












Introduction
The increasing number of total hip arthroplasty (THA) procedures is putting a significant burden on many healthcare systems. Surgeons play a leading role in reducing this burden by minimizing operating room (OR) costs with improved procedural efficiency and quality of care (Fong, Smith, and Langerman 2016; Kurtz et al. 2007; Ackerman et al. 2019; Astolfi, Lorenzoni, and Oderkirk 2012). Technology is mainly introduced to improve accuracy, reproducibility, and efficiency of THA. However, 66% of arthroplasty surgeons experience a work-related injury indicating that joint reconstruction procedures are physically demanding for the surgeon (Alqahtani, Alzahrani, and Tanzer 2016; Epstein et al. 2018; McQuivey et al. 2021). Therefore, technology that supports the surgeon’s ergonomics might reduce the psycho-physiological fatigue.
Long-term survivorship of cementless components can only be achieved with optimized preparation of the femoral canal which allows for optimal component stability and ingrowth. The most optimal broaching technique requires good control of mallet velocity and optimal load transmission along with rotational stability of the broach (Preutenborbeck, Reuter, and Ferrari 2020). With manual impaction, variability in impact velocity and load distribution is inevitable, especially when the surgeon is tired. This variability might be neutralized with an automated impaction device that creates a consistent impaction force with reproducible load transmission and without having to repeatedly swing the mallet (Konow et al. 2022). To perfectly hit the impaction device with the mallet, surgeons often use postural positions that are ergonomically not optimal. This might lead to significant fatigue at the end of a procedure or the operating day (Ferrari et al. 2021).
Surgeons endure prolonged periods of demanding cognitive and physical activity, resulting in mental and physical fatigue (Grantcharov et al. 2018). After a day of surgery, 85% of surgeons experience ‘moderate to high’ mental fatigue (Maffiuletti and Lepers 2012). The ability to focus on a single goal is enabled by executive cognitive functions such as working memory update, selective inhibition, and mental set shifting (Hofmann, Schmeichel, and Baddeley 2012). Cognitive performance reflects the accuracy and efficiency of (sub)cortical processes that allow external stimuli detection, response selection, preparation, and activation (McMorris 2016). In THA surgery, it refers to the surgeon’s ability to keep their mind clear during surgery. As fatigue develops, cognitive measurements highlight greater impulsive decisions and reduced self-regulatory capacity (Wemm and Wulfert 2017). Muscular fatigue is linked to a low cognitive performance and has negative consequences on surgical performance (Stephenson et al. 2020). Increasing demand for quantity and quality of care make the evaluation of the surgeons’ cognitive performance and mindfulness relevant when enabling technology is introduced.
Automated impaction allows the surgeon to forego a manual mallet and helps to deliver consistent energy. Such a technology may reduce the surgeons’ fatigue during THA procedures and might lead to a more reproducible and accurate femoral broaching. Bhimani et al. showed an 8-minute reduction in OR time with automated impaction (Bhimani et al. 2020). Ferrari et al. showed that muscle fatigue in the upper limb was reduced with automated femoral broaching (Ferrari et al. 2021). However, the effect of automated impaction on ergonomics, hormonal stress levels and psycho-physiological fatigue has not been studied yet. In this study, we investigated whether (1) automated impaction of THA components would lead to improved ergonomics and (2) whether this would be associated with reduced cortisol levels and mental and physical fatigue at the end of an operating day with 10 THA procedures.
Materials and methods
The present study was an observational study of 3 OR days with 10 THA procedures that were conducted from start to finish by one experienced right-handed hip surgeon and one scrub nurse in 2 OR rooms. A total of 30 THA procedures were conducted through the Efficient Direct Anterior (EDA) approach on a regular OR table (Corten, n.d.-a, n.d.-b). Patients scheduled for THA were randomly assigned to the manual group or the automated impaction group. Once the assignment was completed, surgery was planned. Each day, eight unilateral THA and one bilateral THA were performed. A commercially available motorized and automated impaction device (KINCISETM System, Depuy Synthes, J&J, Warsaw, USA) was used in 2 OR days. Manual impaction of all THA components was done for one day. In all patients a Corail stem and Pinnacle cup (Depuy-Synthes, J&J, Warsaw, USA) were used
The surgeon’s posture during cup impaction and femoral broaching was filmed. Postural risk was evaluated by 2 independent observers using RULA (Rapid Upper Limb Assessment) and REBA (Rapid Entire Body Assessment) (Appendix B) (McAtamney and Nigel Corlett 1993; Hignett and McAtamney 2000). The RULA and REBA tools use the worst-case posture at one point in time. Both methods are considered effective to evaluate the risk of biomechanical work-related overload for surgeons (Dale and Fiedler 2020; Aaron et al. 2021; Occhipinti and Colombini 2012). RULA has four risk levels that categorize scores from 1 to 7, while REBA is based on five levels of risk that categorize scores from 1 to 15. To compare scores from two different scales, absolute values are assimilated, as described in previous similar analyses (Table 1) (Micheletti Cremasco et al. 2019).
Psycho-physiological assessment (Appendix A) of the surgeon was done using three computerized and validated cognitive tasks (Simon, Pattern Comparison and Pursuit rotor) and five physical tests (isometric wall-sit, plank-to-fatigue, handgrip, shoulder endurance and a supra-postural task). Figure 1 provides a schematic representation of the experimental design, measurements, and timeline. Each morning and afternoon evaluation session was executed in the same sequence of tests and lasted 70 minutes (± 15 min). Morning and afternoon sessions included (1) the collection of a saliva sample, (2) a self-report of global physical fatigue using a visual analogue scale (VAS: 0 = no fatigue to 10 = severe fatigue), (3) the three cognitive tasks and (4) the five physical tests. The midday session was identical, except that only two out of five physical tests (i.e., handgrip and shoulder endurance) were performed due to time constraints. This session lasted by average 25 minutes. During the afternoon session, the surgeon was required to complete the Perceived Stress Scale (PSS) questionnaire to evaluate his level of perceived stress, as described by Cohen et al (Cohen, Kamarck, and Mermelstein 1983). The surgeon wore a heart rate transmitter belt (OH1, Polar, Kempele, Finland) to integrate his heart rate data throughout the day, including in the OR. He was also instructed to sleep at least 7 hours the night before each day and to avoid caffeinated drinks during the day. One day prior to testing (day 0), a familiarization phase including all the cognitive and physical tests was carried out to prevent a potential learning effect on each of the tasks.
The cortisol level was measured in nine saliva samples at 3 different time points (5h30 am, 12h00 pm and 4h30 pm) with the Salivettes test (Sarstedt-Salivette®). The surgeon was instructed to refrain from eating or drinking anything but water for at least 30 min prior to the collection. Washing his mouth or brushing his teeth was not allowed. The morning sample was taken 15-20 minutes after waking up. All samples were immediately frozen and stored at -20°C before analysis. For saliva assays, a liquefying agent (Sputasol, Thermo Fisher Scientific) was added to 400 µL of saliva samples which were then incubated for 30 min at 37°C. Then, saliva samples were prepared for cortisol measurement using automated solid-phase extraction (Oasis HLB, Waters Ltd, Elstree, Hertfordshire, UK). Salivary extracts were processed by LC–MS/MS, with a Prominence Liquid Chromatography system (Shimadzu, Nakagyo, Japan) and a 5500Qtrap detector (Sciex, DC, USA) for saliva.
Efficiency of the procedures was measured by timing surgical steps and instrumentation flow. A granular analysis from the timestamps and audio data was conducted using standard descriptive statistics. Audio frequency was recorded by use of an iPhone, mounted at the wall of the OR. Sound level was recorded by a calibrated decibel meter (UNI-T UT353 BT) mounted at the ceiling in the center of the OR table, 2m above the floor. The weight of the handheld mallet and KINCISE™ device were measured.
All 27 patients signed an informed consent in accordance with the good clinical practices and the declaration of Helsinki. The protocol of the study was approved by the Medical Ethical Board of Ziekenhuis Oost-Limburg (ref. number Z-2022055).
For normal distributed data, we used a paired t-test. For binary data a chi-squared test was used. A p-value ≤ 0.05 was considered significant.
Results
Surgical performance and ergonomics
Demographic variables are shown in Table 2. No intraoperative fractures were seen. No subsidence was seen in the first year after surgery.
The surgeon’s posture during manual and automated impaction is shown in Figure 6-9. An overview of RULA and REBA scores is shown in Table 6. RULA of manual impaction scored 6 and 5 for socket and stem impaction, respectively, compared to 3 with automated impaction. Similarly, REBA of manual impaction scored 9 and 5, for socket and stem respectively, compared to 4 and 3 with automated impaction. Detailed RULA calculation is attached in Appendix B, Figure 2-9.
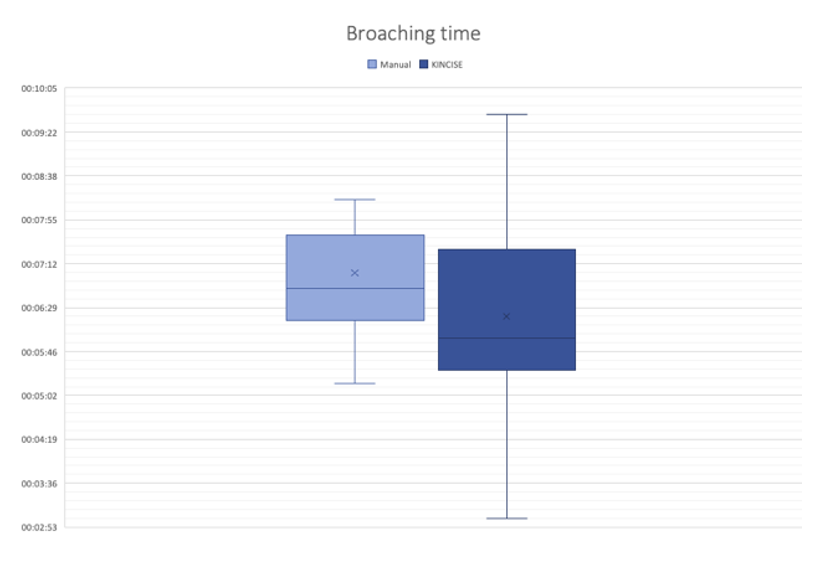
The time from incision until the skin is fully closed was on average 30’59’’ with manual impaction, compared to 29’35’’ with automated impaction. Acetabular reaming and cup placement took on average 5’50’’ with manual impaction and 6’10’’ with automated impaction. Average time for femoral broaching was 7’47’’ with manual impaction compared to 6’58’’ for automated impaction. In four cases (one for manual impaction and three for automated impaction) the Dorr A type femoral canal required canal reaming. Excluding these four cases, broaching time for the manual group was on average 6’20’’ 1’41’‘) and 7’3’’ 1’23’') with automated impaction (Figure 10).
Manual mallet impactions were on average 183 [range, 122-245] strikes per case, with a total of 1832 mallet strikes during the manual impaction day (Figure 9). Automated impaction delivered on average 300 [178-469] hits per case. The sound waves of cup impaction and broaching is shown in Figure 10. The highest sound level was recorded with the standard manual technique (Figure 11). Average sound level of the automated device was lower (64.3 dBA) than manual impaction (68.2 dBA) (Figure 12).
Psycho-physiologic performance
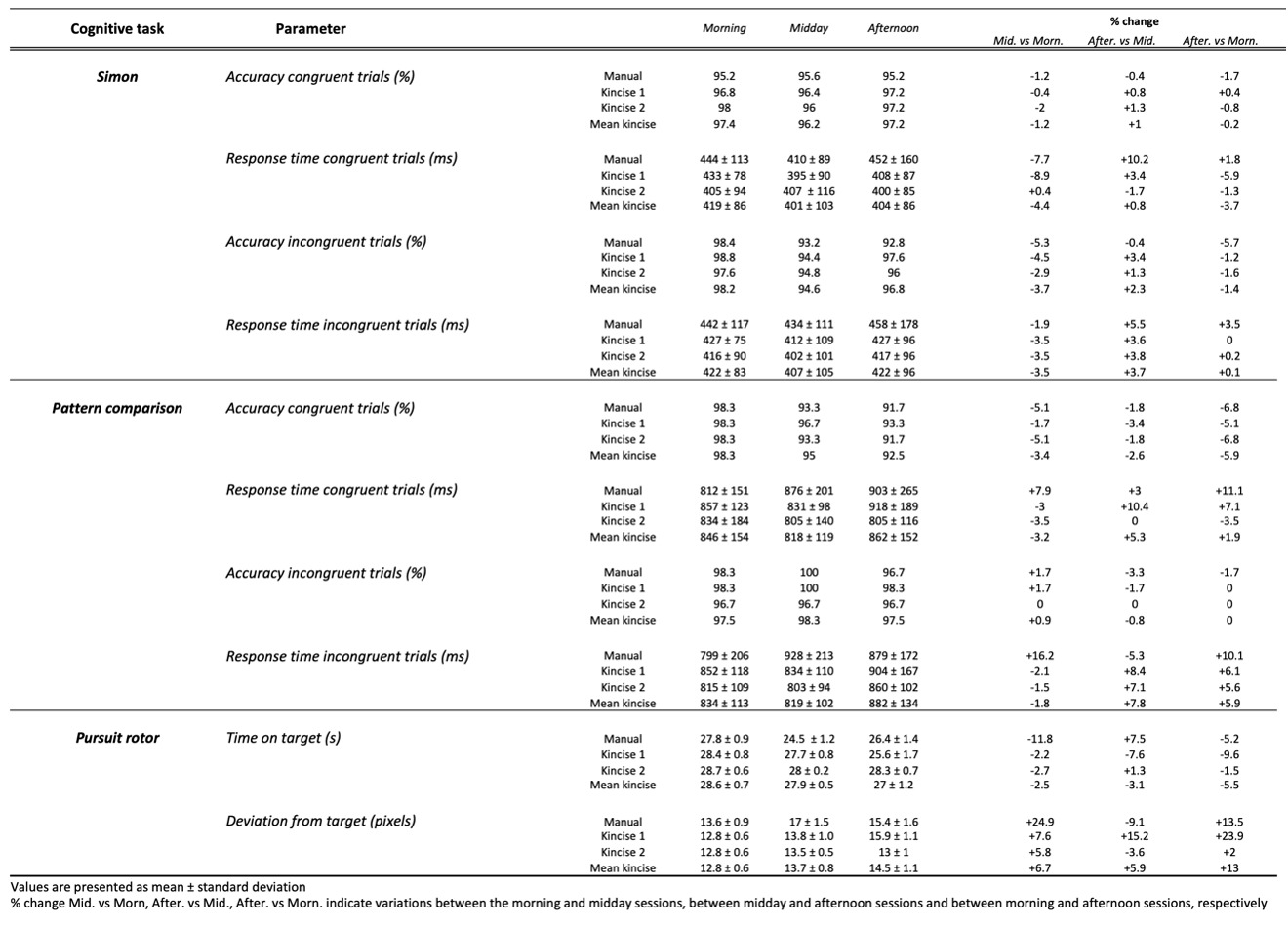
Results of cognitive tasks are presented in Table 3. The Simon task for incongruent trials showed lower cognitive performance in the manual impaction day compared to the automated impaction days, as highlighted by higher RTs (+28ms) and error rates (+2,2%) over the three daily measures. At the end of the day, both the slowest RTs (460ms) and the lowest accuracy (93%) were recorded in manual impaction day. Accuracy was impaired during each midday session. It was accompanied with faster RTs and preserved cognitive control together with the surgeon’s prioritization of speed over accuracy (i.e., the surgeons’ rush between surgeries in the midday session). Focusing on the first quartile of the accuracy function (Figure 2), the error rate for incongruent trials was comparable in morning sessions, but more fast and impulsive errors were observed in midday session during the manual impaction day (Q1 accuracy -13%) compared to the automated impaction days (Q1 accuracy -8%). This pattern was re-iterated at the end day sessions with a reduced accuracy for longer RTs (Q4 accuracy -6%) in the manual impaction day. The Simon task for congruent trials revealed the same trend. Both the longest RTs (430ms) and lowest accuracy rates (96%) were seen during the manual impaction day. The midday sessions showed the same need for speed in the surgeon’s strategy in all cases. But for the end day session, compared with the midday session, an impairment in both RTs (+400ms) and accuracy rates (-1%) was found in the manual impaction day but not in the automated impaction days.
The Pattern comparison task for incongruent trials at end day compared to midday sessions revealed longer RTs in the manual impaction day (+130ms) compared to the automated impaction days (+60ms). The concomitant improvement in accuracy (+2%) in the end day session is caused by the surgeon’s prioritization to accurately perform the task over speed (i.e., the surgeon relaxes after finishing surgery program). However, the disproportional changes in magnitude at the end day session suggest a decline in cognitive performance in the manual and the automated impaction days. Analysis of congruent trials showed a reduced accuracy with proportional increases in RTs during the day. This is caused by a progressive decline in information processing accuracy which was more pronounced in manual impaction day.
The pursuit rotor task results (Table 3) show a reduction in performance over the day in all 3 days. However, a greater time spent on the target (+1.5s) and a smaller target deviation (-1.7 px) was found in the automated impaction days. In addition, the most extreme values of a motoric control decline i.e., the lowest time spent on the target (24.5 s) and the highest target deviation (17 px), were observed during the manual impaction day.
The surgeon’s physical performance (i.e., isometric wall-sit endurance test, plank-to-fatigue test, handgrip test, shoulder endurance test, and a supra-postural task) are presented in Tables 4 and 5. Physical fatigue for most of the tasks was observed during all 3 days. This was characterized by poorer performance in the late afternoon compared to the morning, which was much more salient during the manual impaction day compared to the automated impaction days. For the isometric wall-sit endurance test a 22.9% decrease in time limit between the morning (109 s) and afternoon (84 s) sessions was observed during the manual impaction day. A mean decrease of 10.6% was found in the automated impaction days (117.5 s vs 105 s). A 43.8% decrease in plank-to-fatigue time limit was also observed during the manual impaction day (morning: 128 s; afternoon: 72 s) compared to 2.2% in the automated impaction days (morning: 137 s; afternoon: 134 s).
The estimated time limit (mETL) and delayed onset muscle soreness (DOMS) on the shoulder endurance test decreased linearly over the course of the automated impaction days, while it dropped abruptly between the midday and afternoon sessions during the manual impaction day. DOMS increased slightly in the automated impaction days (morning: 3.15; afternoon: 4.3), whereas it increased substantially during the manual impaction day (morning: 3.8; afternoon: 10), reaching the maximum pain level at the end of the day.
Regarding handgrip data, a small difference between the surgeon’s dominant (i.e., right hand) and non-dominant hand strength was noticed. While both dominant and non-dominant hands showed some decline in force production over the three daily sessions, the pattern of decline was slightly different between hands during the manual impaction day. A strong decrease on the average force produced over the 10 repetitions was observed in the midday session for the dominant hand (28.3 kg; 25.3 kg; 24.7 kg for the morning, midday, and afternoon session, respectively), whereas a strength decrease was only noticed at the afternoon session for the opposite hand (28.5 kg; 29.1 kg; 26.6 kg).
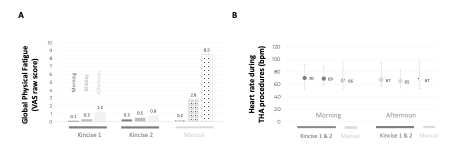
In the supra-postural task, a decrease in the number of taps during the manual impaction day was found (-7.7%), compared to unchanged values during the automated impaction days. Heart rate changes between morning and afternoon were similar during all days (Figure 4B). This decrease in performance was also subjectively experienced via a high level of perceived exertion (+2 points during the manual impaction day compared to +0.5 during the automated impaction days).
In general, these physical data showed a high level of muscular fatigue in the upper limbs, lower limbs, and lumbar muscles. This objectified fatigue is also related to subjective perceptual measures of fatigue (Figure 4A) despite a steady state in recorded heart rate (Figure 4B).
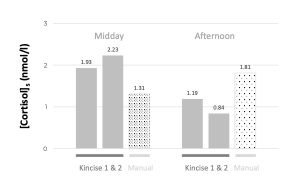
Salivary cortisol levels were highest in the morning (Manual = 8.34 nmol/l; Mean automated impaction days = 8.84 nmol/l). Between midday and afternoon samples, an increase of 38.2% salivary cortisol concentration was observed during the manual impaction day, whereas a mean decrease of 51.2% was found during the automated impaction days (Figure 5). The PSS questionnaire demonstrated a higher stress score during the manual (PSS 7) impaction day compared to the automated impaction days (mean PSS 3).
Discussion
Surgeons must remain lucid to make accurate decisions throughout a busy OR day. A THA procedure is cognitively demanding and external factors have a direct impact on the cognitive performance (Yule et al. 2006; Marquardt et al. 2015). This study demonstrated that manual impaction of THA components is associated with impaired ergonomics for the surgeon which leads to cognitive and physical exhaustion. In addition, the 1832 mallet swings also affected the muscular fatigue. Although the automated impaction device is heavier than the mallet and surgery time is equal, the exhaustion of the surgeon during the automated impaction days was lower than during the manual impaction day. We believe that this finding is directly related to the improved ergonomics that were found when the automated impaction device was used.
During surgery, a constant search for ideal surgical performance often undermines a good ergonomic position. With manual impaction, REBA score matched ‘high risk’ for cup placement and ‘medium’ for femoral broaching, while RULA scores matched 'high risk 'levels for both. By using an automated impaction device, RULA scores improved to ‘medium’ for both cup impaction and femoral broaching, and REBA scores improved to ‘medium’ for cup placement and ‘low’ for femoral broaching. Especially for surgeons with a long career in a high-volume hospital, these findings may be helpful to avoid work-related injuries (Alqahtani, Alzahrani, and Tanzer 2016; Szeto et al. 2009).
Working in a standing position induces muscle fatigue, particularly in the core, the lower and upper limbs (Szeto et al. 2009; Toffola et al. 2009). Both isometric wall-sit and the plank-to-fatigue tests confirm greater fatigue in the lower limb and lumbar muscles. We believe that these postural tasks are impaired due to the decreased ergonomics with manual impaction. In addition, a decrease in mETL in shoulder endurance test and a decrease in grip strength demonstrate muscular fatigue of the anterior deltoid muscle and hand flexor muscles. This can be explained by the 1,832 mallet swings with a 500g mallet. Interestingly, the pattern and the degree of decline in grip strength was different. For the three parameters analyzed (i.e., the average force produced over the 10 repetitions, the maximal peak force, and the area under the force-time curve) at midday session, we observed a decline in force production with manual impaction, whereas with automated impaction a strength maintenance is observed, only slightly decreasing at the end of the day. These findings are consistent with recent data on electromyographic signals, showing a higher reduction in muscle activation and fatigue of the biceps brachii, brachioradialis, and trapezius after manual impactions compared to automated impactions (Ferrari et al. 2021). These results suggest that the automated impaction device reduces muscle fatigue in the upper limb.
The surgeon’s cognitive performance on a selective inhibition task (Simon task) was impaired during the manual impaction day, while it is almost maintained using during the automated impaction days. The impaired performance for congruent trials indicates that even simple cognitive processes could be affected. Simple processes are commonly reported to be unaffected since they mainly require autonomous and perceptive/attentional computations and a limited executive component (Eriksen and Eriksen 1974). Also, the Pattern comparison results show reduced efficiency for information processing during the manual impaction day. Sustained attention and pattern comparison require working memory to implement and maintain a specific task-set focus. In addition, manual impaction takes more effort to perform the pursuit rotor task, appearing that the surgeon’s psychomotor performance is impaired.
With manual impaction, cortisol levels increased between midday and afternoon sessions, while it decreased using an automated impaction device. Although manual impaction led to a higher score on the PSS questionnaire, it is still considered as ‘low stress’ according to Cohen et al (Cohen, Kamarck, and Mermelstein 1983). However, these results confirm that a complex surgical procedure, time pressure and distractions, are substantial stressors in surgeons (Arora et al. 2010) that influences hormonal responses (Tsigos et al. 2000).
Learning surgical techniques is a long and complex process (Nairn et al. 2021). Just like athletes, surgical performance is improved by experience, reflected by a reduction in operating time, infection rate and complications (Foissey et al. 2020). Results of cognitive and physical data in this study are comparable with data collected from trained athletes. In twelve national pentathlon team athletes, Simon task accuracy of 0.98 for congruent trials (vs 0.97 for manual and 0.98 automated impaction in our study) and an accuracy of 0.96 for incongruent trials (vs 0.98 and 0.97, respectively) is reported (Pomportes et al. 2019). Using the same supra-postural task, the surgeon in this study performed better (36 ±2.6 taps) than 24 physically young adults (age 23.9 ± 4.0 years; 22 ± 4 taps) (de-Oliveira et al. 2021). In a 10-repetition dynamic grip experiment as in our study, an average force of 34.8 kg ± 6.9 (vs 28.4 ± 3.6 in the morning session of our study) for the dominant hand and an average force of 34.9 kg ± 9.8 (vs 29.6 ± 3.9 ) for the opposite hand was found (Nicolay and Walker 2005). Finally, trained subjects have lower cortisol levels than untrained subjects, with baseline values in trained subjects comparable to those observed in our study ([cortisol]Trained men = 11.5 nmol/l vs [cortisol]Manual = 8.3 nmol/l vs [cortisol]Mean automated impaction = 8.8 nmol/l) (Rimmele et al. 2007). We conclude that high volume THA surgery requires a good physical and mental condition. Surgical performance can be compared to athletic performance.
Arthroplasty surgery is a working environment with significant noise exposure (J. S. Palmer et al. 2021). The prevalence of hearing loss among arthroplasty surgeons is higher than in their non-surgical colleagues (J. Palmer et al. 2021). Furthermore, noise can have an impact on mental fatigue as well. Therefore, noise generated during arthroplasty surgery should be managed to create safer working conditions. In this series, audio analysis shows a lower sound level with an automated device, compared with manual impaction.
However, this study is also prone to several limitations. First, the data presented in this pilot study represent those of only one surgeon with an extensive experience in both automated and manual component impaction. Since only one particular approach was used and as positioning is different for different approaches, our results may not be generalizable. However, surgical experience is essential for a smooth-running procedure. Surgeons who meet these requirements are not numerous and sample size was adjusted to available funding. Although the design of this observational study does not allow for inferential statistics, the encouraging results reported herein could pave the way for further multicentric research. Second, the surgeon was physically (i.e., 2 cycling sessions per week) and mentally fit. This might have biased stress levels or even might have clouded additional positive effects of an automated device. Also, learning a new surgical technique could be a stressor for a less experienced surgeon, while stress decreases with experience (Kautzner et al. 2017; Yamamoto et al. 1999). Therefore, future studies should focus on the effect of backgrounds, age, and nursing staff on surgeon’s stress level, cognitive and physical fatigue. Third, the surgeon could not be blinded to manual impaction versus automated impaction so unconscious bias during outcomes requiring “effort” may bias outcomes and favor automated impaction. Finally, it is important to emphasize that not many surgeons are able to conduct ten THA a day. Therefore, these results are of particular interest to high-volume centers. However, we also noticed already impairment in some tests during the midday session in the manual impaction day indicating that even at a more regular volume of 6 THA, manual impaction affected some physical tests.
Conclusion
High volume joint reconstruction surgery is comparable to athletic performance. Automated impaction improves the surgeon’s ergonomics and lowers the surgeon’s stress, cognitive and physical fatigue throughout one operating day.

_and_subject.png)



_time_effectively_completed_over_the_3_min.png)
_perceived_physical_fatigue_for_the_three_sessions_(morning__midday_and_afternoon)_and_t.png)
_during_.png)


.png)

