

Introduction
Rotator cuff tears are one of the most common surgical conditions affecting the shoulder, with greater than 460,000 surgeries performed annually. While many patients do well, there is still a significant portion of patients who experience either failure of repair or re-tearing of their rotator cuff, with rates ranging from 3.9-26.8% in those with small or medium sized tears, up to as high as 94% in patients with large or massive tears (Longo et al. 2021; Flurin et al. 2013; H. M. Kim et al. 2014; Galatz et al. 2004; Inagaki et al. 2023; Wang et al. 2023). One solution to address this problem has been the development of scaffolds. These have been primarily developed to lie over the rotator cuff and provide a framework for the new tendon to grow along (Gillespie, Knapik, and Akkus 2016; Cobb et al. 2022; Ricchetti et al. 2012). Early synthetic patches had different biomechanics than native tissue, presenting the concern that they may lead to stress shielding thereby preventing physiologic loads from reaching the tissue (Cobb et al. 2022). Newer nano-scaffolds, which more closely mimic the native extracellular matrix (ECM) structure, have been shown to support cellular infiltration and migration and facilitate improved tissue regeneration at the enthesis (W. Kim et al. 2020). In addition, the regenerative potential of the scaffold can be further supported thru its degradative process by promoting growth factors that enhance the pro-healing stimulus and lessen the fibrotic scar response (W. Kim et al. 2020; Sensini et al. 2018). Several studies have demonstrated an improvement in collagen thickness and organization, but clinical studies are currently lacking (Beason et al. 2012; Zhao et al. 2015). In addition, many of the original scaffolds were designed to be placed over the bursal side of the repair and, therefore, not beneficial at the enthesis where the healing actually occurs
A synthetic nanofiber scaffold consisting of a bioabsorbable biphasic polyglycolic acid (PGA) and poly-L-lactide-co-ε-caprolactone (PLCL) polymer (Rotium, Atreon Orthopedics) was developed to be placed at the bone-tendon interface prior to cuff repair so that the cuff itself holds the scaffold in place. In placing the scaffold at the juxtaposition of the tendon and bone it was postulated that this would improve tendon healing and help promote a more natural tendon reattachment at the enthesis. This was proven in a recently published animal study, where histological analysis after rotator cuff repair in a sheep model treated with and without an interpositional scaffold resulted in the formation of Sharpey-like fibers at 12 weeks in those treated with the scaffold compared to no Sharpey-like fibers in those treated without (Romeo et al. 2022). In addition, repairs treated with the scaffold had higher ultimate failure load and stress at 6 to 12 weeks post-operatively compared to those treated with repair alone.
Recent data assessing the use of this interpositional scaffold in human subjects has shown only a 9% failure rate at 3 months, with no additional complications noted (Seetharam et al. 2022). However until this time, comparative data has been lacking. We currently present a single practitioner’s data pulled from a multicenter randomized prospective registry comparing double row rotator cuff repair in patients greater than 55 years treated with and without an interpositional scaffold

Prior to study initiation, this study received institutional review board approval at all enrolling sites and was enrolled at ClinicalTrials.gov (NCT04325789). Patients with full thickness superior rotator cuff tears as determined on preoperative magnetic resonance imaging (MRI) scans and confirmed intraoperatively were screened to see if they met inclusion and exclusion criteria. Inclusion criteria were: (1) Age > 55 years with full thickness superior rotator cuff tear; (2) minimum one year clinical and radiographic follow-up; and (3) post-operative MRI obtained minimum 4 months post-operatively to assess for healing. Exclusion criteria included revision rotator cuff surgery, partial rotator cuff repairs, current tobacco use, presence of massive rotator cuff tears, and those patients lacking insufficient follow-up. Patients who met eligibility criteria and agreed to participate were randomized at the time of surgery into either a treatment group consisting of double row rotator cuff repair augmented with an interpositional nanofiber scaffold (scaffold group) or a control group where a standard double-row repair without augmentation (control group) was performed. Randomization was performed by pulling an envelope at the time of surgery where graft or no graft was determined. Patients were blinded throughout the study.
The implant is a bioabsorbable biphasic polyglycolic acid (PGA) and poly-L-lactide-co-ε-caprolactone (PLCL) polymer (Rotium, Atreon Orthopedics, Columbus, OH). Implant resorption occurs by 3-6 months.
Technique
All procedures were performed by a single fellowship-trained surgeon. All patients underwent general anesthesia and were positioned in the beach chair position. Diagnostic arthroscopy of the glenohumeral joint and subacromial space was performed from the posterior portal. All additional procedures performed at the discretion of the treating surgeon were recorded (biceps tenotomy, tenodesis, subacromial decompression, etc.). Full thickness rotator cuff rear was confirmed arthroscopically. The greater tuberosity footprint was cleared of soft tissue and bleeding bone created with a burr or shaver. One or two medial row anchors were inserted depending on the size of the tear at the articular margin. If the patient was randomized to the scaffold group, the sutures from one of the medial row anchors were passed through the center of the scaffold outside the shoulder. The scaffold was then shuttled through the lateral cannula over the sutures to lie directly on the greater tuberosity just over the anchor. The medial row sutures were then passed in both groups through the rotator cuff and a standard double row knotless rotator cuff repair was performed. Patients were placed into a shoulder immobilizer at the end of the procedure.
The intraoperative times were documented from procedure start to procedure end as measured in minutes.
All patients in both groups underwent the same standardized post-operative rehabilitation protocol. Patients were immobilized in a sling for 6 weeks with progression to active range of motion and strengthening by 10 weeks postoperatively.
MRI: MRI was performed on each patient at a minimum of 4 months post-operatively at a single imaging center. T2 coronal and sagittal views were independently reviewed by a musculoskeletal radiologist. Failure of repair was the primary outcome variable, and was defined as those with a Sugaya class of 4 or higher (minor discontinuity in the tendon or major discontinuity in the tendon (Muniandy et al. 2021; Sugaya et al. 2005). Patients without early failure were assessed again at 12 months for late failure via ultrasound.
Follow-up visits were completed at 3, 6, 12, and 24 months (if reached). Missing data at time points were excluded from analysis. At each of these visits as well as the pre-operative visit, range of motion, muscle strength, and clinical outcomes were measured.
Range of motion was measured by an investigator not blinded to the patients’ treatment arm with the use of a goniometer for active forward flexion, external rotation with the arm at the side, abduction, and both external and internal rotation at a 90-degree abduction angle. Isometric strength was measured with a muscle dynamometer (Lafayette Instruments) for forward flexion, external rotation with adducted arm, and internal rotation with adducted arm. The American Shoulder and Elbow Surgeons (ASES) score, Visual Analog Scale (VAS) Pain, and Single Assessment Numeric Evaluation (SANE) were administered on an iPad at each appointment or via email prior to the appointment. Minimal clinically important differences (MCID) were considered as 21.0, 1.5, and 13.0 respectively (D. M. Kim et al. 2020).
This study evaluates a single practitioner’s subset of patients pulled from a prospective randomized control trial, which will follow 240 patients for a minimum of 24 months. This initial data is being presented so that surgeons/colleagues may be aware and consider this data in their own practice.
Statistics: Data were checked for normality and appropriate descriptive statistics were computed for all variables. Chi-square tests and independent t-tests were used to compare patient outcomes based on treatment group and failure of rotator cuff repair. Multivariate regression analysis accounting for the use of intraoperative scaffold and tear size, as well as any variables that were statistically different between failure and non-failure groups were included to determine independent association with failure at final follow-up. Data were analyzed using SPSS Version 27 (IBM Corp., Armonk, NY, USA). All tests were two-tailed and a p-value of less than 0.05 was used to determine significance. Analysis was performed on an intent to treat basis; No patients underwent a treatment that they were not initially randomized to.

Results
30 patients were randomized thus far and have greater than one year follow-up. All patients had supraspinatus tears. Two patients in the control group also had associated infraspinatus tears, one medium and one large. Forty-seven percent of patients in the control group underwent biceps tenodesis and 36% in the scaffold group (p=0.5). There were no demographic differences between groups (Table 1). There was no significant difference in duration of surgery between the control and scaffold groups (53±18 vs 59±16 minutes, p=0.4).
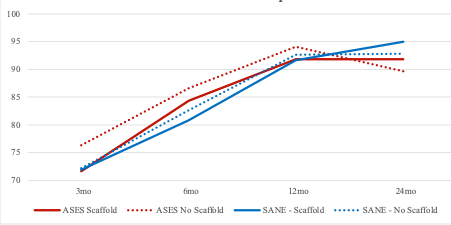
There were improvements in ASES, SANE, and VAS pain scores in both treatment arms at all time points compared to pre-operatively (Figure 1). In patients treated with scaffolds, ASES scores improved by 39.0±12.5, SANE by 39.0±20.8, and VAS pain scores by 4.1±1.7. In patients treated without scaffolds, ASES scores improved by 39.0±15.2, SANE by 41.6±20.4, and VAS pain scores by 4.9±1.7. There were no differences between treatment groups at any time points.

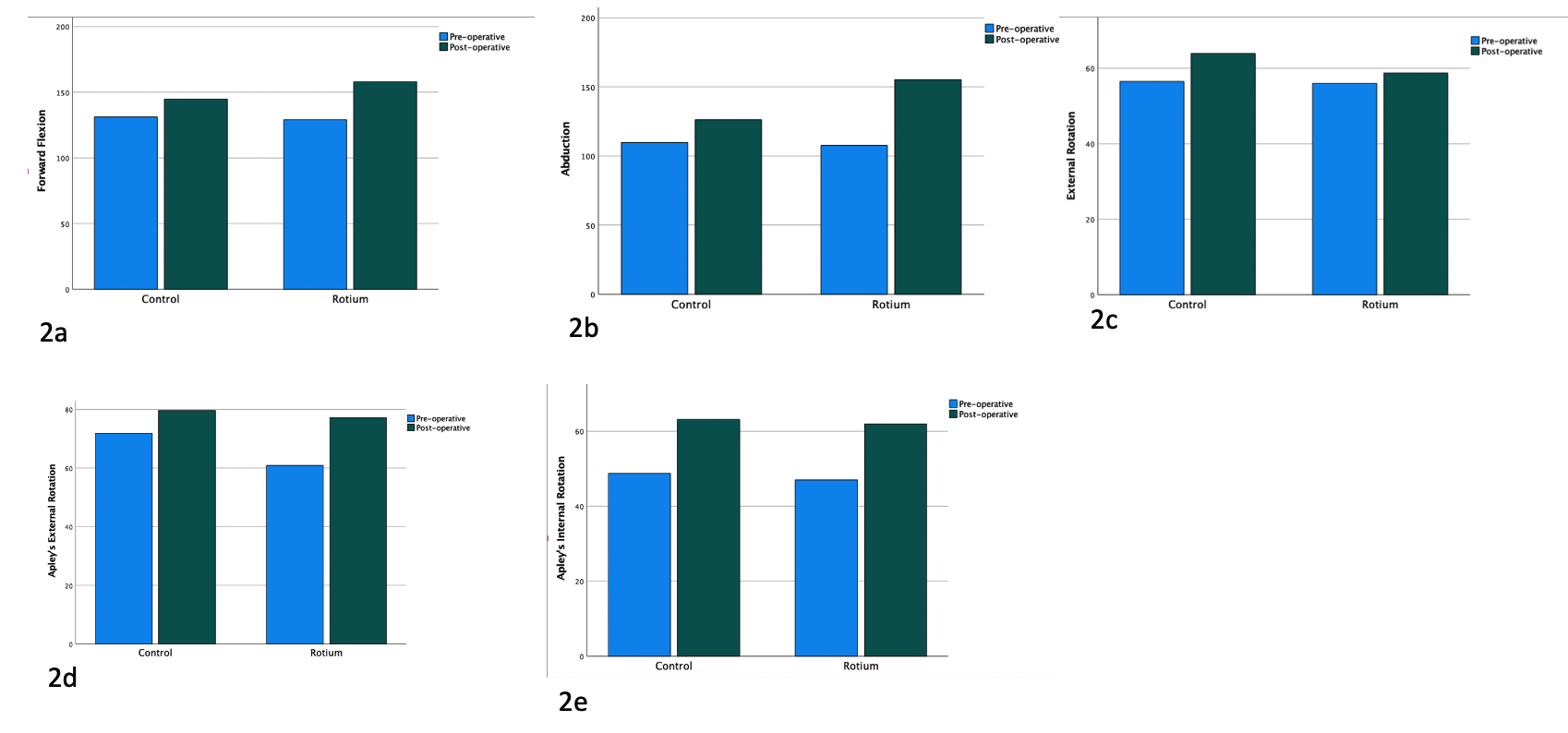
MOTION: There were significant improvements in motion appreciated at 12 months in both groups with the exception of adducted external rotation (Figure 2). Greater mean abduction (155.3 ± 14.7 vs 126.3 ± 25.5) and forward flexion (158.1 ± 8.6 vs 144.8 ± 16.6) were reached in the scaffold group at 12 months; however, this difference resolved by 24 months (Table 2). Apley’s external rotation at three months was noted to be higher in the scaffold group as well, with this difference resolving by the next follow-up.

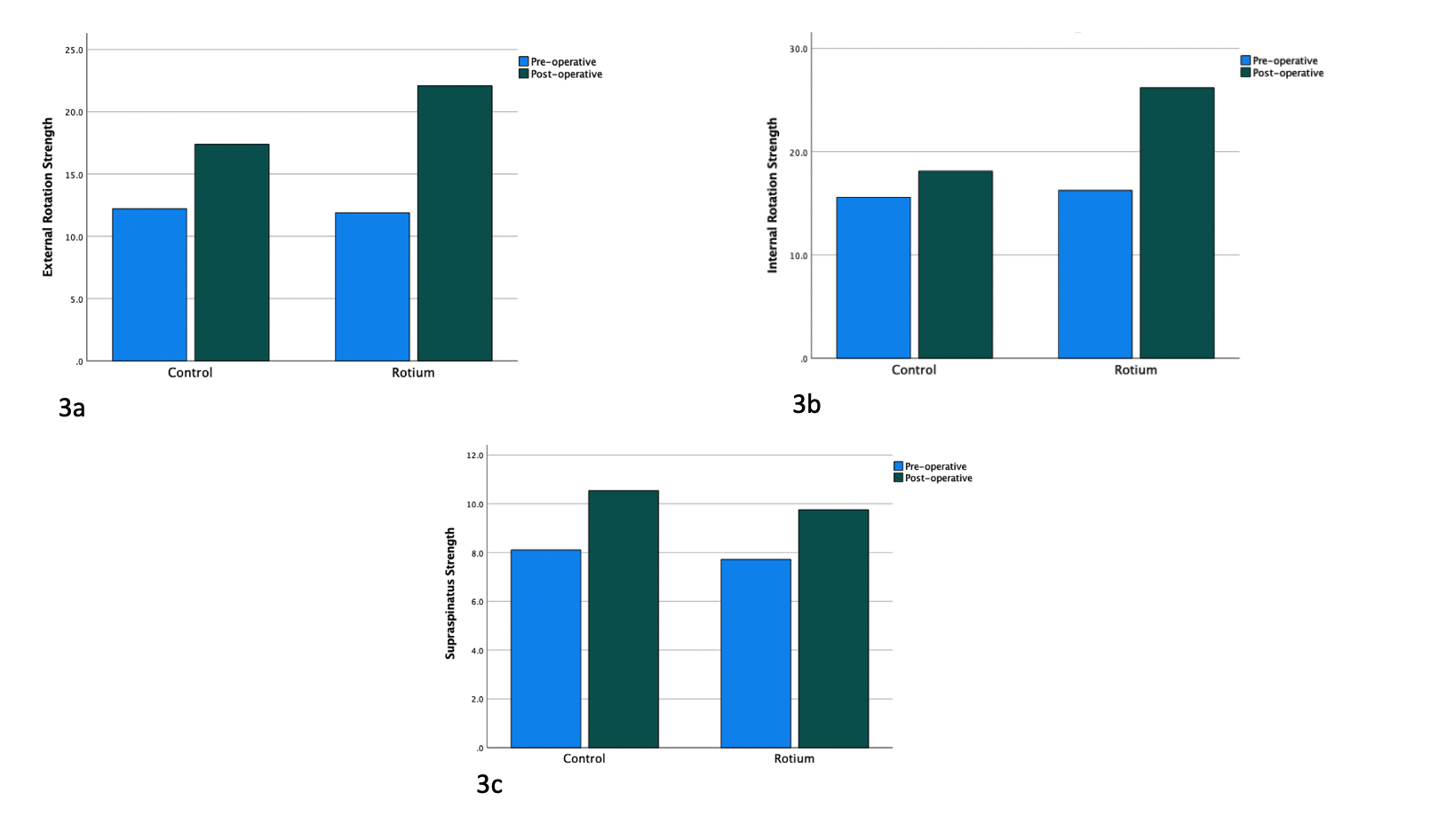
STRENGTH: There were improvements in both treatment arms at all time points compared to pre-operatively (Figure 3). The sole difference between treatment arms is that greater internal rotation was reached in the scaffold group at 12 months (26.2 ± 8.1 vs 18.1 ± 8.2) which resolved by 24 months (Table 2).


Imaging/Failures
There were four early failures in the cohort, three of which were in the control group. By one year, there were a total of nine failures in the cohort, 8 of which were in the control group. The sole failure in the scaffold group was the patient who sustained an early failure. All scaffolds demonstrated complete resorption by the first MRI scan.
Six of the failures were classified as Sugaya 4 and three as 5, including the patient in the scaffold group who experienced failure. Patients who sustained a failure of repair had decreased preoperative external rotation (9.6±3.0 versus 13.1±6.0, p=0.04) (Table 3).
When accounting for statistically and clinically important differences, only the use of a scaffold was predictive of failure ( β=0.70, 95%CI 0.53-0.92).
There were no differences in patient reported outcomes at any time points between those whose repairs failed and those whose did not (Table 4). Patients without a repair failure achieved greater forward flexion at 12 months, abduction at 12 months, and external rotation at 6 months (Table 5). No differences in rotation were noted at other time points, and no difference in strength at any time point was noted.

Discussion
In this study we found an early failure rate of 7% (1/14) without additional late failures in the scaffold group, as compared to 19% (3/16) early failures rising to a total late failure rate of 50% (8/16) in the control group. Despite this, patient reported outcomes and strength were similar between groups. Greater improvements in range of motion were noted in the scaffold group in the first year, but this difference disappeared by year two.
Rates of failure after rotator cuff repair in the literature range widely (Longo et al. 2021; Flurin et al. 2013; H. M. Kim et al. 2014; Galatz et al. 2004). Our cohort sustained a 30% retear rate with 7% in those treated with the scaffold and 50% in those without. Our data is comparable to that in other studies that focused primarily on medium to large sized tears, ranging from 21-94% (Longo et al. 2021; Flurin et al. 2013; H. M. Kim et al. 2014; Galatz et al. 2004; Koh et al. 2011). Koh et al found a 47% retear rate at over two years in patients undergoing arthroscopic single or double row repair for 2-4 cm rotator cuff tears, demonstrating a slightly higher rate at a similar time point for similar tear sizes (Koh et al. 2011).
Bushnell et al evaluated the retear rate after rotator cuff repair with the use of a bovine collagen implant for medium and large tears (Bushnell et al. 2022). They reported a retear rate of 20.8% noted on MRI, as well as two possible implant-related complications. Another study of forty-four patients undergoing double-row repair of medium- to massive- rotator cuff tears with porcine patch augmentation had a failure rate of 15.9%, which was associated with larger tears (Consigliere et al. 2021). Patients treated with a poly-propylene patch to augment rotator cuff repair had a one year re-tear rate of 17% compared to 41% in a control group treated without augmentation (Ciampi et al. 2014).
It has been well described that despite development of a radiographic tear postoperatively, patients still report better pain and functional outcomes compared to preoperatively, and frequently with outcomes similar to patients who did not develop a tear (Bushnell et al. 2022; Consigliere et al. 2021; K. C. Kim, Shin, and Lee 2012). Our patients noted significant improvements in pain and outcomes at all times points, exceeding the MCID for the ASES, SANE, and VAS pain scores. Similar results have been reported in patients treated with scaffolds. In Bushnell et al’s cohort, over 90% of patients, regardless of repair failure, reported improvements in ASES and Constant-Murley shoulder scores greater than the MCID (Bushnell et al. 2022), while patients treated with porcine patch augmentation reported improvements in functional outcomes regardless of tear size or failure (Consigliere et al. 2021). One study however did report that patients treated with polypropylene patch augmentation reported higher UCLA scores at three year follow-up (24.6 vs 14.9) (Ciampi et al. 2014). However, there is a concern that over time, re-tears are associated with worse pain, decreased function, and progression of arthritis (Jeong et al. 2022).
Our cohort noted improvements in motion in those treated with scaffolds relative to those treated without at one year, which resolved by two. This could potentially be due to an earlier reorganization of fibers at the tendon-bone interface. Ciampi et al’s patients treated with patch augmentation reported significantly improved forward flexion (174.7 degrees versus 140.7) than those without at three years (Ciampi et al. 2014). Consigliere et al noted improvements in forward flexion and external rotation after treatment with patch augmentation as well as minimal improvements in external rotation (8 degrees), although there was no control group to compare to (Consigliere et al. 2021). Studies addressing strength after rotator cuff repair with patch augmentation is scarce, however one group noted improvements in abduction strength with the use of a polyethylene patch, whereas our patients noted a relatively greater internal rotation strength post-operatively (Ciampi et al. 2014).
The randomization protocol limited selection bias of the patients. Patients remained blinded throughout, limiting reporting bias in the patient reported outcomes. Another unique aspect of this study is the imaging at two time points allowing for the differentiation between early and late failures. While Ianotti et al found that the majority of retears occurred within the first six months postoperatively after a rotator cuff repair, in this study 38% (5/13) of patients in the control group who did not have a tear at the first MRI demonstrated late progression of their tears (Iannotti et al. 2013). This supports continued late assessment of tear progression in studies evaluating the benefits of scaffold use.
There are, however, several limitations to this study. The investigators assessing patient strength and motion were not blinded to the treatment group; this was partially mitigated by the use of a dynamometer and electronic goniometer to decrease the subjectivity of the measurements. This multicenter study is powered, but the data presented represents a single practitioner’s contribution to the database, thus a larger sample of patients may have revealed different outcomes regarding overall health and patient function. Furthermore, both ultrasound and MRI were used to assess late term healing. The primary investigator has used in-office ultrasound for over a decade, but MRI is still considered the gold standard healing integrity and interobserver variability could be greater with ultrasound interpretation of Sugaya classification. Finally, a longer-term follow-up in this study may also have demonstrated further failures over time in both groups. However as rotator cuff repair failures tend to occur within the first year postoperatively, we feel that two year data captures the majority of the potential differences between the groups, particularly since the scaffold has resorbed by six months (Chona et al. 2017).
In conclusion, patients with an interpositional nanofiber scaffold placed at the time of rotator cuff repair demonstrated a significantly lower radiographic failure rate than patients undergoing rotator cuff repair alone within the first two years. Despite radiographic failures, there were no differences in patient reported outcomes and clinical examination findings at two years between both groups.
Source of Funding
Post-operative MRI’s and implanted scaffolds were paid for by Atreon.