
INTRODUCTION
Distal humerus fractures encompass about 2% of all adult fractures (Athwal, Raniga, et al. 2019) and about half of fractures surrounding the elbow (Anglen 2005) with a reported overall incidence of 5.7 cases/100,000 adults (Robinson et al. 2003). Additionally, operative management of these injuries continues to pose significant challenges to surgeons due to the complex anatomy, poor bone stock, small fracture fragments, and multiplanar kinematics of the elbow joint (Ring and Jupiter 1999; McKee et al. 2009; Mighell et al. 2015). Despite advancements in surgical technique and implant design, there persist a sequela of post-operative complications associated with this fracture including nonunion, arthrofibrosis, and neuropathy (Ring and Jupiter 1999; McKee et al. 2009). One such complication that has gained significant attention is delayed ulnar neuritis following open reduction with internal fixation (ORIF).
Intra-operative management of the ulnar nerve can vary depending on surgeon preference and patient presentation, with no clear guideline for management, leaving the decision to be made by the surgeon at the time of the procedure (Worden and Ilyas 2012). The most common interventions are an in situ neurolysis or anterior subcutaneous transposition. In situ neurolysis involves direct release of the nerve in its anatomic position; while anterior subcutaneous transposition involves moving the nerve into the anterior subcutaneous tissues in an effort to protect it. Although the theoretical benefits of in situ neurolysis or anterior subcutaneous transposition may seem intuitive, recent evidence suggests that excessive manipulation of the nerve puts it at risk for injury. However, these reports are primarily limited to retrospective reviews of small case series.
This study utilizes a large, commercially available, insurance database to determine the impact of intra-operative ulnar nerve management during distal humerus ORIF on post-operative ulnar nerve neuritis.
METHODS
Data Source
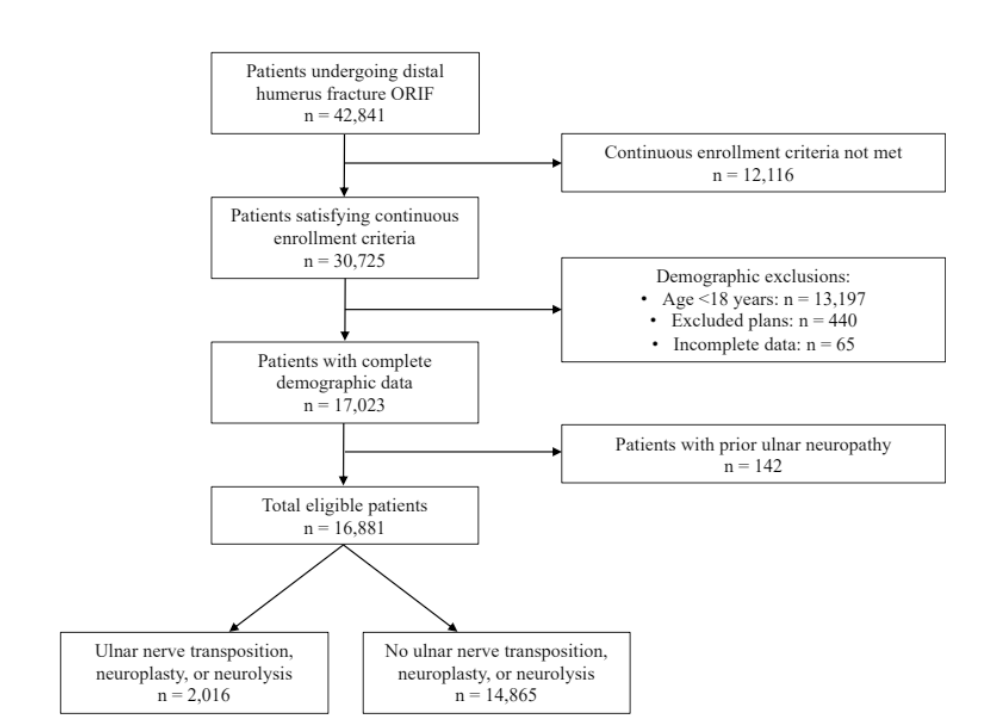
Data from the PearlDiver Mariner Patient Claims Database (PearlDiver Technologies, Colorado Springs, CO, USA), consisting of administrative records from over 151 million insured individuals from 2010 through 2020, were analyzed. Patients from all United States regions and diverse insurance plans are represented, including Medicare Advantage, Medicaid managed care, and private insurance. The data includes patient demographics, diagnoses, procedures, and dates. All adult patients undergoing open reduction internal fixation (ORIF) of distal humerus fractures, including epicondylar fractures, using their respective Current Procedure Terminology (CPT) codes (CPT-24545, CPT-24546, CPT-24586, CPT-24575, CPT-24579) were identified. Concurrent ulnar nerve transposition, neuroplasty, or neurolysis was defined using CPT-64718, occurring on the same day as the index procedure. If patients received bilateral distal humerus ORIF, only the first instance was included. Patients were included if they were actively enrolled in the database one year prior to and after the index ORIF for accurate tracking of comorbidities and outcomes. Additional inclusion criteria included having complete demographic data. Patients with pre-existing ulnar neuropathy, defined as the presence of a diagnostic code for ulnar neuropathy (ICD-9 354.2, ICD-10 G56.20-G56.23) within one year prior to distal humerus ORIF were excluded. Patients were divided into those who received ulnar nerve transposition, neuroplasty, or neurolysis (CPT 64718) and those who did not. A flow diagram of cohort creation is shown in Figure 1.

Outcomes
The primary outcome was the incidence of delayed ulnar neuropathy. This was distinguished from post-injury or post-operative ulnar neuropathy, which occurs within 2 weeks after surgery as defined by Shin and Ring (Shin and Ring 2007). The cumulative incidence of ulnar neuropathy occurring at 1-month intervals after distal humerus ORIF was measured. Ulnar neuropathy incidence at 3, 6, 9, and 12 months after surgery was compared between cohorts.
Statistical Analysis
Continuous variables were reported as mean (SD) and compared using t-tests. Categorical variables were reported as frequencies and evaluated using chi-square tests. Elixhauser comorbidity scores were reported as mean (SD) and compared using Mann-Whitney tests. Multivariable logistic regression models were employed to evaluate the association between ulnar nerve transposition, neuroplasty, or neurolysis and the development of delayed ulnar neuropathy, adjusting for the effects of age, sex, insurance type, and Elixhauser comorbidity index. A separate multivariable linear regression model was constructed to evaluate the influence of ulnar nerve transposition, neuroplasty, or neurolysis on the timing of delayed ulnar neuropathy, adjusting for the same covariates as above.
Based on a prior study that showed an ulnar neuropathy incidence of 33% in patients who received ulnar nerve transposition compared to 9% in patients who did not (Chen et al. 2010), at least 50 patients in each cohort would provide 80% power to detect a difference of at least this magnitude (alpha = 0.05). Statistical significance was defined as p<0.05.
RESULTS
Incidence of Ulnar Neuropathy
We identified 16,881 patients undergoing distal humerus ORIF, of which 2,016 (11.9%) received concurrent ulnar nerve transposition, neuroplasty, or neurolysis. Overall, 95 patients (0.6%) developed ulnar neuropathy within 14 days after surgery, defined as post-injury or post-operative ulnar neuropathy. The majority of these cases occurred in the ulnar transposition, neuroplasty, or neurolysis cohort compared to patients who did not receive ulnar transposition, neuroplasty, or neurolysis (adjusted odds ratio [OR] = 11.22 [95% confidence interval (CI): 7.45, 17.09]; p<0.001). The cohorts differed by age and insurance type distribution (Table 1).
The overall rate of delayed ulnar neuropathy between 2 weeks and 1 year after surgery was 933 / 16,881 (5.5%), which occurred in 191 / 2,016 (9.5%) patients who received ulnar nerve transposition, neuroplasty, or neurolysis and 742 / 14,865 (5.0%) patients who did not (Table 2). In the multivariable analysis, ulnar nerve transposition, neuroplasty, or neurolysis was associated with a 197%, 124%, 101%, and 105% increased odds of delayed ulnar neuropathy at 3, 6, 9, and 12 months after surgery, respectively (p<0.001; Table 3).
Timing of Ulnar Neuropathy
In patients who developed delayed ulnar neuropathy, the average time between ORIF and ulnar neuropathy diagnosis was 149 (86) days. In the cohort that received ulnar nerve transposition, neuroplasty, or neurolysis, the average time to diagnosis after surgery was 132 (88) days compared to 153 (85) days in patients who did not receive ulnar nerve transposition, neuroplasty, or neurolysis (p = 0.004). In the multivariable analysis of patients who developed delayed ulnar neuropathy, receiving ulnar nerve transposition, neuroplasty, or neurolysis was associated with an earlier post-operative diagnosis of ulnar neuropathy by 21 days (95% CI: 7-34 days; p=0.003).

DISCUSSION
In this large database study, ulnar transposition, neuroplasty, or neurolysis at time of distal humerus ORIF leads to increased incidence of ulnar neuropathy in both the immediate post-operative and delayed phase. The greatest odds ratio of developing ulnar neuropathy was present in the immediate post-operative cohort (OR 11.22, 95% CI). Additionally, for patients who received ulnar nerve transposition, neuroplasty, or neurolysis, delayed ulnar neuropathy diagnosis was more prevalent at all time points evaluated, 3, 6, 9, and 12-months (OR 2.97, 2.24, 2.01, 2.05 respectively, P<0.001) post-operatively when compared to patients who did not have ulnar nerve transposition, neuroplasty, or neurolysis.
Ulnar nerve dysfunction is a well described finding associated with distal humerus fractures, having a reported prevalence of 0-51% resulting in transient paresthesia, numbness, and, in severe cases, loss of motor function (Shearin et al. 2018; Holdsworth and Mossad 1990; Vazquez et al. 2010; Svernlöv, Nestorson, and Adolfsson 2016). Due to the anatomic tethering of the ulnar nerve posterior to the medial epicondyle, the nerve is prone to injury at various points, including at the time of injury, during the closed reduction, iatrogenic injury at time of surgery, and during fracture healing (Shin and Ring 2007). This highlights the importance of a comprehensive clinical exam throughout a patient’s care, particularly before and after an intervention.
Surgeons who choose to address the ulnar nerve at the time of ORIF most often perform an in situ neurolysis or anterior subcutaneous transposition. In situ neurolysis is thought to release any direct impingement, or “kink” of the nerve. Anterior subcutaneous transposition involves direct release of the nerve in the cubital tunnel with transposition to the anterior subcutaneous tissue. The benefits of a transposition include release of incomplete tethering that may kink the nerve, moving the nerve away from impinging structures, and limiting scar formation allowing the nerve to glide in its position (Vazquez et al. 2010). Additionally, it is believed that in patients who are unable to terminally extend the elbow, transposing the nerve anterior to the joint line relieves traction along the nerve.
Despite the stated advantages of intervening with the ulnar nerve at time of ORIF, the literature suggest that handling the nerve puts the tissue at greater risk for direct and/or indirect injury, perineural fibrosis, and disruption of intraneural vascularization (Worden and Ilyas 2012; Chen et al. 2010; Vazquez et al. 2010; Kundel et al. 1996; Krkovič et al. 2006; Wiggers et al. 2012; Shearin et al. 2018). In a retrospective review, Chen et al, compared rates of ulnar neuritis following ORIF with and without ulnar nerve transposition and found a 33% increased likelihood of developing neuritis with transposition – concluding that not only is transposition ineffective at protecting the nerve, it can be harmful (Chen et al. 2010). On the other hand, Kundel et al, found the prevalence of ulnar neuritis to be 27% following neurolysis alone (Kundel et al. 1996). However, in a series by Vazquez et al, they reviewed the records of 69 patients at a single institution undergoing distal humerus ORIF with or without ulnar nerve transposition or in situ neurolysis. Their overall incidence of ulnar nerve dysfunction following distal humerus ORIF to be 10% and 16% at immediate and 12-month follow-up respectively; however, no difference was identified between transposition or neurolysis alone (Vazquez et al. 2010). Ruan et al, evaluated 117 patients undergoing distal humerus ORIF with associated transposition or in situ neurolysis and determined no difference in the incidence of neuropathy following either procedure. However, patients who underwent transposition had a lower rate of complete resolution of symptoms (Ruan et al. 2009).
In a prospective, randomized trial, McKee et al, evaluated ORIF versus total elbow arthroplasty for distal humerus fractures in elderly patients. Their study determined a 20% incidence of ulnar nerve symptoms following transposition in the ORIF cohort (McKee et al. 2009). Similarly, a recent meta-analysis by Shearin and colleagues, revealed an increased incidence of ulnar neuropathy for patients receiving anterior transposition when compared to neurolysis, 25.3% vs 13.5% respectively. They concluded that movement of the nerve requires more handling and thus attributed to more opportunity for devascularization and scar formation (Shearin et al. 2018). More recently, Dehghan et al performed a multicenter randomized controlled trial evaluating the ulnar nerve function for patients receiving in situ neurolysis or anterior subcutaneous transposition in 31 and 27 patients respectively. They determined there was no difference in functional outcome and nerve injury between the two groups; however, they did report high rates of ulnar nerve dysfunction in both groups, which showed significant improvement at the 1-year time point (Dehghan et al. 2021).
Beyond the risk of nerve injury from distal humerus ORIF, there is established literature to suggest that excessive handling of the ulnar nerve during surgical procedures can also lead to ulnar neuritis, in the absence of a concomitant fracture. In a retrospective study by Zhang et al, evaluating outcomes for patients receiving cubital tunnel release for ulnar nerve entrapment, patients who had a transposition presented with significantly greater rate of short-term complications when compared to neurolysis alone (9.6% vs 3.6%, p<0.02) (Zhang, Earp, and Blazar 2017). These results do challenge the notion that transposition may lead to further impingement, however, the stated increase in ulnar nerve injury is present in both cohorts studied , indicating that manipulation alone is enough to produce symptoms.
Despite the compelling evidence that intra-operative manipulation of the nerve is associated with increased rates of ulnar neuritis, there are several situations when handling the nerve may be necessary. Surgical management of the ulnar nerve is indicated for accurate fracture reduction with safe application of implants, pre-existing cubital tunnel syndrome, or concern for hardware impingement. A thorough history and physical exam may help guide the surgeon’s decision making. Similarly, patients should receive counseling on the potential complications associated with intra-operative ulnar nerve manipulation.
In addition to the increased incidence of ulnar neuritis, we report the average time to post-operative diagnosis in patients receiving ulnar nerve transposition, neuroplasty, or neurolysis to be 21 days shorter (p<0.003), than patients without the associated CPT code. The authors believe this can be a result of two separate, but potentially related, circumstance: 1: patients who underwent ulnar nerve transposition, neuroplasty, or neurolysis develop symptoms sooner that patients who do not; or, 2: patients who underwent ulnar nerve transposition, neuroplasty, or neurolysis are more critically evaluated in the post-operative setting for ulnar nerve symptoms. One potential criticism of timing to diagnosis is dependent on when patients are scheduled for follow-up. To address this issue, the authors opted to report the trend in diagnosis over the course of a year under the assumption that patients will have at least one clinic appointment, following a distal humerus open reduction and internal fixation within one year of surgery as is the standard of care.
As with all insurance database studies, there is inherent heterogeneity introduced through multiple payer systems and institutional ICD/CPT coding procedures. The authors recognize that, despite diligent efforts to enhance the consistency and reliability of procedure coding, a lack of standardization persists regarding when surgeons opt to code specific procedures poses a limitation to how these results may be interpreted. Further limitations include the lack of laterality with CPT/ICD-9 coding does not allow for specific granularity of the injured extremity. However, this study was performed under the assumption that ulnar neuritis is developed in the operative extremity given that patients with a diagnosis of ulnar neuritis prior to injury were excluded from the analysis. Additionally, this limitation is consistent in both cohorts therefore minimizing the effect on our results.
The mechanism and severity of injury is not represented in this study, as well as hospital course at index injury, i.e., closed reduction and other associated injuries, that may have increased risk injury to the nerve. For this reason, we focused our conclusions based on delayed diagnosis of ulnar neuritis, understanding that the immediate peri-operative phase may result in nerve injury. This limitation suggests a promising avenue for future research to further characterize sub-groups of patients based on fracture pattern, severity, and fixation strategy and how that may influence the rates of ulnar neuritis associated with this injury. Lastly, the authors reiterate the conclusions drawn from this study do not distinguish between neurolysis and anterior subcutaneous transposition. Instead, we assert that minimizing manipulation of the nerve likely has a protective effect on patients in terms of developing ulnar neuritis.
CONCLUSION
Our review of a large insurance database shows that operative manipulation of the ulnar nerve at time of distal humerus ORIF leads to increased risk of ulnar neuritis in the delayed post-operative phase. Additionally, we found the overall rate of delayed ulnar neuropathy was 5.0% and 9.5% from 2-weeks to 1-year post-operatively for the no manipulation and manipulation cohorts, respectively. As such limited manipulation of the ulnar nerve to only what is required for surgical exposure and safe reduction and instrumentation of the fracture is recommended. Lastly, the prevalence of this phenomenon is significant at 5.5% and surgeons should routinely evaluate patients regardless of treatment strategy.