




INTRODUCTION
The World Health Organization (WHO) declared SARS-CoV-2 (COVID-19) a worldwide pandemic on March 10th, 2020 (Cucinotta and Vanelli 2020). In the brief period immediately after this announcement, the United States Surgeon General recommended cancellation of all elective surgeries. The Centers for Medicare & Medicaid Services (CMS) and the American Academy of Orthopedic Surgeons (AAOS) soon supported this recommendation (Brown et al. 2020).
A survey among American Academy of Hip and Knee Surgeons (AAHKS) found that 92% of hospitals had stopped performing elective arthroplasty by April 2020 (“AAHKS Surveys Members on COVID-19 Impact” 2020). The Annual Joint Report Registry’s (AJRR) 2020 report corroborated this reduction. Between January to April 2020, hip and knee procedures performed in hospitals decreased 89% and those performed in ambulatory surgical centers (ASC) decreased 96% (American Joint Replacement Registry (AJRR): 2020 Annual Report 2020). This suspension led to dramatic backlogs in arthroplasty cases. The proposed catch-up time was calculated to range from 9 months to 35 months from April 2020 (Wilson et al. 2020). Even with the lifting of the suspension, a continued backlog was anticipated to persist due to staffing shortages and supply chain challenges.
Furthermore, the reduction in elective TKA caused by the pandemic came at a time when TKA was increasingly being performed in the outpatient setting. CMS removed total knee arthroplasty (TKA) from the inpatient only list in January 2018 (The Federal Register 2017). Following this decision, there was a rapid transition toward outpatient TKA. Studies have shown the cost-savings of outpatient arthroplasty with minimal effect on complications (Jain, Jain, and Aggarwal 2020; Smith et al. 2021). Many viewed the COVID-19 pandemic as a catalyst for the transition to outpatient arthroplasty because it was thought to potentially reduce patients’ exposure to COVID-19 and helped to relieve the financial burden associated with the loss of volume at the onset of the pandemic (Gleicher et al. 2021). However, changes in overall and outpatient TKA volume throughout the recovery from the COVID-19 pandemic remain poorly understood.
Therefore, the purpose of this study was to observe how the overall and outpatient TKA volume changed throughout the period spanning the COVID-19 pandemic. We hypothesized that there would be a slow transition to normal volume, with disruptions caused by restrictions coinciding with spikes in COVID-19 cases. Additionally, we expected to observe a rapid transition to outpatient TKA beyond what would have been predicted by pre-pandemic trends.

METHODS
Database
A retrospective analysis was conducted using the PearlDiver (Mariner Dataset) Database (10435 Marble Creek Circle Colorado Springs, CO 80908). The Mariner dataset contains over 150 million patient all payer claims information from January 2010 to April 2021. The dataset includes claims information from a variety of institutions including hospitals, skilled nursing facilities, outpatient rehabilitation facilities, ambulatory surgical centers, and clinic/office visits. PearlDiver only releases de-identified patient information. Therefore, this study was exempt from Institutional Review Board Approval.
Patient Selection: Inclusion/Exclusion
Patients were identified if they underwent an elective TKA using Current Procedural Terminology Codes (CPT) 27447 between January 2018 and April 2021. January 2018 was designated as the start date of the study because it corresponded with the removal of TKA from the CMS inpatient-only list, which would otherwise confound the analysis of outpatient TKA volume. International Classification of Diseases (ICD) procedure codes were not used to identify TKA volume as they do not contain records of outpatient procedures. Patients were excluded if they were less than 18 years old or if they underwent lower extremity arthroplasty for non-elective indications such as malignant neoplasms based on ICD 9/10 diagnosis codes (ICD-9-D-140, ICD-10-D-239, ICD-9-D-C00, ICD-9-D-D49).
Observed and Expected Volume
Monthly TKA volume was observed from January 2018 to April 2021. The proportion of TKA performed on an outpatient basis was calculated for each month by dividing the number of TKA cases where the length of stay was zero days by the total TKA volume that month.
To observe the change in monthly pre-pandemic volume and proportion of TKA performed in the outpatient setting, the rate of change for volume and proportion was calculated using the compounded monthly growth rate (CMGR) based on the following equation: CMGR = (Y2 value/Y1 value)^1/(Y2 – Y1)^ -1. Y1 is the first month of the analysis and Y2 is the final month. The CMGR is a validated metric of change that is commonly used to analyze trends due to its ability to reduce the impact of short-term fluctuations on overall trends (Eltorai et al. 2018).
Statistical Analysis
To observe the impact of the pandemic on the change in volume and proportion of TKA performed in the outpatient setting, historical data from January 2018 to February 2020 was used as a baseline. A linear regression analysis controlling for seasonal variation was conducted using this historical data to predict the expected volume and proportion of outpatient TKA from March 2020 to April 2021. 95% Confidence intervals were included for the expected volume and proportion in the outpatient setting. If the observed volume or proportion did not fall within the 95% confidence interval, it was determined that there was a statistically significant difference between the observed and expected volume or proportion for that month. Adjusted R2’s were used to evaluate the performance of the linear forecasting models. All analysis was performed in Microsoft Excel (Microsoft Corporation 2018).
Source of Funding
No Funding was received in support of this study.

RESULTS
Pre-Pandemic: Volume and Change in Outpatient Proportion
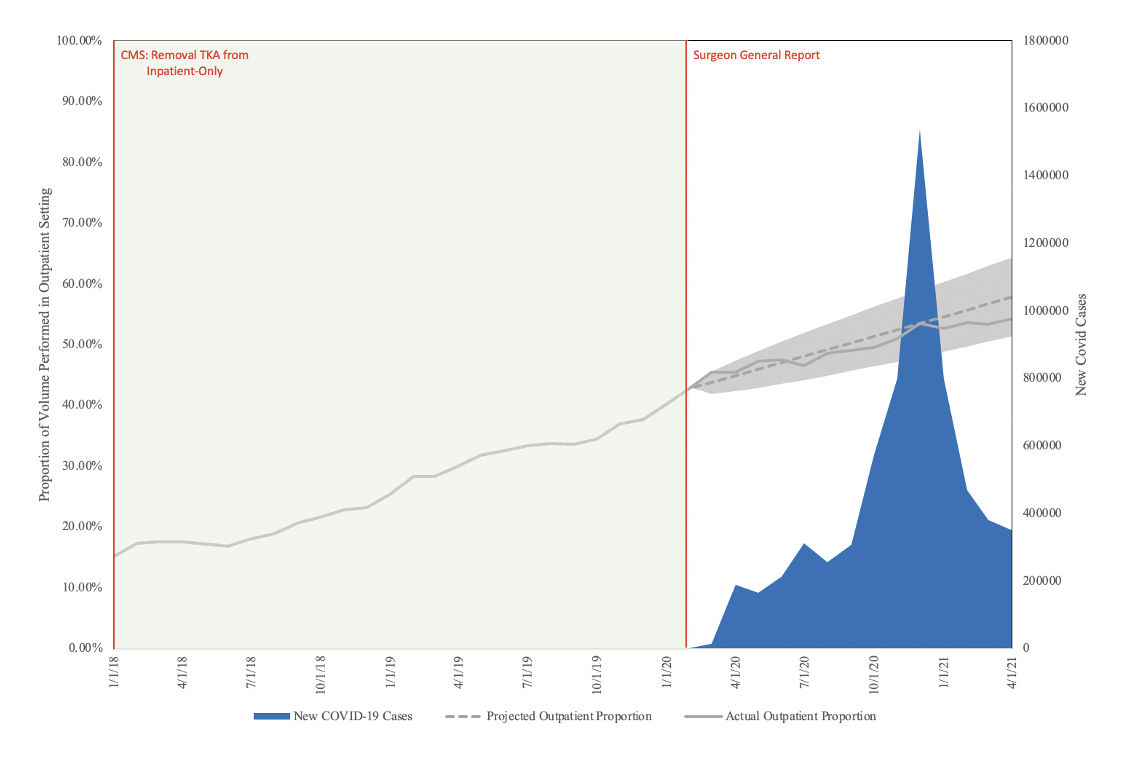
Between January 2018 to February 2020, the volume of elective TKA increased by 17.74% from 12,497 in January 2018 to 14,715 in February 2020, with a CMGR of +0.63% (Figure 1; Table 1). Between January 2018 to February 2020, the percentage of elective TKA volume performed in the outpatient setting increased by 183.44% from 15.09% in January 2018 to 42.82% in December 2020, with a CMGR +4.09% (Figure 2; Table 2).


Pandemic: TKA Volume and Change in Outpatient Proportion
A linear projection model using historical data from January 2018 to February 2020 and controlling for seasonal variation was created. The adjusted R2 for the model was 0.846. This model was conducted to identify deviations in the observed TKA volume from the model predictions during the pandemic. Between March 2020 to April 2020 (first wave of COVID-19 and Surgeon General recommendation), there was a significant decrease in TKA volume by 96.4% (Figure 1; Table 1). By June 2020, total TKA volume reached the expected number based on the linear regression model (Actual: 15,692; Expected: 15,586 (95% CI: 13,345-17,738; Figure 1; Table 1). Between June and August 2020 (second wave of COVID-19), there was a gradual but non-significant decrease in TKA volume by 7.7%. From October 2020 to January 2021 (third wave of COVID-19), there was another significant decrease in TKA volume by 28.1% (Figure 1; Table 1). By March 2021, total observed TKA volume returned to the expected volume (Actual: 16,227; Expected: 17,181 (95% CI: 14,540-19,823; Figure 1; Table 1).
A linear projection model was conducted to observe the change in the expected proportion of TKA volume performed in the outpatient setting during the pandemic. The adjusted R2 for the model was 0.991. Throughout the pandemic interval, the observed proportion of TKA volume performed in the outpatient setting did not deviate from the expected proportion throughout the entirety of the pandemic (Figure 2; Table 2).

DISCUSSION
Our study showed a significant decrease in TKA procedures below expected volumes, in the first and third waves of the pandemic. However, volume rapidly returned to the expected level following these waves. Thus far, there has been no period in which a rebound effect was observed by which TKA volume significantly exceeded the expected level. Additionally, the study found no significant deviation in the proportion of TKA cases performed on an outpatient basis compared to what would have been expected based on pre-pandemic trends.
The rate of change in volume during the pandemic we found during the pandemic is congruent with a prior study observing the national inpatient change in volume (Heckmann et al. 2022). However, unlike our study, this study showed that arthroplasty volume still did not return to pre-pandemic levels by December 2020 when compared to the average historical monthly inpatient volume from 2017 to 2019. A notable difference of this study compared to ours is that there was no accounting for outpatient arthroplasty procedures. Following the CMS’ removal of TKA from the inpatient only list in January 2018, there was an increased transition of TKA to the outpatient setting. This study corroborated this transition, showing a 183.44% increase in the proportion of TKA performed in the outpatient setting from January 2018 to February 2020. Therefore, the utilization of inpatient only data is limited when assessing the change in current TKA volume.
Nonetheless, we did not expect this rapid return in volume to pre-pandemic numbers following the suspension. Studies published early in the pandemic predicted a persistent decrease in volume compared to historical projections, with effects expected to last for years to come. One justification for this predicted persistent decrease was an increased prioritization of patient optimization and selection for surgery to ensure high quality outcomes (O’Connor et al. 2020). The postoperative complications associated with readmissions can lead to excessive resource utilization, decreasing the supply of resources to COVID-19 patients. Another rationale was a proposed decrease in patient demand for TKA (Landy et al. 2020). A Google trends analysis showed that the public interest in knee replacements decreased during the pandemic. This was attributed to the fear of COVID-19 exposure and its associated complications among the general public. Lastly, as there was a backlog in all elective surgeries, there was an anticipated delay in returning to TKA volume as other non-arthroplasty surgeries would be prioritized by health systems and patients (COVIDSurg Collaborative 2020).
Despite these predictions and justifications, our study showed a rapid increase in arthroplasty volume back to normal expected pre-pandemic levels by June 2020. This is in line with recently published studies which have suggested that arthroplasty volume is returning to pre-pandemic levels. Surveillance of AAHKS members showed that once elective surgeries were reinstated, most surgeons reported no restrictions on their surgeries and believed that they were adapting to the challenges of COVID-19 successfully (Stambough et al. 2021). Although limited by their small sample of hip and knee volume, data from AJRR also showed a resumption in hip and knee volume to pre-pandemic numbers by June 2020. The rapid return to pre-pandemic levels was believed to be attributed to an increased transition from the inpatient setting to the outpatient setting as well as from hospitals to ambulatory surgical centers (ASC) (O’Connor et al. 2020).
Outpatient arthroplasty offered many benefits in the pandemic period because it reduced hospital resource utilization and potential exposure to COVID-19 by patients. ASC’s also don’t have to compete for resources such as intensive care unit beds and ventilators, and staff, who were in limited supply at the beginning and peak of the pandemic.. However, our study showed that the change in proportion of outpatient TKA followed the expected trajectory if the pandemic had not happened.
There are several possible reasons that a proportional shift to outpatient TKA was not observed in the present study. First, at the onset of the pandemic, a substantial transition to outpatient arthroplasty was already underway following removal of TKA from the inpatient-only list in January 2018. Additionally, there are many patients who are not candidates for outpatient TKA. Reasons for this include need for rehabilitation services to achieve sufficient ambulatory capacity to function at home, absence of social supports, and medical comorbidities requiring monitoring in the inpatient setting (Moore et al. 2020). These factors limit the potential for rapid growth in the proportion of TKA surgeries performed on an outpatient basis. However, as initiatives such as pre-rehabilitation, optimization of preoperative comorbidities, and outpatient monitoring of TKA patients are more widespread, the patient population eligible for outpatient arthroplasty is expected to grow (Peacock et al. 2022). Nonetheless, the already observed transition to outpatient TKA following the CMS changes can explain how TKA volume was able to return to the expected volume so quickly.
This study has several strengths. This is the first national database study to observe the change in knee arthroplasty volume during the COVID-19 pandemic until April of 2021. Additionally, this is the first study that can observe and comment on the change in outpatient arthroplasty as many databases are limited to only inpatient data. There are also limitations to this study, mostly attributed to the utilization of the national insurance claims database. PearlDiver is limited to the utilization of billing codes and thus relies on the accurate coding of these diagnoses and procedure codes. Additionally, we are limited to the codes and filters provided by PearlDiver. Among these filters, we are unable to extrapolate socioeconomic status among patients. Additionally, although PearlDiver contains information from ambulatory surgical centers, the database is unable to filter based on location of services. Future studies can observe whether there was any increase in the utilization of ambulatory surgical centers during the pandemic. This study only observed the impact of COVID-19 on TKA and not total hip arthroplasty (THA). Many studies have been combining these two procedures as their volume typically follows each other. However, we did not observe the change in THA volume as the ruling by CMS to remove THA from in-patient only list directly overlaps with that of the COVID-19 pandemic. Therefore, we would not be able to discern any changes related to the pandemic or the CMS ruling specifically.

CONCLUSION
This study showed a rapid return to pre-pandemic TKA volume following the suspension of elective surgeries in March of 2020. No rebound increase in TKA volume was observed over the study period. The transition toward outpatient TKA continued during the observed pandemic period, though growth was in line with projections from the pre-pandemic period.