.jpg)
INTRODUCTION
Knee osteoarthritis is a debilitating condition affecting millions of people worldwide, causing pain, limited mobility, and reduced quality of life. While numerous treatment modalities have been explored, the management of knee osteoarthritis remains a complex challenge. However, recent advancements in pain management techniques have shown promising results, and one such approach gaining attention is cryoneurolysis (Malik et al. 2023).
The knee and knee capsule are innervated by a plenitude of sensory nerves. Cryoneurolysis has already demonstrated positive outcomes in knee osteoarthritis pain by treating the infra-patellar branch of the saphenous nerve (Radnovich et al. 2017). In addition, multiple studies have shown significant reduction in post operative knee pain following total knee arthroplasty with cryoneurolysis of the anterior femoral cutaneous nerve and infra-patellar branch of the saphenous nerve (Urban, Dolesh, and Martin 2021; Plessl et al. 2020; Mihalko et al. 2021; Dasa et al. 2016). Similarly, the deep genicular nerves are well established in literature as primary sensory innovators of the knee - specifically the superior medial genicular nerve, superior lateral genicular nerve, and inferomedial genicular nerve - and are the primary targets for other modalities of nerve modulation, such as radiofrequency ablations of the knee (Conger et al. 2021). Therefore, both the superficial and deep genicular nerves together play a crucial role in innervating the knee joint and have been implicated in the pathogenesis of knee osteoarthritis related pain.
Cryoneurolysis involves the use of extreme cold temperatures between -20 degrees Celsius to -100 degrees Celsius to selectively degenerate the axon and myelin sheath of peripheral nerves, providing temporary pain relief by interrupting the pain signal transmission. This technique has been successfully employed in various orthopedic and non-orthopedic applications (Radnovich et al. 2017; Urban, Dolesh, and Martin 2021; Perry and Segal 2022; Grigsby, Radnovich, and Nalamachu 2021), and its potential in treating knee osteoarthritis pain is being explored with growing interest due to its localized mechanism of action and minimal contraindication to therapy. Cryoneurolysis is contraindicated for use in patients with cryoglobulinemia, paroxysmal cold hemoglobinuria, cold urticaria, Raynaud’s disease, and open and/or infected wounds at or near the treatment site. Potential complications and side effects of treatment include but are not limited to ecchymosis, edema, erythema, local pain and/or tenderness, and localized dysesthesia.
Interestingly, despite these known findings, there remains a lack of published research specifically targeting the comprehensive treatment of both the superficial (anterior femoral cutaneous nerve and infra-patellar branch of the saphenous nerve) and the deep genicular nerves (superior medial genicular nerve, superior lateral genicular nerve, and inferomedial genicular nerve) for knee osteoarthritis pain, nor does there exist literature of the effectiveness of repeat therapies in humans (Hsu and Stevenson 2014).
This case study aims to bridge this knowledge gap by presenting a comprehensive treatment approach utilizing cryoneurolysis for both deep and superficial genicular nerves in a patient suffering from knee osteoarthritis pain as well as demonstrate the efficacy of subsequent repeat cryoneurolysis treatments. The case study demonstrates the effectiveness and outcomes of this innovative intervention, shedding light on the potential benefits and challenges associated with this novel treatment modality.
CASE REPORT
A 65 year-old-male with past medical history of hypertension and Kellgren-Lawrence grade 2-3 tricompartmental bilateral knee osteoarthritis was referred to our clinic with complaints of persistent and debilitating arthritic like complaints of the bilateral knees refractory to conservative treatment for over 1 year. Previous conservative treatment consisted of activity modification, formal physical therapy, oral anti-inflammatories, intraarticular corticosteroid injections and viscosupplementation injections, all of which provided very limited and temporary relief. On initial referral, he noted 8/10 pain bilaterally that interfered with his very active lifestyle. Specifically, this patient competed in various Senior Olympics track events and his pain was limiting his participation. Despite the repetitive impacting nature associated with these activities, he enjoyed participating in them and desired to resume participation. On discussion regarding further treatment options, he was not interested in utilizing orthobiologics or pursuing definitive treatment with total knee arthroplasty. The patient was looking for alternative nonoperative treatment options and thus was subsequently referred to our clinic for consideration of cryoneurolysis.
The patient had a past medical history of hypertension managed by oral antihypertensives and a past surgical history consisting of bilateral hip resurfacing. Otherwise, his history was unremarkable with no significant family history. The patient reported being very active and he exercised regularly as described previously. He denied tobacco or illicit drug use and reported no known drug allergies. His other home medications included meloxicam for his knee pain, which was no longer providing him with adequate relief.
CLINICAL FINDINGS
On physical exam, the patient ambulated with a nonantalgic gait. He had a normal body habits with a BMI of 28.5. His bilateral knees revealed a 1+ effusion with a mild varus deformity. Active and passive knee range of motion was 0-110 degrees bilaterally with crepitus and mild to moderate pain with terminal extension and hyperflexion. There was tenderness to palpation about the medial and lateral joint lines bilaterally with a negative McMurray’s test. There was no evidence of cruciate or collateral instability. There was no erythema or evidence of infection and his skin was unremarkable. His bilateral lower extremities were neurovascularly intact.
DIAGNOSTIC ASSESSMENT
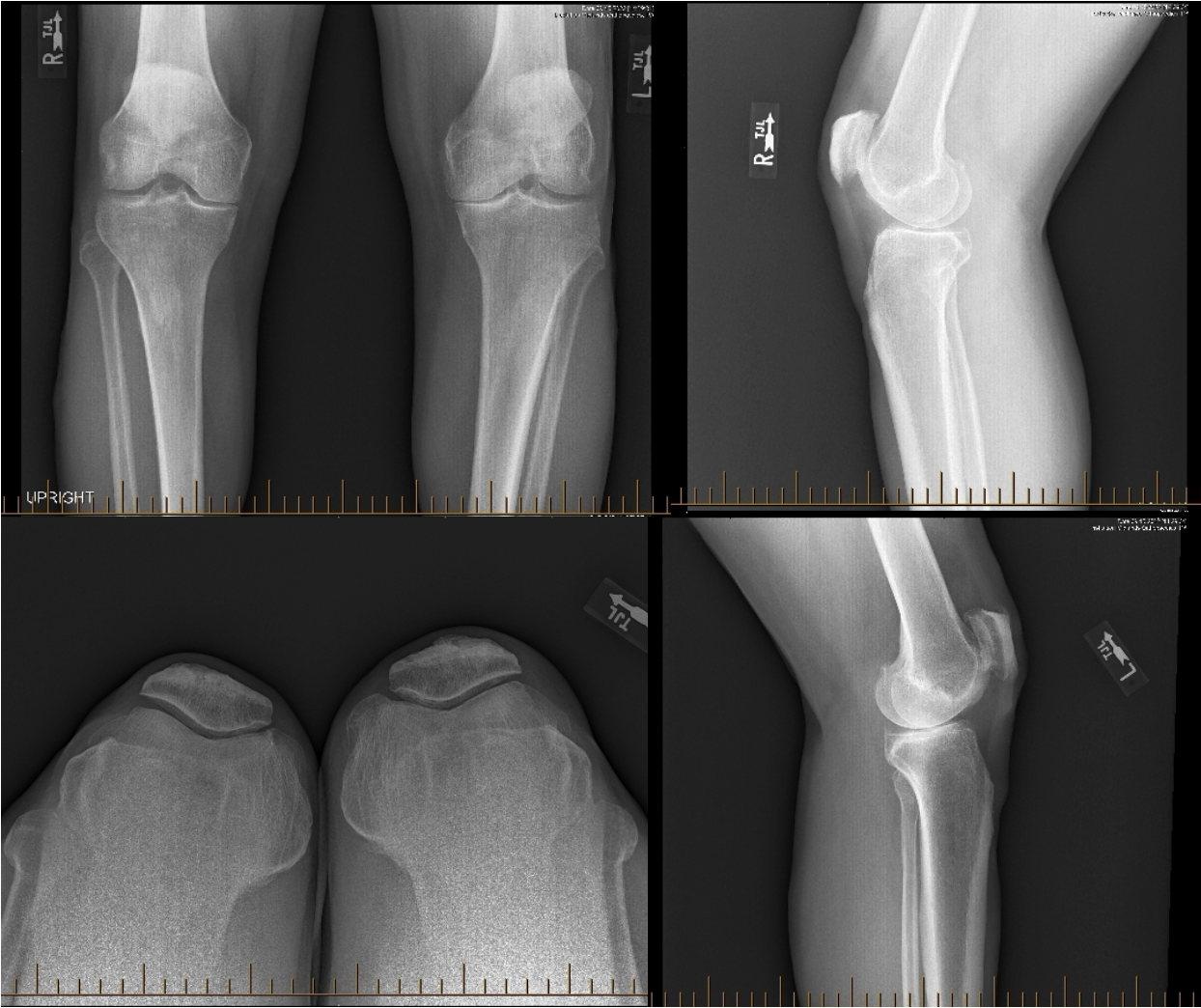
Three view weight-bearing radiographs of the left knee revealed Kellgren-Lawrence grade 3 osteoarthritis with significant joint space narrowing of the medial compartment and moderate joint space narrowing of the lateral and patellofemoral compartments. There is osteophyte formation noted tricompartmentally, most pronounced at the medial and patellofemoral compartments. No fracture was present.
Three view radiographs of right knee revealed Kellgren-Lawrence grade 2 osteoarthritis with moderate tricompartmental joint space narrowing. There is osteophyte formation noted tricompartmentally, most pronounced at the patellofemoral compartment. No fracture was present.

THERAPEUTIC INTERVENTION
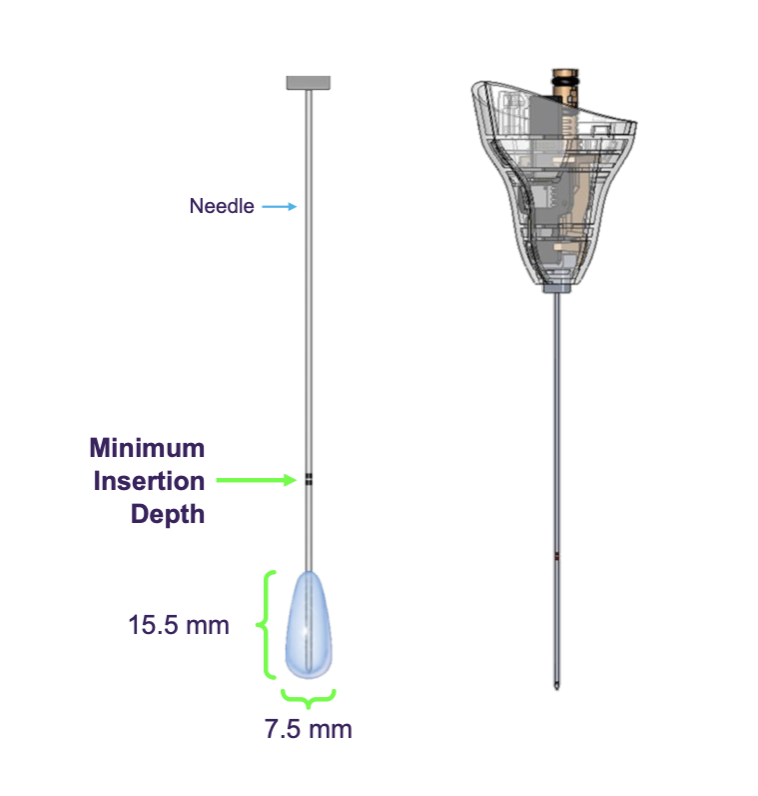
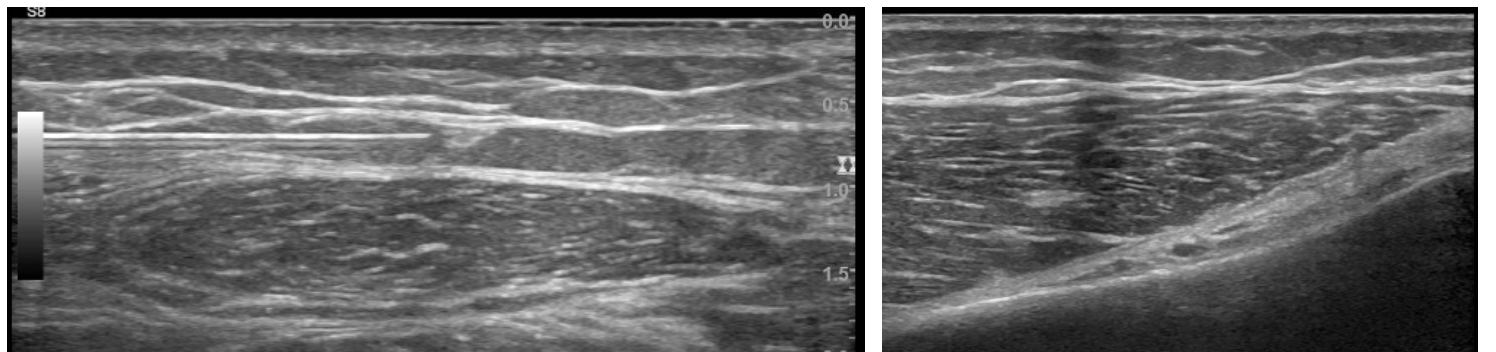
Iovera° is a handheld cryoneurolysis device, which delivers a controlled amount of liquid nitrous oxide to a closed end needle, which is then placed under ultrasound guidance adjacent to the specific targeted peripheral nerve. The liquid nitrous oxide flows from the hand piece to the distal end of the probe where it expands into a gas thus forming an ice ball at the targeted nerve achieving temperatures as low as -88°C. These temperatures cause a second-degree Sunderland nerve injury, which results in Wallerian degeneration. This leads to degeneration of the axon and myelin sheath, however, does not interfere with the integrity of the endoneurium, perineurium, and epineurium. The degeneration of the axon and myelin results in interruption of the nerve signals immediately after treatment, however, the nerve axon regenerates at a rate of approximately 1-2 mm per day, which provides a complete restoration of nerve function once regenerated (Evans, Lloyd, and Green 1981).
The patient was scheduled for cryoneurolysis of the bilateral knees, utilizing the iovera° device.
Bilateral cryoneurolysis with iovera° was performed under ultrasound guidance with the iovera° Smart Tip 190 needle, a 90mm needle which provides a single treatment ice ball approximately 15.5 x 7.5mm at the distal end of the treatment needle.

Treatment for the bilateral knees consisted of treating two branches of the anterior femoral cutaneous nerve at the mid-thigh level, treatment of the infra-patellar branch of the saphenous nerve, as well as treatment of the superior medial genicular nerve, superior lateral genicular nerve, and inferomedial genicular nerve with the device under
ultrasound guidance.

FOLLOW-UP AND OUTCOMES
Immediately following initial treatment, the patient reported complete resolution of his symptoms which lasted 4 1/2 months. The patient was able to return to activities without pain and the treatment was well tolerated. Based on the success of the first treatment, the patient then returned to clinic and scheduled his second treatment for his bilateral knees. The patient reported complete relief from the second treatment for just over 5 months. He again reported his return to activities. He then opted to proceed with a third treatment, which provided him with complete resolution of his symptoms for almost 6 months. The patient was able to continue in the Senior Olympics as he desired, competing in various track events with no pain following his first and third treatments. The patient did endorse mild dysesthesias about the anterior thigh following his third treatment, however, the patient was still very satisfied with the results of his treatment. This dysesthesia resolved completely, consistent with the duration and mechanism of action of the cryoneurolysis treatment and is a known potential site-specific reaction of the use of iovera°.
The patient in this case study experienced not only pain relief but also a substantial improvement in his quality of life. The resolution of his symptoms after the initial cryoneurolysis procedure allowed him to resume daily activities and engage in physical exercise that was previously limited by pain. Furthermore, the subsequent repeat treatments sustained the pain reduction, offering him an extended period of improved mobility and reduced discomfort.
DISCUSSION
In conclusion, this case study reports on a 65-year-old male with a history of Kellgren-Lawrence grade 2-3 tricompartmental bilateral knee osteoarthritis who underwent cryoneurolysis of the deep and superficial genicular nerves which demonstrated promising outcomes in the management of chronic knee pain. The patient reported complete resolution of his symptoms following the initial treatment, and two subsequent repeat treatments resulted in consistent and significant symptom improvement lasting between 4-6 months per treatment.
Cryoneurolysis, a procedure that involves freezing targeted nerves, has emerged as a viable option for patients suffering from chronic knee pain that is unresponsive to conservative treatments. By selectively targeting the deep and superficial genicular nerves, which are known to transmit pain signals from the knee, cryoneurolysis disrupts the nerve conduction, potentially providing long-lasting pain relief. Additionally, when compared radiofrequency ablation, cryoneurolysis potentially can have less side effects to include less local damage to surrounding tissues or risk of third-degree skin burn (McCormick et al. 2020).
These findings suggest that cryoneurolysis can be an effective treatment option for patients with knee osteoarthritis pain, providing a viable additional conservative treatment option for patients who wish to delay surgery or in non-surgical candidates. Its ability to offer long-lasting pain relief, coupled with the office-based nature of the procedure, makes cryoneurolysis an attractive option for individuals seeking to manage their chronic knee pain without significant downtime and limited side effects. The ability to repeat the procedure also makes it attractive option for non-surgical candidates.
While this case study highlights the positive outcomes achieved in a specific patient, further research and larger-scale studies are necessary to evaluate the generalizability and long-term efficacy of cryoneurolysis of the combined deep and superficial genicular nerves in the treatment of knee osteoarthritis. However, these initial results indicate that cryoneurolysis of the deep and superficial genicular nerves holds promise as a valuable and repeatable therapeutic addition to the armamentarium available for managing knee pain and improving the quality of life for patients suffering from osteoarthritis.
ACKNOWLEDGMENT
None
FINANCIAL SUPPORT AND SPONSORSHIP
None
INFORMED CONSENT
Written informed consent was obtained from the patient for publication of the case details
INSTITUTIONAL ETHICAL COMMITTEE APPROVAL
Not applicable
AUTHOR CONTRIBUTION
The author confirms sole responsibility for all aspects of this case study