.jpg)
Introduction
Total knee arthroplasty (TKA) and total hip arthroplasty (THA) can be effective for severe osteoarthritis (OA), improving patient functioning and quality of life (Davis et al. 2011; Ethgen et al. 2004; Kane 2005; Mei et al. 2019; Okafor and Chen 2019; Skou et al. 2015). Currently, approximately 790,000 TKAs and 450,000 THAs are performed each year in the United States (American College of Rheumatology 2022). A projection model using data from the 2004-2014 National Inpatient Sample estimates that by 2040, TKA procedures may increase by 401%, or 3,416,000 procedures and THA procedures could increase by 284%, or 1,429,000 surgeries (Singh, Yu, et al. 2019).
However, postoperative pain is very common and can be significant in both TKA and THA (Grosu, Lavand’homme, and Thienpont 2014; García-López, Polanco-García, and Montes 2021; Andersen et al. 2009; Wylde et al. 2011; Liu et al. 2012); it is a predominant factor in extending hospital stays, negatively affecting functional outcomes and leading to readmissions (Husted et al. 2011; Singh, Lemay, et al. 2019; Lo et al. 2021; Dubljanin Raspopović et al. 2021). Opioids are commonly used for controlling postoperative pain (Fujii et al. 2018; Cook et al. 2019; R. Shah et al. 2020) but are associated with negative outcomes (Karssiens et al. 2021; Berardino et al. 2022; Blevins Peratikos et al. 2020) and may be a predictor of moderate to severe acute postoperative pain after TKA (García-López, Polanco-García, and Montes 2021). Additionally, the use of opioids for analgesia can lead to prolonged opioid use or dependency (A. Shah, Hayes, and Martin 2017; Politzer et al. 2018; Goesling et al. 2016). Guidelines from the American Association of Hip and Knee Surgeons (AAHKS), The American Academy of Orthopaedic Surgeons (AAOS), The Hip Society, The Knee Society, and The American Society of Regional Anesthesia and Pain Medicine (ASRA) state that “preoperative opioid use is associated with inferior patient reported outcomes, increased opioid consumption after surgery, an increased risk for chronic opioid use, and an increased risk of complications after total joint arthroplasty” (Hannon et al. 2020).
Multimodal analgesic (MMA) regimens are currently recommended for TKA and THA to control pain and can reduce opioid use; these typically include the administration of a combination of analgesics both pre- and postoperatively (Hannon et al. 2019; Li, Ma, and Xiao 2019; Moutzouros et al. 2020; Ma et al. 2021; Højer Karlsen et al. 2015; Karam, Schwenk, and Parvizi 2021; Blaney 2020). Periarticular injection administration, or local infiltration analgesia (LIA), during total joint arthroplasty has been shown to be effective in reducing pain and opioid use and is recommended for TKA and THA according to recent guidelines (Hannon et al. 2022). A global collaboration of surgeons and anesthesiologists, The PROSPECT Working Group, also recommends the use of periarticular LIA for TKA, but indicated that the heterogeneity of the analyzed studies precluded a specific recommendation for the optimal site and volume of the medications used in this manner (Lavand’homme et al. 2022). A common LIA used for total joint arthroplasty is ropivacaine, epinephrine, clonidine, ketorolac (RECK) although there is limited research evaluating the safety and efficacy of this “cocktail” (Duraney 2020; Tingle 2023). Thus, there is a need for effective non-opioid or opioid-sparing regimens to improve pain relief following TKA and THA, including extended-release local anesthetics.
Novel anesthetic indicated for postsurgical analgesia
HTX-011 (ZYNRELEF™, Heron Therapeutics, San Diego, CA) is an extended-release, dual-acting, local anesthetic consisting of bupivacaine and low-dose meloxicam within a tri(ethylene glycol) poly(orthoester) (TEG-POE) based technology Biochronomer™ polymer for drug delivery (Table 1); this novel polymer enables the controlled release of the active ingredients over a 72-hour period post-application (Ottoboni, Gelder, and O’Boyle 2014; Ottoboni et al. 2019, 2020). Hydrolysis causes cleavage of the polymer ester bonds, creating small water-soluble polymer fragments that are primarily eliminated via the kidneys (Ottoboni et al. 2019).
When formulated within a polymer, a low dose of meloxicam reduces the local inflammatory response and maintains a pH that is closer to physiologic levels in the surgical site environment; this allows bupivacaine to better penetrate the nerves and thus extend the analgesic effect beyond the typical duration of 12 hours or less (Ottoboni et al. 2019). Unlike periarticular injections, ZYNRELEF is a semi-viscous solution which is applied directly onto the pain-generating tissue within the surgical site. No needle or injection is necessary for application. The viscosity of ZYNRELEF results in the medication staying in the location where it is applied while allowing for extended release to all affected tissues (Ottoboni et al. 2019).
ZYNRELEF in TKA was evaluated in a Phase 2b, double-blind, placebo-controlled and active-controlled, multicenter trial of patients undergoing primary unilateral TKA under general anesthesia (Lachiewicz et al. 2020). The trial evaluated the analgesic efficacy, safety, and pharmacokinetics of ZYNRELEF as a single dose of ZYNRELEF (400 mg bupivacaine/12 mg meloxicam) (N=109; 13.7 ml) (Lachiewicz et al. 2020). ZYNRELEF was instilled after cementation of components, placement of the tibial spacer, and completion of irrigation and suction. ZYNRELEF was instilled onto the posterior capsule, the anteromedial tissues and periosteum, and the anterolateral tissues and periosteum using syringes with a Luer lock applicator. Patients receiving needle-free application of ZYNRELEF experienced superior pain reduction through 72 hours after TKA compared to patients receiving injected saline placebo and patients receiving injected bupivacaine hydrochloride. An open-label study of ZYNRELEF used in combination with an MMA regimen in patients undergoing TKA across six sites in the United States found reduced pain scores and opioid use compared to the prior Phase 2b randomized clinical trial. ZYNRELEF was well-tolerated, and no additional risk associated with the use of MMA was observed (Lee et al. 2022).
To better understand the outcomes of ZYNRELEF use outside of a clinical trial, we reviewed the medical records of patients undergoing TKA or THA at a single institution. The application technique described here addresses the need for additional research on ZYNRELEF in real-world settings in patients with TKA as well as experiences in THA, particularly in an outpatient setting, and used in combination with different MMA, periarticular injections, and adductor canal blocks.
Methods
Rationale and overview
In the winter of 2022, elective inpatient adult reconstruction was shut down in the Northeast United States because of the COVID-19 pandemic. The state in which I practice (Massachusetts) would only allow for outpatient adult reconstruction hip and knee patients; thus, our hospital (Southcoast Health Systems) examined the use of ZYNRELEF to determine whether a locally applied intra-incisional application of a substance would provide significant long-acting pain relief to allow for outpatient adult reconstruction surgery.
In the two years prior, Southcoast Health Systems had tried injections of RECK for patients undergoing TKA and THA. When we analyzed the pain response data, more than 80% of patients treated with RECK continued to have moderate to severe pain and 20% had severe pain as reported by the patient (on pain scale with mild pain being ≤3.5, moderate pain being 3.5-6.5 and severe pain being ≥6.5). This could be because none of the components within RECK are biologically active greater than 8 hours. Safety also became a concern with RECK after an internal database analysis found a 3% incidence of acute renal failure in patients treated with RECK. RECK has never been approved by the US Food and Drug Administration (FDA) and the concentration of ketorolac in the LIA cocktail is twice the recommended dose for patients over the age of 65, which is the age group that predominates in our practice. Therefore, we decided to switch from RECK to ZYNRELEF in February of 2022.
We conducted a retrospective review of patients undergoing TKA or THA between February and July 2022 in our practice to assess outcomes with use of ZYNRELEF as part of these procedures. Patients were treated with ZYNRELEF as part of our multimodal pain protocol. Our pre-operation procedures involve instructing patients to take 1000 mg of acetaminophen the night before surgery. We allow our patients to drink a carbohydrate drink up to two hours before surgery. On the morning of surgery, patients were given another 1000 mg of acetaminophen, 300 mg of gabapentin, and 15 mg of meloxicam. A summary of the medications received by all patients in this analysis before, during, and after joint replacement surgery is shown in Table 2. As this is a descriptive analysis, there was no control group; however, we did compare the number of narcotic pain prescriptions for procedures using ZYNRELEF and RECK.
Surgical technique and ZYNRELEF application
The surgical method and ZYNRELEF application were generally the same for both TKA and THA; the procedures were muscle-sparing but did not use minimally invasive surgical techniques or robotic assistance. Prior to incision, we injected 0.25% bupivacaine hydrochloride (Marcaine®, Pfizer, New York, NY, USA) to pick up dermal pain receptors with care taken not to exceed 400 mg of bupivacaine per day in systemic adsorption. This was not done for our first seven patients, who had a mean body mass index (BMI) of 35 and carried excess adipose tissue around the surgical site. However, we observed that these patients were not receiving adequate ZYNRELEF coverage at the incision site and hypothesized that the extra adipose tissue likely inhibited significant diffusion of the pain relief substance on to the actual dermal/skin portion of the incision. Therefore, we amended our protocol to include the pre-incision injection of 0.25% bupivacaine hydrochloride for the remaining patients.
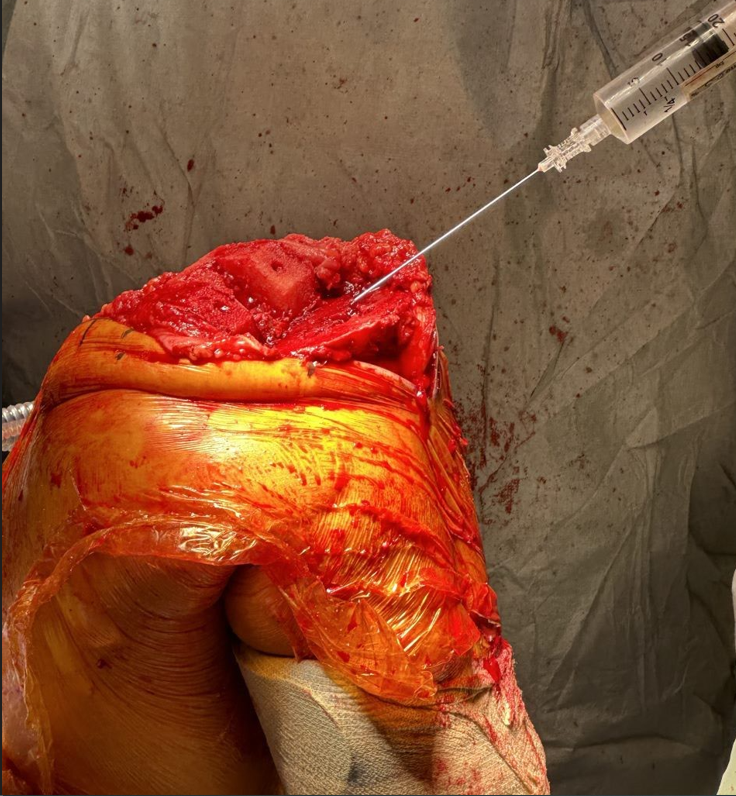
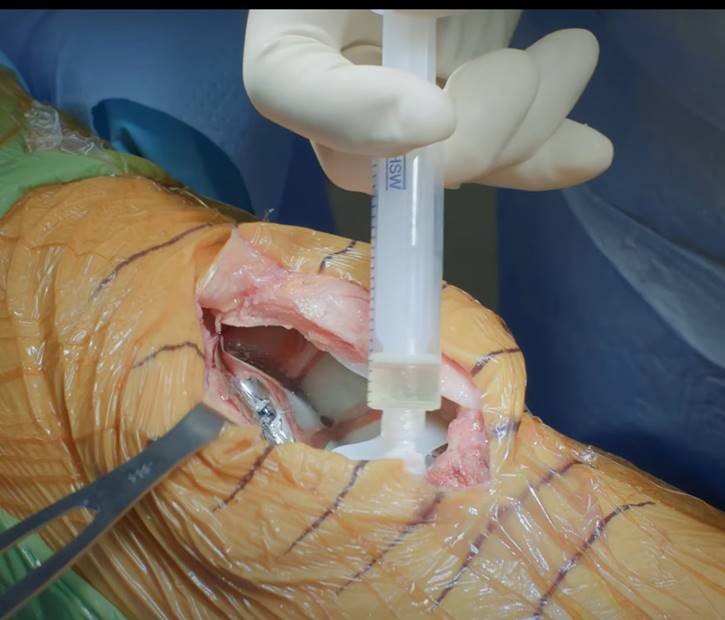
After incision, we layered 10cc of 0.25% bupivacaine hydrochloride on the raw edges of metaphyseal bone (Figure 1) once all of the bone had been prepared and prior to press fit or a cemented prosthesis. This is a carryover from research my team has conducted on pain fiber innervation of large joints and a great deal of pain and sympathetic wiring in the metaphyseal bone; we have routinely layered 10cc of 0.25% bupivacaine hydrochloride on the cut metaphyseal bone of any surgical site that we are attending. For TKA, the cut surfaces of the femur, tibia, and patella are cleared of fluid and fibrinous debris prior to layering bupivacaine hydrochloride, which is then allowed to be absorbed onto the bony trabecular surface. For THA, bupivacaine hydrochloride is layered onto the machined surface of the bone and allowed to soak in. For both TKA and THA, the wound edges are then injected with an additional 10cc of 0.25% bupivacaine hydrochloride to pick up dermal pain receptors. This seeps in and as it is absorbed it picks up and anesthetizes both the pain and sympathetic receptors in the bone. Once the implant was press fit or cemented in place, ZYNRELEF was applied over the entire surface area of the cut and exposed surfaces for both knee and hip replacements, inside the joint wound, bathing the synovial tissues (Figure 2). Because the patient is supine, ZYNRELEF is able to go through the articulation onto the posterior capsule. We did not use tourniquets, so meticulous hemostasis was carried out. We then performed a multilevel closure of fascia and dermis/skin. Finally, the dermal skin area was anesthetized with 0.25% bupivacaine hydrochloride. There were no difficulties or challenges regarding the overall surgical procedure or wound closure when using ZYRELEF.


Results
Overall, 167 joint replacement patients were treated with ZYNRELEF. The majority of patients were female, and the mean age was 65. Patient demographics are shown in Table 3. Outcomes for patients having TKA or THA are presented in Table 4. Pain, assessed within four hours after wound closure, was well-controlled, with most reporting mild pain (≤3.5 on an 11-point visual analog scale). Although no long-term observational pain scale assessments were available for these outpatient procedures, there were no call-backs from patients for additional pain medications (all patients were provided with 20 Percocet tablets to take home) and anecdotal reports from patients at the 10-day postoperative office visit were indicative of the pain being well-controlled. On average, patients experienced a 50% reduction in opioid use (milligram morphine equivalent [MME]), i.e., narcotic pain prescriptions went from 10 mg oxycodone when RECK was used to 5 mg, on average, when ZYNRELEF was used. Additionally, none of the 11 prior narcotic users who underwent treatment with ZYNRELEF within their incisions required augmentation of their home narcotic regimen.
No patients experienced a postsurgical infection, as assessed within 90 days of the surgery, nor were there any reported cases of local anesthetic systemic toxicity (LAST). No patients experienced acute renal injury, as assessed within 90 days post-op, and the rate of all-cause readmission was very low (3%). All patients were able to go home the same day as their procedure. All patients experienced excellent wound healing with no misdirection of fibroblasts. None of the patients who had ZYNRELEF technology used in their incisions required secondary manipulation for stiffness. We hypothesized that the COX-2 inhibition of the meloxicam exerted a suppressive effect on fibroblast proliferation.
Conclusions
My practice’s initiative to explore the use of ZYNRELEF was borne out of necessity during the COVID-19 pandemic, to allow more of our patients to have TKA and THA procedures when our hospital restricted elective surgeries to outpatient procedures only, which we were able to accomplish by using ZYNRELEF. Although TKA and THA procedures have traditionally required an inpatient hospital stay, these surgeries are more commonly being conducted as outpatient, or fast-track procedures (Kolisek et al. 2009; Hartog, Mathijssen, and Vehmeijer 2015; Goyal et al. 2017; Hoeffel et al. 2019). This was accelerated in other institutions as well due to the COVID-19 pandemic, which limited inpatient elective surgeries due to staffing and infection concerns (Cherry et al. 2021). Outcomes, complications, and readmissions for patients undergoing TKA or THA as outpatient procedures have been shown to be similar to those observed in inpatient procedures (Hartog, Mathijssen, and Vehmeijer 2015; Hoeffel et al. 2019; Cherry et al. 2021).
The use of ZYNRELEF in addition to an MMA regimen can also potentially reduce the need for postoperative pain medication, particularly opioids. Ensuring access to non-opioid medications is the key tenet of the Non-Opioids Prevent Addiction in the Nation (NO PAIN) Act (The Register Herald 2023). The legislation, signed into law in late 2022, “establishes separate payments for certain non-opioid treatments under the Medicare prospective payment system for hospital outpatient department services and the payment system for ambulatory surgical center services. The bill applies to pain management treatments that are able to replace or reduce opioid consumption, as shown through clinical trials or data” (117th United States Congress, 2022).
If more TKA and THA procedures can be conducted on an outpatient basis, there may be important financial implications as the number of these surgeries is expected to grow substantially in the near future (Singh, Yu, et al. 2019). As of April 1, 2022, Centers for Medicare & Medicaid Services (CMS) approved pass-through status for ZYNRELEF for separate reimbursement outside the Hospital Outpatient Department (HOPD) care setting; ZYNRELEF is currently the only local anesthetic with separate reimbursement in both the HOPD and Ambulatory Surgical Center settings (Heron Therapeutics Inc. 2022). Additionally, Heron Therapeutics, Inc. participates in the 340B Drug Pricing Program which provides financial assistance to hospitals serving vulnerable communities, to address the rising costs of prescription drugs (The American Hospital Association 2023). Thus, ZYNRELEF can be an economically viable option for hospitals in underserved communities providing TKA and THA procedures. Conversely, RECK is currently not reimbursed as part of the Diagnosis Related Group (DRG) code for total joint replacements. Additionally, RECK or its components may lead to renal injury (O’Donnell and Dolan 2018; Garg et al. 2014; Haragsim et al. 1994; Chan et al. 2014), which can be costly (Bekker 2019; Silver and Chertow 2017; Dasta and Kane-Gill 2019; Silver et al. 2017).
We have shown that when used as part of a multimodal pain protocol, ZYNRELEF is safe and effective in a real-world setting. Hydrolysis of the drug delivery polymer in ZYNRELEF causes the polymer ester bonds to separate, with the resulting water-soluble polymer fragments primarily eliminated via the kidneys (Ottoboni et al. 2019). Among the patients we analyzed in a six-month period undergoing TKA or THA with ZYNRELEF, there were no cases of acute renal injury. ZYNRELEF is also easy to use, owing to its semi-viscous nature and not requiring a needle or injection to be applied. Pain was well-tolerated and there were no incidences of postoperative infection.
There are limitations to our findings, including the retrospective nature of the review of patient records, lack of a control group with which to compare the experiences of TKA and THA procedures using ZYNRELEF, lack of long-term follow-up, limited patient-reported outcome measures, and lack of patient sociodemographic information. Additionally, this analysis describes the experiences of one surgeon at a single institution; thus, this may not be generalizable to the experiences of other physicians and facilities. Lastly, the patients who had TKA and THA during the period under review may have had different demographic and clinical characteristics than patients who were not selected for a procedure in an outpatient setting. Future research investigating ZYNRELEF as compared with RECK or other pain management options for TKA and THA is warranted to further assess the impact of each in real-world outpatient settings.
Acknowledgements
The author thanks Rebecca Hahn, MPH of KJT Group, Inc., Rochester, NY for providing medical writing support, which was funded by Heron Therapeutics, Inc., San Diego, CA in accordance with Good Publication Practice (GPP2022) guidelines. The author would also like to thank Lee Ann Girotti, MS, formerly of Heron Therapeutics, San Diego, CA for her review of the manuscript drafts.
Disclosures
Dr. Michael Langworthy is a consultant for Pacira, and receives royalties from Ortho Development.
Funding
Heron Therapeutics, Inc. provided support for this analysis and medical writing.