clinical reality is that a lot of time is also spent in the clinic where there is a significant clinical knowledge gap related to non-surgical interventions. As individualized conservative care should be preconized for each patient, the Knee Kinesiography exam could help fill this gap.

Beyond the additional information useful to develop effective correctives, PSOMs assessed by the KneeKG® also showed to provide valuable input in artificial intelligence (AI) tools to better characterize patient function, understand success or failure of interventions, and support decision-making. A recent study which used PSOMS from the KneeKG® with AI and machine learning (M. Mezghani and et al. 2021) approach showed that data were sensible enough to predict the impact of OA patients’ response to a treatment consisting of a physical exercise program. In addition, PSOMs from the KneeKG® also allowed to successfully identify distinct kinematic phenotypes using AI approach both in the healthy and pathologic populations (N. Mezghani and et al. 2021; M. Mezghani and et al. 2022), reinforcing the intrinsic value of these objective data to help clinicians in their decision-making process.
Furthermore, a study reported that such PSOMs could support HCPs in the decision of when a patient is appropriate for surgery. It is generally accepted criteria for TKA surgical candidacy that the patient should have end-stage radiographic OA and exhausted conservative treatment options for the pain and symptoms. The PSOMs can be used to assist clinicians by providing objective data through a triage tool integrated within the KneeKG® system compared with radiographic features unrelated to patients’ symptoms and function. It is based on an AI classification model using PSOMs as inputs reaching an accuracy of 85% (80% sensitivity and 90% specificity) to discriminate patients who are deemed candidates for TKA and those who were not compared to the decision of experienced orthopedists (M. Mezghani et al. 2016). Clinicians can then use the automatic suggestion based on PSOMs describing the knee dynamic behavior to help them choose and document the type of approach (i.e., conservative or surgical) to recommend for the patient.
Surgical Care
Emerging technologies for the past years have allowed surgeons to achieve higher precision in the measure of parameters of interest in TKA planning and in the operating room. However, there is a shared objective within the orthopedic community to attain higher accuracy in the surgical episode of care to improve clinical outcomes. Lack of functional assessment tools makes it difficult to define optimal and personalized targets for alignment, implant choice, and gap balancing. This lack of functional data to assist surgeons in their decision-making, especially during surgical planning, may partially explain why up to 20% of patients remain dissatisfied post-surgery (Tanzer and Makhdom 2016). Surgeons often rely on static imaging to define intervention targets although it provides incomplete information of the knee function. For example, radiographic measures, such as arithmetic HKA and joint line obliquity, were shown not to be associated with 3D kinematics before nor after TKA (Hagemeister et al. 2023). This is even more important as abnormal knee kinematics are directly linked with implant survivorship and are the main cause of residual pain post-surgery in up to 40% of patients (Michalik, Rath, Springorum, et al. 2016), which can ultimately lead to costly revision surgery.
While standard of care aimed for a neutral mechanical lower-limb alignment for the past decades, different schools of thoughts have arisen in the hope to achieve optimal patient satisfaction levels and TKA outcomes. Several authors suggested that alignment targets should be based on 3D/4D data, supporting concepts like kinematic alignment and functional alignment (Oussedik et al. 2020). In pursuit of personalized TKA approaches, some authors explored patient phenotyping in terms of bone (MacDessi et al. 2021) or ligamentous (Graichen et al. 2022) morphology to gain better understanding of the patient’s condition prior to surgery. Notably, Bensaddek et al. demonstrated that phenotyping OA patient could be achieved based on different kinematic 3D profiles identified from Knee Kinesiography measures (Bensaddek et al. 2023). A combination of morphological, functional, and kinematic data may eventually help define individualized alignment target and contribute to achieving better outcomes including higher satisfaction levels.
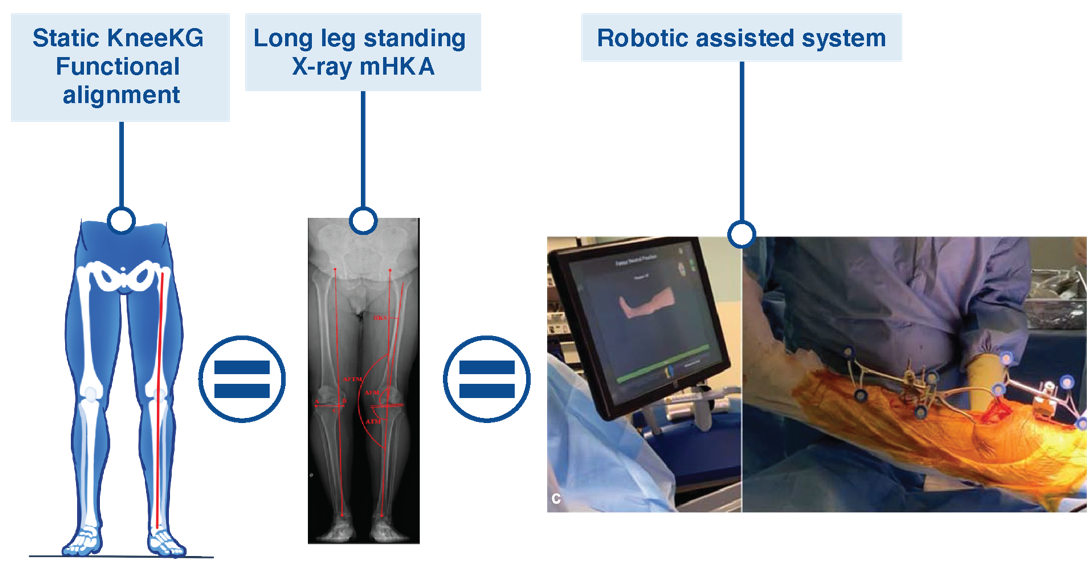
Understanding that PSOMs obtained from the KneeKG® correlate with conventional surgical measures of interest, such data can provide valuable support to orthopedic surgeons in their surgical planning. Notably, the literature search revealed an initial study, demonstrating that a frontal plane alignment measure from the KneeKG® (i.e., at maximum knee extension during gait) closely align with measures obtain from a surgical robot in the operating room (Deroche et al. 2022) (Figure 8). A subsequent study confirmed the equivalence between mechanical HKA and the static functional HKA defined during the functional and postural registration process at the beginning of the Knee Kinesiography exam (Landry et al. 2023). Moreover, the KneeKG® is going a step further by defining additional dynamic dysfunctions that could be of interest in surgical planning. These include the varus thrust, dynamic knee flexion contracture, hyperextension, and the behavior of the frontal plane alignment during dynamic task (i.e., is the malalignment increasing, decreasing, or even crossing over from valgus to varus or vice versa, is the malalignment constitutional or instability related, etc.). The assessment of these PSOMs pre-surgery may help surgeons in their decision process to find the right balance target as they are associated with excessive soft tissue contractures.

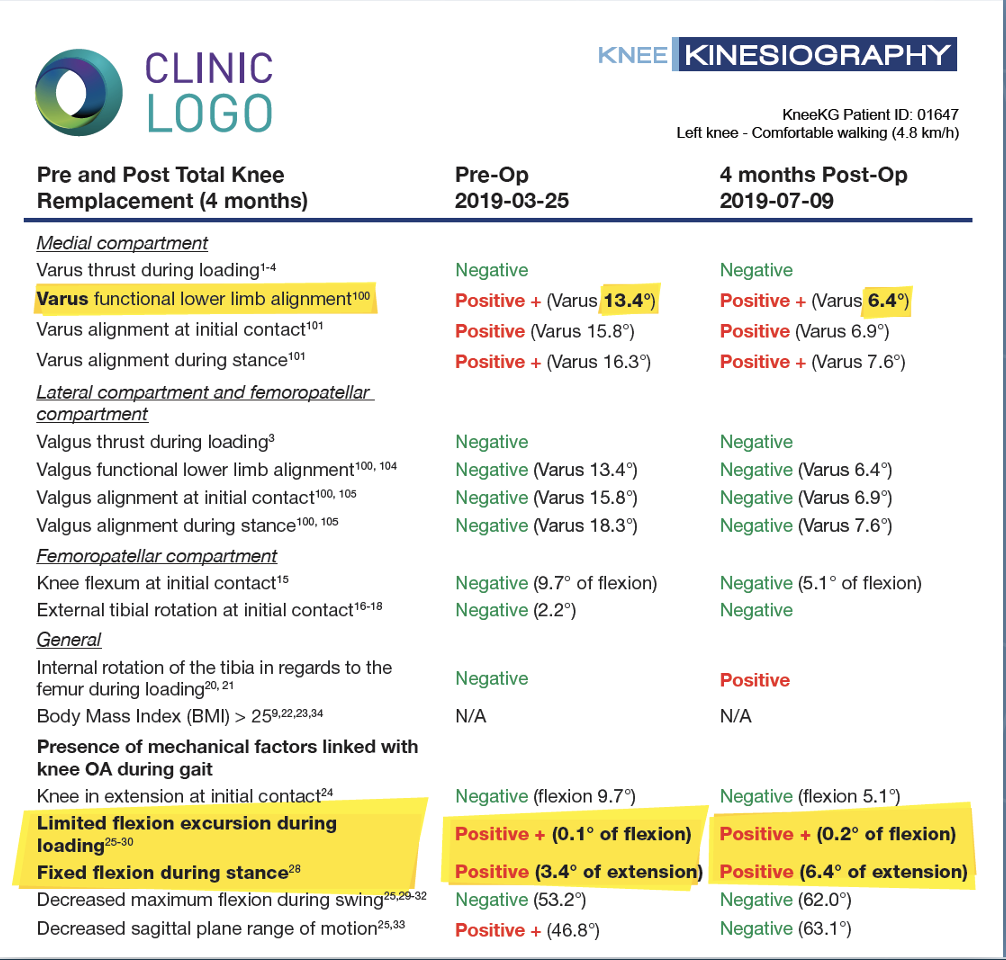
The example below illustrates the added value of the PSOMs obtained from the KneeKG® to better understand and document poor outcomes post-surgery. In this case of a patient presenting with residual pain post-TKA, static imaging confirmed the absence of prosthetic loosening or components malpositioning, which are known factors for surgery failure. The Knee Kinesiography report confirmed the successful correction of the lower limb functional varus alignment with the surgery (from 13.6° pre- to 6.4° post-operatively; Figure 9). Importantly, the report also highlights the persistence of certain biomechanical dysfunctions post-surgery that were present pre-operatively (i.e., dynamic flexion contracture during loading and stance phases). These PSOMs are known to be linked to residual pain post-surgery, supporting the clinician in differentiating the cause of poor PROMs post-surgery. It was determined that these results were not directly associated with the surgery itself, but rather with post-surgery biomechanical dysfunctions that persisted from the pre-surgery knee functional state. Addressing these dysfunctions through post-operative rehabilitation was deemed necessary.

This example illustrates how dynamic functional PSOMs could contribute to reducing the dissatisfaction rate post-TKA. Multiple studies have shown how PSOMs are directly correlated with PROMs, especially pain and function, and satisfaction levels after TKA (Hagemeister and et al. 2023; Fuentes et al. 2022). A study by Hagemeister et al. (2023) showed that patients presenting with a varus thrust post-TKA surgery were associated with significantly worse function 1-year post-TKA (Hagemeister and et al. 2023). Interestingly, other biomechanical markers in the frontal plane post-surgery, more specifically alignment behavior at heel strike and during stance, as well as flexion contracture during stance, are related to patient satisfaction levels post-TKA (Fuentes et al. 2022). Other authors have also reported that the same measures post-surgery allowed to identify significant differences in knee function between a cohort of patients reporting painful TKA versus a cohort of asymptomatic TKA (Planckaert et al. 2018; Kirschberg et al. 2018). Interestingly, and as previously reported in this review, other studies showed that these same biomechanical markers can be corrected through a conservative KneeKG-based treatment approach (Cagnin, Choinière, Bureau, et al. 2023; Cagnin et al. 2022). It can be argued that employing such targeted approach to address residual biomechanical dysfunctions in post-TKA rehabilitation could be beneficial in alleviating dissatisfaction among patients. As unrealistic expectations constitute another important factor of dissatisfaction post-surgery, PSOMs obtained from a Knee Kinesiography pre-surgery could be relevant to educate patients about their dysfunctions and help them set realistic expectations about surgery. The positive impact of education based on KneeKG results has been highlighted in the RCT study recognized in the AAOS guidelines as strong evidence for patient education programs (Cagnin, Choinière, Bureau, et al. 2019, 2023; Cagnin et al. 2022; American Academy of Orthopaedic Surgeons 2021). While additional comparative studies may help demonstrating the positive impact of integrating such data in pre- and post-surgical management on patient dissatisfaction rate, reported data support its potential to bring valuable benefits to surgeons, assisting them to achieve higher patient satisfaction and function.
THE HEALTH ECONOMICAL IMPACTS OF THE KNEEKG® APPROACH
Optimizing Care for Costs Reduction
In 2019, Milliman Inc., an independent, international actuarial and consulting firm in the healthcare, insurance, and financial markets, conducted an analysis of US payer healthcare expenditures and utilization of healthcare services to address knee OA in the commercially insured population (18-64-year-olds) (Fitch et al. 2020). The white paper, titled “Knee Osteoarthritis in a Commercially Insured Population: A Claims-Based Analysis.” examined the annual diagnostic and therapeutic patterns for patients with symptomatic knee OA and the impact it has on healthcare insurance costs.
“The cost burden of knee OA is high among the US commercially insured working age population. Many existing treatments to manage the progression and/or reduce the symptoms of knee OA are expensive and have questionable efficacy. There is evidence of overutilization of certain tests and treatments for knee OA in the US. This claims-based analysis identifies knee OA diagnostic and treatment patterns that may highlight opportunities for improving the efficiency of managing this chronic condition.” (Fitch et al. 2020)
Key findings in the snapshot analysis revealed a knee OA prevalence rate of 1.97% with an average annual healthcare knee OA patient spend ~3 times the cost of an average adult plan member. Of the $17.6K average annual insurance spent per knee OA patient in 2017, nearly 31% of those costs were attributed to knee OA-related services such as imaging, physical therapy, hyaluronic acid injections, and knee arthroplasty. More specifically, over 80% of the knee services spend was associated with knee arthroplasty at 62%, while 10% was associated with arthroscopy and minor knee surgery, and 9% associated with knee injections (e.g., hyaluronic acid, steroid).
While payers push back on diagnostic imaging as the sole source for treatment planning, the use of quantifiable PSOMs from the KneeKG® fit the value based care models and may bring societal and economic benefits by optimizing knee care and reduce unnecessary treatments or procedures. Incidentally, the 2019 RCT evaluating the impact and efficiency of integrating the KneeKG® in the knee OA conservative continuum of care reported clinically significant improvements for patients in terms of pain and function in less than 3 sessions with an HCP compared to a minimum of 12 to 18 physical therapy sessions in care programs with similar results (Cagnin, Choinière, Bureau, et al. 2023). Considering that the improvement of their global condition can go hand in hand with a reduction in use of medication (Therrien et al. 2016), the use of PSOMs obtained from the KneeKG® could help making a difference reducing patient costs.
The triage tool integrated in the KneeKG® system to assist clinicians in their decision of when a patient is appropriate for surgery is another example of possible care and cost optimization. A study at Dalhousie University (Halifax, Nova Scotia, Canada) evaluated the impact of utilizing the KneeKG® system in the patient care pathway to improve the actual surgical referral decision process (Kenny et al. 2017). The study evaluated the subsequent downstream impact on the health system with respect to resources and economic outcomes. The modeling analysis found that incorporating an assessment with the KneeKG® system prior to surgical consultation 1) reduced the amount of TKA demands, 2) reduced by approximately 24% the number of patients who were inappropriately referred to a surgeon, and 3) provided an initial cost-savings to the healthcare system of just over 6% per patient.
Interestingly, these benefits did not include the potential cost-savings attributed to delaying the need for TKA through appropriate correctives, nor potential cost-savings attributed to a reduction in the number of revision surgeries. These aspects were suggested in a 2016 study in patients on a waiting list for TKA (Therrien et al. 2016). Following a significant improvement in function and a reduction in the need for daily pain medication in patients following a PSOMs KneeKG® driven therapeutic approach, 7 of 11 patients (63%) who were originally on the waiting list for TKA, delayed their surgery. These aspects are decisive considering that TKA was the biggest contributor to knee OA-related costs in 2017, contributing 62.4% of the total knee OA related spending. Nonetheless, longitudinal studies following patients for several years are needed to rigorously evaluate the possibility of reducing the need for revisions.
Implementing the KneeKG® System in Orthopedic Practices
The KneeKG® is already available in hospitals, clinics, and imaging centers, and it can easily be included in the conventional toolset of HCPs. Practices utilizing the KneeKG® in the United States report reimbursement for the procedure using established Current Procedural Terminology (CPT) codes (e.g., 96000 and 96004) with reimbursements ranging between $200 and $380 per exam depending on the payer. Since the launch of the KneeKG® into the market, HCPs have submitted insurance claims to both public and private payers, presenting opportunities to educate them on the unmet clinical need and clinical benefits the technology provides. This resulted in positive payer reimbursement for the KneeKG® by third party payers to include but not limited to Medicare (i.e., in the US), Government, National, and Regional healthcare insurers.
The implementation process for onboarding a KneeKG® System into a site of care is simple and straightforward. It starts with an implementation meeting with all stakeholders, allowing to go over all key aspects of a successful implementation (i.e., space required, treadmill specifications, information technology (IT) checklist, etc.). All training can be complete within 3 weeks with on-line support. The training starts with a 60-minute online session as an introduction to the KneeKG® System for those who will test patients, as well as for clinicians who will interface with the reports. Once the KneeKG® unit is received at the site of care, a one-hour virtual meeting is organized to unbox and setup the system. All the equipment is checked to ensure readiness for training. The virtual technical training covering the step-by-step protocol for testing patients consist of online sessions (total of 6 hours) for the technicians who will be doing the testing. Often, trainees are medical assistants (MAs), athletic trainers (ATCs), kinesiologists, physical therapist (PT) assistants, or other technicians, and after practicing on 10-15 knees, they certify on the protocol. This ensures high-quality, reproducible results in their data, for accurate patient reports. A trained staff is available for support throughout the process and as patient testing begins.
Limitations and challenges
While this work primarily focused on presenting a comprehensive review of how the Knee Kinesiography exam could enhance the management of knee OA and TKA, it is important to acknowledge a few limitations and challenges. Although the exam is relatively quick to conduct (i.e., approximately 15 minutes), it still requires a resource to complete the procedure. This resource can be a medical assistant, athletic trainer, or PT assistant to mitigate the cost related to this technical procedure. With staff limitations and increased workload at site of care, some clinics may find it challenging to allocate resources for operating new technologies. Furthermore, there is a non-negotiable timeframe during which the allocated resources must undergo clinical and technical training to obtain certification for conducting the examination. This training process may extend over several weeks. While it is key to the process to guarantee the quality of the data collected, this aspect should be considered carefully before contemplating the implementation of the system in an orthopedic practice. While using a conventional treadmill to collect data may be perceived as a limitation since walking might not be a strenuous activity, it allows a good reproducibility of the data, and less space is required. The majority of patients can undergo the exam, but it should be noted that those relying on walking aids, exhibiting extremely limited flexion range of motion (i.e., <10°), or walking at a very slow speed (i.e., <0.7 mph) may not be able to complete the exam. Such patients could follow a reconditioning program designed to help them improve their overall function before performing a Knee Kinesiography.
Beyond these limitations, the deployment and use of this exam at a larger scale confronts challenges comparable with the ones faced by other disruptive technologies. Foremost among these are issues pertaining to compliance, security, rigorous clinical validation, and interoperability, which have been successfully addressed in the past twenty years, leaving such deployment with two remaining challenges, namely workflow integration and resistance to change. While the variability among different care sites invites to conduct specific comprehensive risk assessments, it is also the responsibility of the orthopedic community and its stakeholders to proactively address these challenges to ensure the success of innovation implementations.
CONCLUSION
This comprehensive review shed the light on how a Knee Kinesiography exam can provide objective functional insight about knee dynamic behavior, complementing information from conventional tools and establishing an accurate knee functional profile. The in-clinic access to objective patient-source outcome measures contributes to its growing adoption by clinicians to assist them in the conservative and surgical management of patients with knee osteoarthritis. This approach has the potential to bring significant benefits by improving health and guiding clinicians towards a more value-based care practice. While the added value of the patient-source and reliable data from the KneeKG® has been demonstrated throughout the osteoarthritis continuum of care, they also have many applications in other knee pathologies. The use of the Knee Kinesiography exam for anterior-cruciate ligament injuries, meniscal tears, patellofemoral pain syndrome as well as applications in professional athletes’ care will be detailed in a future article. The implementation of the Knee Kinesiography exam can have a positive impact on the decision-making at patient-level, practice-level, and in terms of population-health and savings both in healthcare resources utilization and healthcare system costs.