

Introduction
Over the years there has been an increasing demand for total knee arthroplasty (TKA) because of longer life expectancies, and rising expectations for quality of life and mobility in later life-years. Since the introduction of TKA into modern medicine, many types of pre-and intra-operative planning modalities for this surgery have been developed. Freehand techniques were swiftly augmented by intramedullary and extramedullary alignment guides which remain in use. However, these conventional alignment tools rely on direct visual inspection and assume a standard bone geometry, which does not apply to all patients. Multiple planning systems and software were developed to eliminate the need for these conventional alignment guides. The developers of these planning systems aimed to offer better alignment, survivorship of the prosthesis, and better clinical outcomes for patients receiving TKA, in an effort to reduce post-operative pain and loss of function. A rigorous amount of attention to pre- and intra-operative planning and their accompanying modalities are of importance to avoid implant failure as well as visualising the operation and foreseeing any potential pitfalls during surgery (Tanzer and Makhdom 2016).
The first surgical planning for arthroplasty was performed using tracing paper and/or plastic overlays on standard radiographs (Eggli, Pisan, and Müller 1998; Knight and Atwater 1992; Linclau, Dokter, and Peene 1993). Soon numerous computer-based pre-operative planning software programs were developed to ease this process, in combination with the use of calibrated radiographic images. During the past decades, multiple new modalities for planning of TKA have been introduced, including computer-assisted navigation (CAS navigation) for TKA, patient-specific instrumentation (PSI) (Stulberg, Picard, and Saragaglia 2000), and robot-assisted TKA (Bellemans, Vandenneucker, and Vanlauwe 2007).
With the introduction of new techniques and modalities, an abundance of research has been done to compare accuracy in alignment, cost-effectiveness and patient satisfaction rates between them. In general, successful TKA outcome is dependent on multiple factors such as surgical experience, patient demographics, pre-operative patient reported outcome measures (PROMs), pre-operative knee mobility, and patient expectations (Lizaur, Marco, and Cebrian 1997; Lingard et al. 2004). Differences in outcomes between specific types of planning modalities for TKA have been investigated (León-Muñoz et al. 2019). Yet, no full overview of computer-based pre- and intra-operative planning modalities and their method of use for TKA is available. With the current proliferation of available techniques, physicians are posed with the challenge of which type to implement into their daily practice and how to use them.
The aim of this systematic review was to give a comprehensive overview of historical and currently available digital pre- and intra-operative planning modalities for TKA. Furthermore, it aims to describe key elements of each surgical planning modalities and their method of use. In this review, based on articles found in the systematic review, the following types of CAS-based TKA were described: CAS navigation, PSI and robotics.
Materials and methods
Review and protocol
This systematic review was performed in line with the PRISMA-P statement for constructing a systematic review. The protocol for this systematic review has been registered in the PROSPERO database (protocol number CRD42023402165).
Search strategy and eligibility criteria
The following databases were searched: OVID Medline, EMBASE.com, Web of Science (Clarivate), and the Cochrane Library (Wiley).
No search limitations were applied. The first and final search was conducted on September the 3rd, 2022. Only titles in the English language were eligible for selection. The full search can be found in Appendix 1. All relevant titles in other languages are provided in Appendix 2.
Studies were included in the review if they met the following criteria:
-
Articles which described computer-based pre- and/or intra-operative planning modalities for TKA.
-
Articles which described patients undergoing TKA using computer-based pre- and/or intra-operative planning modalities, with explanation of the planning modality itself.
Articles were excluded if the authors solely investigated clinical outcomes. Furthermore, articles were excluded if they focused on non-digital planning modalities, singular tools for ligament balancing, reports on unicondylar knee arthroplasty or revision arthroplasty, case series, and case reports.
Study design and data collection
The studies found in the search were de-duplicated and the remaining studies were assessed based on the eligibility criteria. All articles found in the search were independently reviewed by two reviewers (DS, ID) using Rayyan, a tool for the screening and selection of studies for systematic reviews (Ouzzani et al. 2016). The first assessment was performed using the available titles and abstracts (TiAb). After this assessment, the reviewers examined the remaining full text articles and independently decided whether articles were eligible for inclusion. Any disagreement between reviewers was resolved by discussion between the reviewers and if requisite a third reviewer (MS) was involved. After final inclusion of the articles, the following data was extracted: Study ID (author, year), country of study conduction, and type of planning modality or modalities. Furthermore, textual data extraction was performed on development, use and explanation of use of computer-based pre- and intra-operative planning modalities for TKA.
Data analysis
This review is descriptive in nature; therefore no statistical analysis or meta-analysis has been performed.
Results
Search results
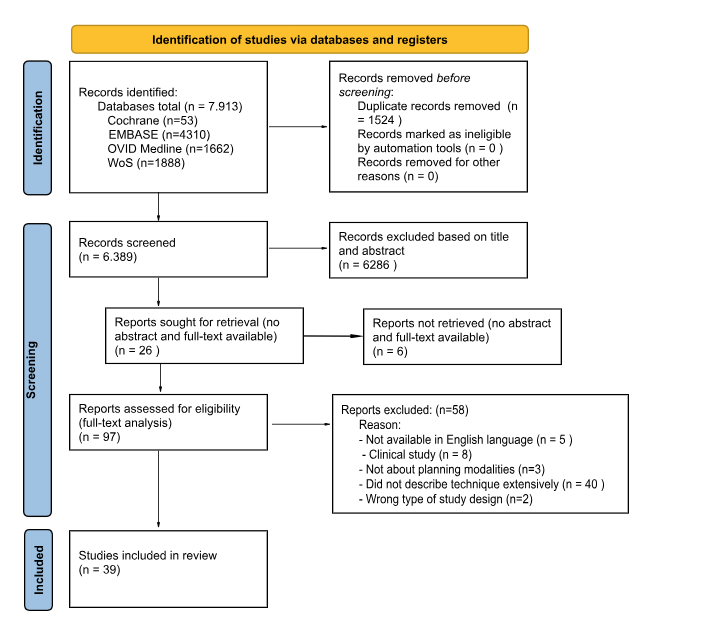
A full overview of the literature search and the selection process is provided in Figure 1. The systematic search in the abovementioned databases resulted in 7.913 hits. After deduplication 6.389 titles remained to be examined. These titles and abstracts were individually examined by the two reviewers (DS, ID) which resulted in 97 articles eligible for full-text analysis. After this analysis, 39 articles were included into the study (Table 1).

Study results
All of the 39 studies included into the systematic review are used for the following part of this article. First, a short history of CAS and its different subtypes will be introduced. Thereafter, an overview of these different CAS subtypes (CAS navigation, PSI and robotics for TKA) will be presented.
Computer assisted surgery (CAS)
CAS represents a surgical concept where computer technology is used for surgical planning. CAS was developed in the 1980s and early 1990s. In the following years, the use of CAS took off enormously, which also caused an increase in scientific interest. In 2000, the International Society for Computer Aided Surgery (ISCAS) was established. Ever since, CAS has brought a big change in tools and techniques on how surgeries are planned and executed in several medical disciplines.
CAS for TKA can be divided into three types; computer integrated instruments for surgical navigation, image guided instruments for surgical planning, and robotic devices (Delp et al. 1998; Desai et al. 2011; Joskowicz 2017).
The first type of CAS, computer integrated instruments, also known as CAS navigation, provides a real-time view of anatomy and marked surgical instruments intra-operatively. It uses 3D position sensors in order to visualise positional information of surgical instruments. The second type, image guided instruments, also patient-specific instrumentation (PSI), allows surgeons to create a three-dimensional (3D) pre-operative plan. 3D-modelled guides manufactured from these plans guide the surgeon intra-operatively. The third type, robotic assisted surgery, provides intra-operative assistance to surgeons using a (semi-)active robotic arm (Delp et al. 1998; Desai et al. 2011; Joskowicz 2017; Medical Advisory Secretariat 2004).
All three types of CAS will be presented in more detail in the next sections.
CAS navigation
The first type of CAS is CAS navigation.
General concepts
The first orthopaedic CAS navigation surgery was performed on a total hip replacement in 1992, by William Barger (Sacramento, California, USA). The first TKA using CAS navigation was executed in 1997 by Frederic Picard (Grenoble, France) (Delp et al. 1998; Desai et al. 2011; Cievet-Bonfils et al. 2020).
CAS navigation is used to achieve a digital image that serves as a map for the surgeon intra-operatively. These CAS-systems provide positional information about surgical instruments relative to the bone in this digital map, but do not perform any part of the surgery (Desai et al. 2011; Medical Advisory Secretariat 2004). With this digital map, surgeons are able to use additional information to make decisions on where to make bony cuts and how much bone is to be resected in TKA.
Three different types of CAS navigation exist: pre-operative imaging techniques, intra-operative imaging techniques, and image-free techniques.
The pre-operative imaging techniques, also volumetric image-based navigation, uses information from either a CT- or MRI-scan. The image information is transferred into planning software which surgeons can utilise for pre-operative decision making. For the second technique, intra-operative imaging, such as fluoroscopy, is used for anatomical mapping of the knee. This informative map is utilised during the surgery and aids the surgeon in planning their bony cuts. In the image-free technique, kinematic joint information and/or morphologic bone information is determined intra-operatively. Using software, the collected data is then merged with an anatomical model to form a digital image. Infrared light-based trackers are most commonly used, whereas research on electromagnetic tracking has also been done (Desai et al. 2011).
For all above mentioned techniques the obtained anatomical information has to be registered in order for it to be used. In other words, within either computer programs or during digital tracking itself, certain anatomical landmarks have to be registered in the computer, so that it registers the anatomy of the patient’s knee, or where the knee is within space (Desai et al. 2011).
After registration of landmarks has been completed, the programs can calculate bony resections and soft-tissue releases. Additionally, the surgeon is able to alter the computer-based planning to his or her wishes. When using CAS navigation, the computer-based programs assist the surgeon with planning, but ultimately planning is done by the surgeon (Desai et al. 2011).
After the initial planning has been performed, implementation during surgery follows. The image-free technique is the most used technique for computer assisted navigated TKA (Desai et al. 2011; Medical Advisory Secretariat 2004). Therefore, the authors will focus primarily on the infrared-, image-free based CAS navigation technique.
Surgical technique
Image-free CAS navigation systems consist of an infrared light-based optoelectronic tracker. This tracker guides the placement of the cutting guides by measuring the 3D coordinates of sensors. The optical localizer must be installed about one metre from the surgical field, to visualise placed trackers (Delp et al. 1998; Desai et al. 2011; Cievet-Bonfils et al. 2020; Mezger, Jendrewski, and Bartels 2013).
At the start of the surgery trackers with infrared light emitting or -reflecting diodes are placed in the femur and tibia to create reference frames. Different mechanical angles and the hip rotation centre are acquired by moving the hip, knee, and ankle in all directions. Next, bone morphing of anatomical landmarks such as the femoral condyles and tibial plateau is performed with a handpiece. The acquired points are combined to build up a 3D surface model of the patient’s individual anatomy. Bone cutting guides with sensors are then placed. The localizer measures the 3D coordinates of all sensors and visualises this on the screen. The angles of the bone cuts will be calculated by the computer system depending on the position of the guides. Once the orientation of the jig is in the desired position, the jig is secured in place. The surgeon can then make the bone cuts following the planning on the screen. Once the bone cuts are completed, the surgery continues as a traditional TKA (Delp et al. 1998; Desai et al. 2011; Cievet-Bonfils et al. 2020; Mezger, Jendrewski, and Bartels 2013).
Patient-specific instrumentation
Rapid prototyping (RP), also known as 3D printing, is a technology used to create templates of computer-generated designs. In the medical field, these 3D templates were first used by maxillo-facial surgeons and dentists (Ganapathi 2014). The first described case of RP being used for TKA was in the United States in 2007 (Chow and Torre 2016). RP technology can be applied to create PSI moulds to perform TKA.
General concept
For PSI, a CT-, MRI-, or a combination of an MRI-scan with a long leg x-ray is used to create a pre-operative plan constructed from patient specific imaging sets. When PSI was first developed, CT-imaging was applied to model the knee anatomy. Subsequently, software was used to create a personalised surgical plan for femoral and tibial resection planes. The personalised surgical plans were translated into 3D-modelled guides to fit the shape of each individual patient’s femur and tibia (Batailler, Swan, et al. 2021). However, as PSI developed, MRI-imaging became an available option, creating the potential to include the cartilage layer of the femur and tibia. Essentially, software programs transform 2D CT- or MRI-images into 3D rendered templates of the knee (Mattei et al. 2016).
The computer program is then used to place digital 3D-modelled femoral and tibial implants on the computer model of the patient’s knee (Delp et al. 1998; Müller et al. 2000; Radermacher et al. 1998). This technology led to the development of the PSI concept, in which 3D-printed plastic moulds can be created to aid the placement of cutting jigs on the patient’s knee during surgery. Instead of using the computer program itself to only plan component size and resection planes, the computer program is used to create corporeal objects to use intra-operatively (Gauci 2022). With this technology either pin guides could be manufactured, which aid surgeons to place pin tracks for conventional cutting guides, or the models can have integrated cutting slots (Ganapathi 2014).
Pre-operative planning and surgical technique
The preoperative scan is loaded into specific software systems. The surgeon can oversee the 3D modelled knee in the software system and evaluate the generated digital plan with bony resections. Several parameters, like the slope, rotation and bony resections can be assessed and altered within the system. The pre-operative plan can be modified to the surgeon’s wishes. Once an appropriate plan has been approved, the information within the software system is sent to a manufacturer and a mould is constructed (Mattei et al. 2016; Gauci 2022).
Intra-operatively, after the femoral and tibial bones are prepared for bony resection the PSI models are placed on the accommodating bone (McGovern 2011). Osteofytes and/or cartilage defects should not be removed before placing the model when MRI-imaging has been used as the models are based on bone as well as cartilage. Contrary, when using CT-based PSI the surgeon is required to remove the cartilage and soft tissue under cutting block contact points to ensure accurate fit of the mould (Mattei et al. 2016). The models are used for the initial femoral and tibial cuts. If sufficient, the surgeon can continue the next steps of the surgery. If cutting planes are unacceptable, intra-operative modifications can be made in terms of cut thickness, however rotation, slope and angulation cannot be changed. Once the desired bony resections are made, the usual TKA procedure follows.
Robotics for TKA
The third CAS system used for TKA is robotics.
The use of robotics in medicine started in the 1980s when industrial robots were modified for use in the operating theatre. The robots were used to bear tools for surgeons at specific locations in neurosurgical cases. When the tools arrived at their designated location the surgeon took over to perform the surgical duty. The robots were purely used as passive positioning systems (Davies et al. 2004, 2006).
Development of multiple robotic systems took place in the early to mid 1990s, mostly in neurosurgery, maxillofacial surgery, laparoscopic surgery, and orthopaedic surgery. This resulted in the first clinical trials for a robotic TKA in 1998 (Davies et al. 2006).
General concepts
In orthopaedic surgery, three types of robotic systems are in use: passive, active and semi-active or synergistic robots (Jacofsky and Allen 2016; Sousa et al. 2020). The above-mentioned system is an example of a passive robot. The robot itself does not perform any surgical action but aids the surgeon in either: surgical simulation, pre-operative planning or intra-operative navigation. An example of a passive robot in knee surgery is the BRIGITTM robot, which eventually developed into the semi-active ROSA® robot (Jacofsky and Allen 2016; Sousa et al. 2020; St Mart and Goh 2021; X. Chen et al. 2022).
The second type of robots are active robots. In TKA, active robots were the first generation of joint surgery robots used (X. Chen et al. 2022). These robots carry out a specific task such as making bony cuts or reaming femoral cavities in hip surgery. The surgeon does not intervene in their surgical duties, but the systems contain a safety override allowing the surgeon to take over if needed. Some examples of these types of robots in knee surgery are ROBODOC® (now TsolutionOne®), and the CASPAR® robot (Medical Advisory Secretariat 2004; Jacofsky and Allen 2016; Sousa et al. 2020; St Mart and Goh 2021; X. Chen et al. 2022; Clatworthy 2022; Chan et al. 2020; Nathwani and Shenoy 2021; A. F. Chen et al. 2018; Siebert et al. 2002). The third type of robots used in orthopaedic surgery are synergistic or semi-active systems. These robots work together with the surgeon and combine their skills to perform specific surgical steps. Examples used for TKA are the Acrobot®, MAKO®, VELYS™ Robotic Assisted Solution (VRAS), and NavioTM. The synergistic system allows the surgeon to control the surgical strategy of the robot while the surgeon directly receives feedback when for instance making bony cuts in TKA (Medical Advisory Secretariat 2004; Davies et al. 2004, 2006; Jacofsky and Allen 2016; Sousa et al. 2020; St Mart and Goh 2021; X. Chen et al. 2022; Nathwani and Shenoy 2021; Jakopec et al. 2001, n.d.; Jakopec, Rodriguez, et al. 2003; Jakopec, Harris, et al. 2003).
Among these three types, the semi-active systems are the most widely used robotic systems for TKA.
In addition to the above-mentioned different types of robotic systems, there are several possibilities for orientation and visualisation. Image-based systems rely on CT, MRI or X-rays to construct a virtual model of the knee based on CAS technology. A key advantage of these systems is the ability to perform pre-operative planning. Imageless systems record bony landmarks intra-operatively to form a virtual reconstruction of the knee from a preloaded database of patient scans in the robotic software. Some robotic systems use a combination of both (Jacofsky and Allen 2016; Sousa et al. 2020; St Mart and Goh 2021; Nathwani and Shenoy 2021; Siebert et al. 2002; Jakopec et al. 2001, n.d.; Jakopec, Rodriguez, et al. 2003; Jakopec, Harris, et al. 2003; Konan, Maden, and Robbins 2017; Graichen, Lekkreusuwan, and Scior 2019; Roche 2015; Wu et al. 2021).
Two different software systems exist. Closed systems only use specific manufacturer approved implants, while open systems allow different implants designs from different manufacturers from an inventory. With open systems, general bony cuts can be planned, but techniques specific to a specific knee implant cannot be applied (Jacofsky and Allen 2016; Sousa et al. 2020; St Mart and Goh 2021; Nathwani and Shenoy 2021; Roche 2015; Liow et al. 2017).
Planning and surgical technique
Active robotic systems
Active robot systems use a pre-operative planning module where the surgeon determines position of implants on a pre-operative CT scan (most used) or MRI (Joskowicz 2017; Nathwani and Shenoy 2021; Siebert et al. 2002). Based on this pre-operative plan, a specific machining plan is generated by the software. Fixed trackers are attached to the femur, tibia, and the surgical cutting tool. After additional pin-based contact registration, the plan is then used by the robotic system during surgery. The limb is immobilised and attached to the robot. In active systems, the robot mills or saws the bone, or places the jigs on the bone for manual cutting. Thus, active robotic systems are autonomous and operate under supervision of the surgeon. The surgeon does not provide any active input during these surgical steps, but the surgeon can alter or stop the robot at any time (Joskowicz 2017; Nathwani and Shenoy 2021; Siebert et al. 2002; Konan, Maden, and Robbins 2017).
Passive robotic systems
Passive robots utilise three types of methods for intra-operative navigation: volumetric image-based navigation in which CT, MRI or ultrasound images are used, fluoroscopic navigation which construct guiding maps intra-operatively, or imageless navigation (Medical Advisory Secretariat 2004).
The main concept is that the robotic system is used as a positioner for a guide or a jig (Sousa et al. 2020; St Mart and Goh 2021; Nathwani and Shenoy 2021; Batailler, Hannouche, et al. 2021; Malvisi et al., n.d.). Image-based surgery is performed by importing pre-operative images into the system. Subsequently, validated algorithms create a virtual 3D model of the patient’s knee. Imageless surgery is performed by stylus guided orientation of the leg and knee during surgery. When using the imageless method, the surgeon points out anatomic landmarks and performs mobilisation of the knee, which is of importance to gather information on the characteristics of the soft tissue balance of the knee. Using a camera and calibrated tracking pins inserted into the femur and tibia, the system creates a 3D rendered reference of the knee and where it is located within the OR (St Mart and Goh 2021; Nathwani and Shenoy 2021; Batailler, Hannouche, et al. 2021; Malvisi et al., n.d.). Whichever method is used, during surgery the robotic system uses the acquired information to place a cutting jig in the required position for the surgeon to make an accurate cut (St Mart and Goh 2021; Nathwani and Shenoy 2021; Batailler, Hannouche, et al. 2021; Malvisi et al., n.d.).
Semi-active robotic systems
In the late 2000s, semi-active robots were developed for unicompartmental knee arthroplasty (UKA), and later for TKA as well (Joskowicz 2017; Cievet-Bonfils et al. 2020; Nathwani and Shenoy 2021; Konan, Maden, and Robbins 2017; Bautista, Manrique, and Hozack 2019). Semi-active systems are under direct control of the surgeon. The surgeon performs the burring- or cutting procedure, but the robotic system will retract the cutting tool or provide alerts and feedback when the limits of a predefined operative region are reached (Medical Advisory Secretariat 2004; Nathwani and Shenoy 2021; Jakopec et al. 2001, n.d.; Jakopec, Rodriguez, et al. 2003; Jakopec, Harris, et al. 2003; Konan, Maden, and Robbins 2017). Semi-active systems are able to do this by using image-based or imageless software and adapt based on the anatomy of the individual patient (Calliess et al. 2018).
To create a virtual model of the knee intra-operatively, the surgeon places pin-tracking diodes in the femur and tibia, and registers anatomical landmarks with a navigation probe. The system uses an infra-red camera that tracks the attached diodes and the robotic arm. By moving the limb and knee, construction of the limb axis and calculation of gap balance are carried out. Within the computer system a template implant is placed in the desired position on the virtual model of the knee. Then, a high-speed burr or saw attached to the robotic arm performs bone resections. The system provides resistance and automatically stops when bony cuts go outside of the determined boundaries defined by the operative plan. The components are implanted by the surgeon (Cievet-Bonfils et al. 2020; Jacofsky and Allen 2016; Sousa et al. 2020; St Mart and Goh 2021; Nathwani and Shenoy 2021; A. F. Chen et al. 2018; Jakopec et al. 2001, n.d.; Jakopec, Rodriguez, et al. 2003; Jakopec, Harris, et al. 2003; Wu et al. 2021; Bautista, Manrique, and Hozack 2019; Calliess et al. 2018; Roche 2021; Yohe et al. 2021).
Discussion
Due to the abundance of planning modalities for TKA, physicians are posed with the challenge of which type to implement into their daily practice. In this comprehensive review, the authors aimed to summarise the development and key elements of computer-based pre- and intra-operative planning modalities for TKA. In this review the authors described CAS, PSI and robotics for TKA.
CAS is an evolving field with continuously changing techniques and software. For TKA, technological developments such as computer software and execution tools are continuously invented to achieve more accurate alignment, better interaction with and understanding of soft-tissue balance, and subsequently improved prosthesis survival and patient satisfaction. The question of what kind of technological improvement will be most impactful remains. The future of CAS for TKA is promising however, especially since the rise of artificial intelligence (AI) which may be able to assist with planning and alignment. The possible role of AI is however not yet known.
In addition to these technological developments, different alignment strategies arose which in combination with CAS could improve clinical outcome, patient satisfaction, prosthetic alignment and implant survival. Theories regarding native knee alignment and knee phenotyping are currently being researched extensively.
Alignment has been designated as one of the factors that determine survivorship of the implant (Werner et al. 2005). Since the introduction of TKA, the fixed alignment approach of mechanical alignment (MA) has been used as consistent targets for all knees (MacDessi et al. 2023; Allen and Pagnano 2016; Oussedik et al. 2020; Karasavvidis et al. 2023). MA has been, and still remains, the most common alignment technique for executing TKA which attempts a horizontal joint line, and a neutral mechanical axis (MacDessi et al. 2023; Allen and Pagnano 2016; Oussedik et al. 2020; Insall et al. 1985). This results in an evenly distributed biomechanical loading on the femoral and tibial implants (Insall et al. 1985). However, MA alters natural knee kinematics and balance, which may compromise functional outcomes.
To simulate the patient’s own pre-arthritic, or constitutional, alignment, multiple alignment philosophies arose as alternatives to MA and are gaining popularity (Karasavvidis et al. 2023). Kinematic alignment (KA) has been suggested as a technique to recreate a patient’s constitutional alignment, improving soft tissue balance and resulting in more natural knee movements with similar or better PROMs (Allen and Pagnano 2016; Karasavvidis et al. 2023; Lee et al. 2017; Tian et al. 2022; Gao et al. 2020; Howell et al. 2013). MA restores the 3D morphology of the native knee irrespective of anatomical extremes, therefore prioritising the patient’s constitutional alignment over the generic target of a neutral axis. Nevertheless, KA may increase the risk of alignment-related early failures.
With the proliferation of CAS technology, resection thickness, alignment and joint gaps can be planned and/or assessed intra-operatively. As a result, functional alignment (FA) has been proposed as a technique to combine optimal mechanical alignment and balancing of the soft tissues. With the aid of CAS, the limb alignment and gaps can be planned or assessed in real-time by changing the implant position in all three planes, individualised to the patient’s knee and gaps. Consequently, individualised alignment targets can be achieved reproducibly (Oussedik et al. 2020; Karasavvidis et al. 2023). This comprehensive systematic review aids in the understanding of the differences between computer-based planning modalities from which surgeons can choose to achieve the chosen alignment strategy.
In addition to the knowledge of alignment strategies themselves, understanding of constitutional knee alignment and different phenotypes is of utmost importance to choose an optimal alignment strategy in TKA. In patients with knee arthritis, asymmetric loss of the tibiofemoral joint space results in an altered mechanical hip-knee-ankle (HKA) angle compared to their pre-arthritic coronal knee alignment. Over the last years, research was conducted on estimation of the constitutional alignment before arthritic deformity occurred. Some authors proposed a formula to calculate the ‘arithmetic HKA’ (aHKA), from which the approximate constitutional alignment could be derived (Griffiths-Jones et al. 2021; MacDessi et al. 2020). Apart from aHKA, joint line obliquity (JLO) has been designated as an independent variable in knee alignment. This JLO in the coronal plane is parallel to the floor during walking or running as the centre of mass shifts laterally during single leg stance, with adduction of the hip joint (MacDessi et al. 2023; Oussedik et al. 2020).
Recent literature highlighted the fact that the anatomy of the knee is variable, and consists of multiple phenotypes (Hirschmann et al. 2019). Based on the aHKA and JLO, the Coronal Plane Alignment of the Knee (CPAK) classification has been developed. This classification categorises knees in nine different phenotypes (MacDessi et al. 2021). Knowledge of these functional knee phenotypes may enable the surgeon to identify which patients may benefit most from different alignment strategies where soft-tissue balance is prioritised (MacDessi et al. 2021).
With the acquired knowledge on alignment strategies, constitutional knee alignment, and different phenotypes, surgeons are guided to a better understanding of optimal positioning of a total knee prosthesis for specific groups of patients. This can be valuable toward personalised TKA. To achieve this in daily practice, future developments within CAS could be accommodating to accomplish personalised alignment goals as desired by the surgeon.
New technological developments occur constantly. Recently, Augmented Reality (AR) has been proposed as a technology that could improve accuracy in TKA, providing a more efficient and cost-effective solution. Fucentese et al. proposed that the use of AR glasses during surgery improves procedure efficiency, particularly when combined with single use instruments. Furthermore, it allows for better visualisation of the ligaments of the knee joint and tibial rotation during TKA implantation (Fucentese and Koch 2021). However, AR is currently in the early stages of research.
The strength of the present article is that it was performed in line with the PRISMA statement for performing a systematic review. The search was conducted by a clinical epidemiologist to ensure that relevant articles could be included.
Its flaw however, is the exclusion of non-English language and non-full text documents which could lead to reporting bias. Also, a fair amount of available literature is from the first or older computer-assisted technologies, while these change over time. Therefore, one cannot generalise the results of a certain CAS system to other systems as some techniques are outdated swiftly by continuous evolutions within and in between groups of techniques (Medical Advisory Secretariat 2004). In addition to this, while the search was conducted systematically, one could not assume that certain valuable articles might have not been found within the margins of the search. Furthermore, this review described key elements of each surgical planning modality, and their method of use, objectively while experiences of use may differ in clinical practice.
As new techniques are researched and may become popularised it is of importance that clinical performance of planning modalities remain the top priority. At present, no clear answer can be given on which modality is superior. More research remains to be done to define better understanding of optimal positioning of a total knee prosthesis, and possibly develop the best possible planning modality for TKA.
Conclusion
Over the past decades, technological advances using computer software such as CAS navigation, PSI, or robotics were developed to achieve improved clinical outcomes after TKA. With an abundance of available techniques, the author’s goal was to create a clear overview for readers to understand the differences between available computer-based planning modalities. This review showed that the monumental development of digital planning modalities for TKA has led to a vast amount of well-researched options that surgeons can choose from and use in daily practice.