


Introduction
In 1965, Branemark utilized the concept of a percutaneous OI implant linking bone through oral mucosa to an external prosthetic dental implant (Branemark 1983; Brånemark 2001). Since then several implant designs for use in orthopedics have come to market including the OI Protheses for the Rehabilitation of Amputees (OPRA) and ESKA produced the Endo-Exo Femur prothesis (EEFP).(Hagberg and Brånemark, n.d.; Aschoff, Clausen, and Hoffmeister 2009) For patients who have undergone a lower extremity amputation, the process of attachment and suspension of a prosthetic limb to the residual limb is critical for successful ambulation. Unfortunately, many factors including residual limb pain, neuromas, skin break down, ingrown hair follicles, residual limb perspiration, irregular scar tissue, and/or changes in body habitus/weight have been shown to be factors that can interfere with the functionality of conventional socket suspension systems (Lyon et al. 2000; Meulenbelt et al. 2009; Hagberg and Brånemark 2001; Demet et al. 2003; Pezzin et al. 2004; Pezzin, Dillingham, and MacKenzie 2000; Butler et al. 2014; Dudek et al. 2005; Ortiz-Catalan, Håkansson, and Brånemark 2014; Dillingham et al. 2001; Van de Meent, Hopman, and Frölke 2013). Patients with poor prothesis fit/suspension system eventually develop reduced hip range of motion with increased pelvic tilt leading to gait abnormalities (Tranberg, Zügner, and Kärrholm 2011). Any cause of pain associated with the suspension systems will naturally lead to reduced wear and functionality. These challenges eventually lead to the socket and/or prosthesis needing to be adjusted or replaced. Prosthesis adjustment costs are reported to range from $6,203 to $20,070 per episode (“Prosthetic FAQs for the New Amputee,” n.d.; Smith et al. 1995; Juhnke et al. 2015).
OI provides many benefits to patients including solutions to the complications that arise from traditional socket prosthesis. Studies have shown the principal benefits of a direct connection between the femur and the external prosthetic to be beneficial. OI allows the patient to experience more efficient energy transfer during movement when compared to a matched effort with a conventional socket prosthesis (Hagberg and Brånemark, n.d.; Van de Meent, Hopman, and Frölke 2013; “Comparison of Bone Anchored Prostheses and Socket Prostheses for Patients with a Lower Extremity Amputation a Systematic Review.Pdf,” n.d.). OI patients have reported a unique proprioceptive feedback when the coupled prosthesis makes contact with the ground, a phenomenon referred to as “osseoperception” (Hagberg and Brånemark, n.d.; Van de Meent, Hopman, and Frölke 2013; Häggström et al. 2013). The patient with a functional OI will no longer experience the suction socket related skin irritation issues. The reported advantages of a functioning OI implant include less pain, more efficient ambulation, and improved quality of life when compared to a traditional SS systems (Van de Meent, Hopman, and Frölke 2013; Tranberg, Zügner, and Kärrholm 2011; Häggström et al. 2013; Brånemark et al. 2014; Hagberg, Hansson, and Brånemark 2014; Hagberg et al. 2008; Lundberg, Hagberg, and Bullington 2011; Hagberg et al. 2005; Frossard et al. 2010).
Purpose
The authors of this study set out to explore the benefits of an OI system using a press fit bone stem interface. A custom OI stem has been designed and developed, the Patriot™, manufactured by Signature Orthopedics LTD, Sydney Australia. Initial designs of the custom Patriot™ stem included porous titanium coating on the surface of the stem at the area of diaphyseal engagement in concert with a custom stem diameter designed to match the native femoral canal (Figure 1). Later versions of the custom stem have incorporated hydroxyapatite surface treatment at the level of porous coating to further facilitate bone on-growth. The design philosophy of all variations of the custom stem was to create a 3-point fixation in the residual femur for stable and efficient energy transfer during ambulation. Allowing early stable fixation the device could then be coupled during the phase of bone on-growth, osseointegration. The surgical plan for implantation was based on reaming the femoral diaphysis to the diameter of the stem as was previously described.

In this case series the authors present the clinical outcomes from the application of a custom OI implant for the treatment of amputation at the transfemoral level. Outcomes are reported with utilizing the Q-TFA and SF-36 scores, time coupled per day, and overall satisfaction from the use of an (OI) implantable device in the treatment of 11 transfemoral amputees (TFA) with a minimum 6-month follow-up. Radiographs were reviewed for evidence of bone remodeling over the use of the Patriot™ OI system.
Materials and Methods
Implant design and fabrication
This study reports on a series of custom, nonFDA approved style of implanted device, collective termed “Patriot™” system. The Patriot™ OI stem is fabricated from forged titanium with a proprietorial surface porous coating. Later versions (3) incorporated a HA coating at the level of the porous section of the stem. Each device is fabricated for each patient as a custom device based on a pre-operative CT scan of the residual limb. The minimum length of the stem was designed to be 8 cm of diaphyseal contact. The pre-operative CT scan was rendered into a 3D image through analysis of the images. Each stem was then created to precisely match matched residual limb medullary canal morphology. A slotted tip is incorporated to allow for minor variations between the metallic stem and canal morphology during insertion. The concept is to allow deformation of the tip of the stem and prevent fracture during implantation. All stems shared common design core philosophy, but each was a custom device, applied under the FDA standards for custom implants.
Surgical and Rehabilitation Technique
Surgical and rehabilitation techniques have been described by Hillock et. al (Hillock et al. 2013; Hillock, MD, Tatum, BCP, and Dolegowski, PT 2014).
Enrollment and Consent
All subjects were counseled on the custom nature of the Patriot™ system and given written documentation outlining the planned follow up evaluations in accordance with all relevant legal and ethical standards. All actions and activity related to this research project have been conducted in compliance with an approved IRB protocol. This is a retrospective report of the Patriot™ system.
Patient Population
13 patients were treated with the Patriot™ OI device at two facilities treated by two surgeons. All patients had agreed to follow up evaluation of outcomes and current state. Of the 13 patients/femurs treated, there was one explant of a single stem per patient request. Another patient was lost to follow-up and presumed deceased due to a malignancy unrelated to the traumatic injury treated with the device. Another patient stopped responding to requests for engagement and was lost to follow up. The demographic information including age, sex, side of amputation, time from initial amputation to stage I OI, and reason for amputation of the remaining 11 were recorded and reported in Table 2. Of the 11 the duration of follow up data was 3 to 8 years, average of 5 years post treatment.
Outcome Evaluation: Patients were administered the Questionnaire for Transfemoral Amputees (Q-TFA) and Short Form 36 (SF-36) and were evaluated for overall pain, new back or stump pain, time coupled per day, and overall satisfaction. The responses were scored and compared to established data from previous studies reporting scores utilizing the same questionnaires from their peers.
Results
Patient Population and Demographics (Table 3)
Four female and seven male patients, age thirty-seven to seventy-three, treated with the Patriot™ OI device for TFA. The time since initial amputation to stage I surgery was two months to eighteen years. Reasons for amputation were limited to trauma (9), neoplasm (1), and infection (1). Time between stage I and stage II/device coupling ranged from three to seven months. The range for follow-up time was eight months to 87 months, average 63 months. (Figure 2)

Complications
Five patients developed minor PSP related complications including cellulitis, pain, and wound dehiscence requiring additional surgery and antibiotics. These procedures were all minor outpatient incision and drainage events with loosening of the PSP scar tissue. One patient sustained an implant failure at the designed shear pin. The system is designed to fail at the shear pin rather than damage an osseointegrated stem. Therefore, this was viewed as an acceptable failure as the system preformed as intended and the stem bone interface was protected. Revision of the broken abutment was completed under sedation with immediate return to full function as an outpatient.
Two patients expressed anxiety and developed a psychological body dysmorphic syndrome following implantation. Counseling and an intensive therapy program helped one patient overcome these issues. The patient is now very satisfied with the device, no longer taking any medications, nor seeking professional psychiatric treatment/support. Another subject was not able to obtain satisfaction and became clinically depressed. After careful consideration and counseling the second patient requested explant of a well-fixed stem.
Another patient had sustained polytrauma injuries at the time of their original amputations related to a helicopter crash. This was the only bi-lateral amputee in this series, right TFA and left transtibial (TTA) level. Due to the complex soft tissue injuries and burn scars conventional suction socket systems were too painful to be used for any period of time. The patient was wheelchair bound most of the time. The TFA Patriot™ custom stem was used on the right, while a separate custom TT level OI device was used on the left. The unique nature of bilateral OI stems at different levels has not resulted in delayed rehabilitation or complication.
Device Explant
As stated, a single OI device was explanted at the request of the patient. There was no mechanical or biological failure of the device. The patient was unable to tolerate anxiety related to the device and requested it be removed. This patient remains in contact with the treating surgeon.
Statistics methods
Descriptive statistics, including the 95% confidence interval, were calculated for the current study and for the comparator studies reporting scores from cohorts of transfemoral amputees not treated with OI. When 95% confidence intervals did not overlap, differences were inferred to be statistically significant.
Q-TFA
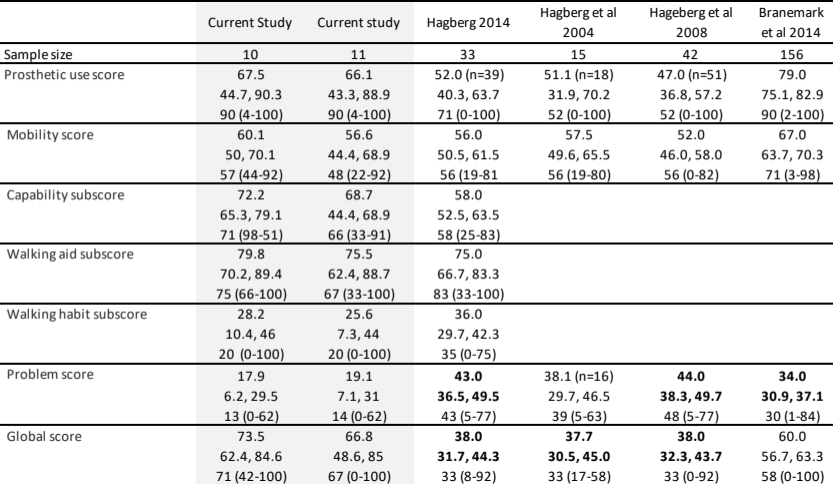
For the Q-TFA, confidence intervals were wide due to the limited sample size. Mobility score walking aid sub-score were similar to those reported in the other studies (Table 4). The study population had lower Problem scores and higher Global scores than most comparator studies reporting numbers from transfemoral amputees not treated with OI. These values were found to be statistically significant. Average Prosthetic use score and capability sub-score were trending upwards relative to other studies although the results were not found to be statistically significant. The walking habit sub-score was found to be lower in this study relative to previously reported numbers, but also not found to be statistically significant.
)_for_the_curren.png)
SF-36
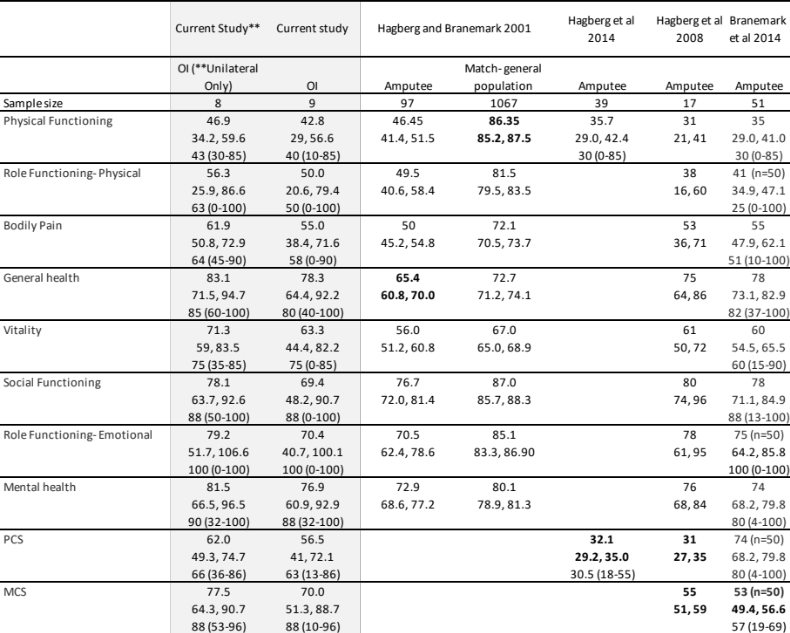
Based on the SF-36, the current study participants had quality of life scores similar to those of the general population and other amputee populations, with a few exceptions (Table 3). Although physical function was lower in all the amputee populations compared to the general population, vitality, social functioning, and role functioning on emotional tasks were not. The study population had higher general health and higher PCS and MCS than some other amputee populations not treated with an OI in the literature (Table 5).
)_for_the_curren.png)
Participants in the study reported average use of prosthetic limb of 12 hours/day. All patients reported equivalent or improved back pain since being treated with OI and only four patients reported an increased in residual limb pain.
Radiographic Image analysis
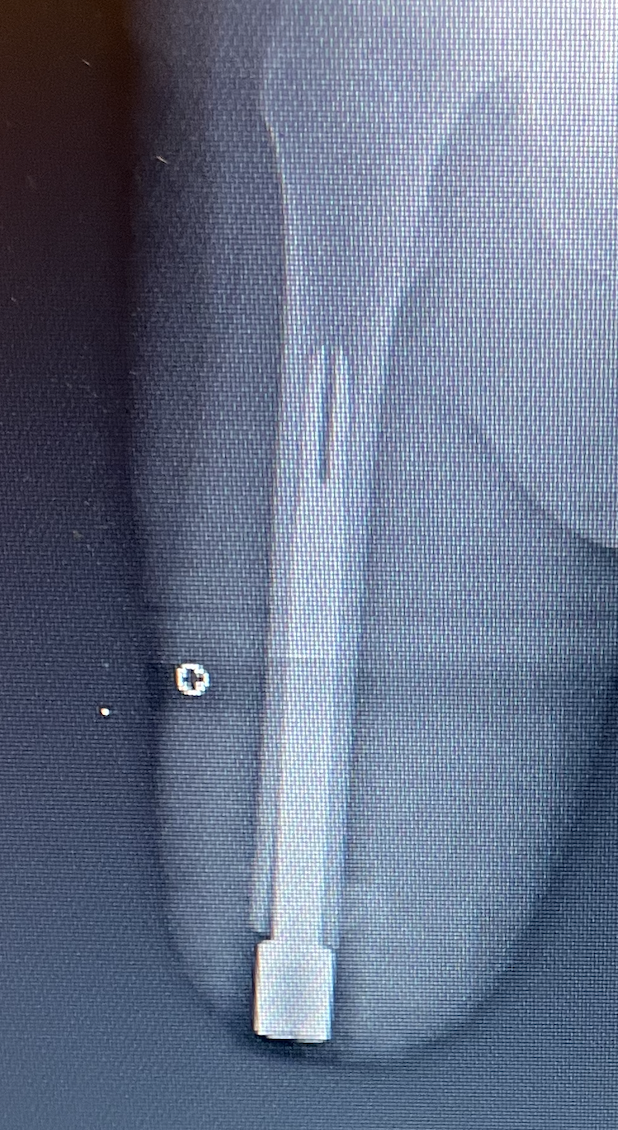
Of the 11 patients for which long term follow up data was available, 6 had serial plane film radiographic images available for review (Figures 3 and 4). Common features of these 6 femurs were robust bone remodeling in the diaphysis at the contact of the porous coated section. All showed minor distal bone reabsorption of 4 to 6 mm. The nature of this change is certain but did not appear to be associated with functional limitations or reported problems.


Discussion
This retrospective study is an unblinded case series sought to evaluate a custom OI device and its impact on recipient patients’ quality of life and function. Though the number of subjects was limited the findings were positive and support further study and development of OI systems.
Study group patients were evaluated for differences in quality of life based on the SF36 and Q-TFA, prosthetic use, residual limb pain, back pain, and overall satisfaction in transfemoral amputees relative to their peers. The results were consistent with previously published studies comparing patients treated with OI (Van de Meent, Hopman, and Frölke 2013; Lundberg, Hagberg, and Bullington 2011; Hagberg et al. 2005). Although not all findings were statistically significant, all metrics measured were found to be trending higher than those reported by peers not treated with OI. The improvements in scores are likely due to clear expectations, risks and benefits of the device, proper skin care, patient motivation, and previously failed use of a traditional socket suspended prosthesis.
A bone anchored prothesis has been reported in prior studies to lead to elimination of socket related problems including socket adjustments/re-fit modifications, less trouble sitting, residual limb perspiration, and ease of coupling and uncoupling, resulting in lower Q-TFA problem scores (Hagberg and Brånemark 2001; Hagberg, Hansson, and Brånemark 2014; Hagberg et al. 2008). Four of this study group patients reported residual limb pain post stage II coupling. All patients reported equivocal or improved back pain. All reported complete resolution of suction socket related skin irritation and pain. All showed dramatic increase in duration of coupling over time post stage II.
All subjects reported the experiencing the phenomenon termed osseoperception by prior authors. The proprioceptive sense vibration from prosthetic heel to ground contact was felt through the prosthesis, leading to more fluid and efficient gate cycle. All patients perceived better anatomic alignment of the coupled residual limb and felt improved gait mechanics. Patients reported that daily skin PSP hygiene protocol did not impact daily life.
These factors likely contributed to the statistically significant increase in Global Scores related to the issues and functionality of the prosthesis and quality of life for the amputee.
The remaining Q-TFA mean scores for prosthetic use and mobility had an upward trend, yet were not statistically significant, due to wide confidence intervals caused by small samples sizes and timing since Stage II Procedure. Patients with more therapy following stage II reported significantly higher mobility scores and prosthetic use of at least 12 hours/day than patients whose surgeries were completed within the last year. With more time and a larger sample, it is hoped that this trend will continue to improve.
As stated by Hagberg et al and by Geertzen et al., individuals with lower limb amputations need to be able to walk at least 500m on their own to be functionally independent (Hagberg, Hansson, and Brånemark 2014; Geertzen et al. 2005).Our study found that 18% (2/11) of patients walk 500m at least once a week, while none reported walking more than 500m daily, accounting for the low walking habit sub-score sub score. More research is needed to determine why these patients are not walking further. The majority did not report the need a walking aid while ambulating in the in their home 73% (8/11). Several subjects noted using at least one walking stick/cane for ambulation in the community. These findings align with TFA utilizing a SS prosthetic.
The Short Form 36 (SF-36) was used to evaluate health related quality of life (Ware and Sherbourne 1992). All scores from the questionnaire were included. The study population had statistically significant improvements in physical combined score (PCS) and mental combined score (MCS) relative to their peers. Although the individual components of each score were not statistically significant, all scores trended upwards and contributed to the increased combined scores for physical and mental functioning. The improvements seen in quality of life for those treated with OI are consistent with the findings of Branemark, Haegberg, and others (Hagberg and Brånemark 2001; Van de Meent, Hopman, and Frölke 2013; Tranberg, Zügner, and Kärrholm 2011; Brånemark et al. 2014; Hagberg, Hansson, and Brånemark 2014; Hagberg et al. 2008; Frossard et al. 2010). Although physical function of the amputee populations was lower compared to the general population, the vitality, social functioning, and role functioning for transfemoral amputees were equivalent to their nonamputee peers.
Low scores from patients not treated with OI correlate with the many challenges faced by this population. Although OI in general has not been shown to provide a perfect return to overall functionality, the increase in prosthetic use time, decreased residual limb-related problems, improved quality of life, and decreased problem scores can be regarded as a successful outcome supporting further study of OI systems.
Radiographic analysis demonstrated bone remodeling at the diaphysis consistent with Wolf’s Law response to loading. This is felt to show bone responding to load transferee through the device bone on growth. Distal bone reabsorption is attributed to stress shielding as has been reported in press fit total hip stems. An alternate explanation would be inflammation from chronic low-grade infection through the PSP leading to bone distal bone loss. Of note none of the stems failed to osseointegrate or later loosened, implying osteomyelitis was not a factor.
Study Limitations and Directions for Future Study
This was a retrospective case series of custom devices with a common design philosophy. The sample of subjects was small but meaningful and excluded patients with vascular disease. All retrospective series are associated limitations. Wide confidence intervals are attributed to the small patient population. This hindered statistically significant findings in all categories. The data was also self-reported via questionnaire. A physician assessment of capability and progress may be beneficial. Longer-term follow-ups will be required to fully evaluate the benefits and complications of the procedure and the Patriot™ system. These long-term follow-ups can also provide greater insight into assessment of quality of life and cost analysis of the procedure, device, and external prosthesis. Further study and long term data accumulation on patients with vascular disease treated with the device are also needed to better evaluate the efficacy of treatment with the device.
Conclusion
This case series studied outcomes with the custom Patriot™ OI system in the management of transfemoral amputees. The study demonstrated a decrease in problem scores and increased global scores on all metrics evaluated. It also showed improved quality of life in physical and mental functioning relative to their matched peers. Improvements in back pain were noted as well and overall status as an amputee and satisfaction with the device were stated to be average and above.
This study group clearly demonstrated equivalent success rates when compared to those previously published OI devices at the transfemoral level. Every measure reported was improved or neutral compared to matched peer amputees not treated with OI. Based on these favorable findings further study of the Patriot™ OI device is warranted. Though the current standard of care for the transfemoral level amputee is suction socket suspension OI devices offer many advantages that need further clarification. More long-term data is required to fully assess the efficacy of treatment of transfemoral and transtibial patients with OI, and more specifically the Patriot device. Also, future study should include patients with vascular disease to determine if this treatment may be a viable option for improving outcomes in patients with trans femoral and transtibial amputation in this patient population as well.