


Introduction
Clavicular fractures are a common injury, accounting for 2.6% of all fractures, and are usually found in young males (McKee 2010). While non-operative treatment may be an option for some clavicle fractures, it has been shown that surgical intervention is more beneficial for displaced midshaft clavicle fractures. Surgical correction in these cases demonstrated decreased rates of nonunion (Martin et al. 2021). The use of bone graft is often employed to help increase union rates in cases of nonunion or revisions (Sidler-Maier et al. 2017).
The traditionally used standard for autologous bone graft has been the iliac crest (Wolfe and Kawamoto 1978). This is proven to be effective, but there are risks ranging from infection, superficial seroma, superficial hematoma to abdominal herniation through the donor site defect, vascular injury, and iliac wing fracture (Arrington et al. 1996). These complications have the potential to lead to increased donor site morbidity.
We propose that the distal clavicle can be used as autograft into the midshaft clavicle for treatment of nonunions and revisions.
The distal clavicle is excised commonly to treat conditions such as acromioclavicular (AC) impingement in a procedure originally described by Mumford. This procedure has low associated complications with a high rate of patient satisfaction (Snyder, Banas, and Karzel 1995). Tokish et al. described distal clavicle autograft as an option for glenoid bone defects with no complications from neither the distal clavicle excision nor the autograft placement (Taylor et al. 2020). This graft may eliminate the additional complications that often occur with iliac crest harvest.

Case Presentation
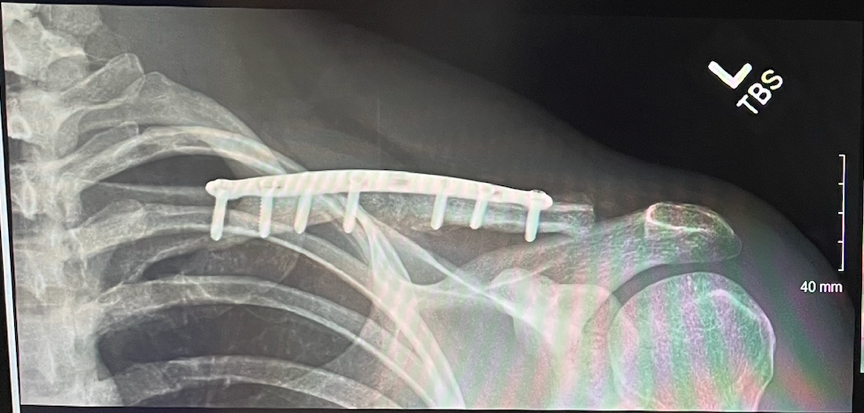
The patient was a 22-year-old male who originally fell and injured his left clavicle while running. X-rays revealed a midshaft displaced comminuted fracture with three centimeters of shortening and greater than 200% displacement. The patient was treated with operative reduction and internal fixation (ORIF). This fracture healed well with minimal pain and no complications.
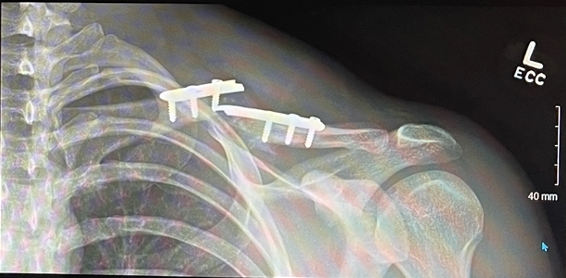
Six months post-op from the first injury, the patient returned to clinic with pain after working out at a gym. He noticed deformity along the left clavicle as well as swelling. Repeat X-rays were obtained in the office, shown below (Figure 1).

Preoperative plan
Repeat X-rays at the six-month office visit revealed interval displacement of previously noted midshaft clavicle fracture with hardware failure and displacement with shortening of approximately one centimeter at the fracture site. Treatment options were discussed thoroughly with the patient, and the recommendations were made for revision surgery for nonunion clavicle fracture with hardware failure.
Operative results
The patient was positioned in beach-chair positioner and was prepped and draped accordingly. Standard anterior approach was used, and the prior skin incision was extended to approximately eight centimeters in length along the previous well-healed incision. Dissection was carefully performed, and cultures were drawn for precaution even with no evidence of infection, which then resulted in negative cultures.
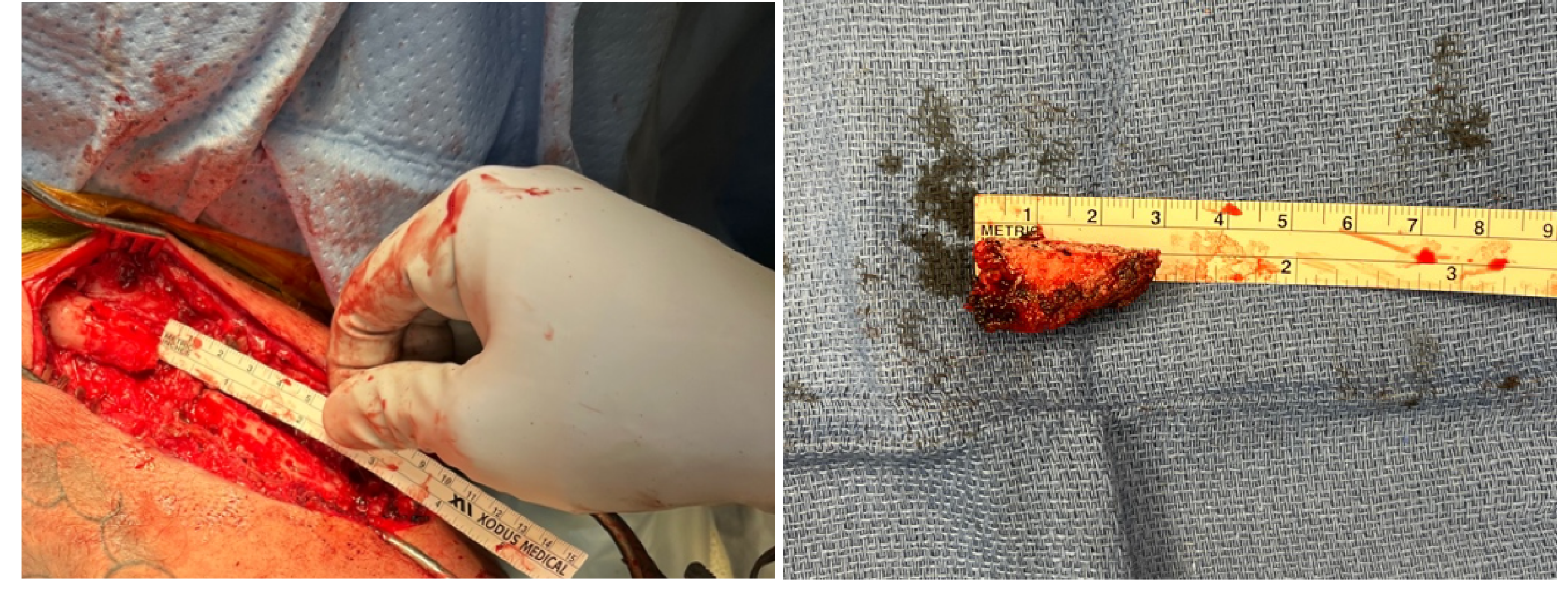
Previous hardware was removed without difficulty. The remaining bone was good quality, although there was a segment of bone void comprised of fibrous scar tissue with minimal callus formation (Figure 2). Fracture was reduced, and an Acumed (Hillsboro, OR) pre-contoured clavicle plate was placed spanning the fracture site. Wound was then irrigated with Irrisept (Irrimax Corporation, Lawrenceville, GA) and normal saline.
Due to the bone defect, it was decided to utilize autologous bone graft from the patient’s ipsilateral distal clavicle as previously described by Tokish et al (Taylor et al. 2020). Incision was extended further to the AC joint. The distal clavicle was measured and harvested with a size of approximately 3 cm in anterior to posterior (depth) and approximately 1.5 cm in medial to lateral (width) to ensure no violation of the trapezoidal branch of the coracoclavicular ligament, which is on average located 2.1 cm from distal clavicle (Figure 2).
To further augment the repair, bone marrow aspirate from the ipsilateral proximal humerus was obtained using percutaneous technique

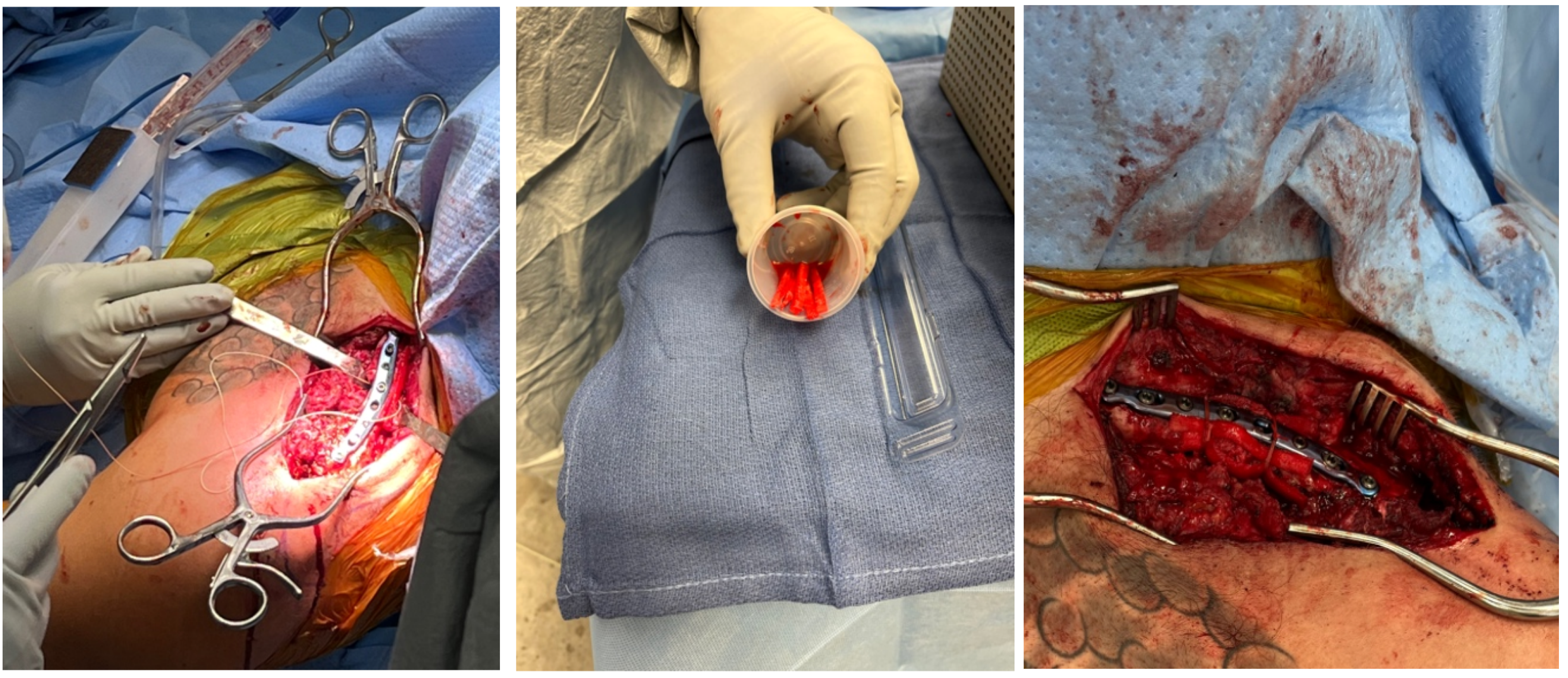
At this time, the plate was positioned and screwed into place (Figure 3 Left). Since this procedure was a revision, further augmentation was achieved utilizing BioBrace collagen strips which were cut and used to recreate the periosteal sleeve (Figure 3 Center). These were secured with #1 Vicryl sutures in a cerclage racking hitch fashion. Any remaining harvested bone fragments were mixed with vancomycin topical powder and placed along the fracture site (Figure 3 Right). Fixation was completed with 8-hole superior locking plate with a combination of locking and nonlocking screws. Films with fluoroscopy were obtained through range of motion to ensure stable fixation and no iatrogenic instability of the AC joint.

The wound was thoroughly irrigated and vancomycin topical powder placed. The wound was closed with Vicryl followed by subcuticular Monocryl. Dressing was placed and patient was placed in a sling and made non-weight bearing for approximately 4 weeks with pendulum exercises only.

Postoperative Results
Patient was seen for follow up at three weeks and nine weeks. At three weeks, incision was well-healed with X-ray demonstrating stable fixation. At nine weeks, patient displayed full range of motion. Repeat X-rays showed signs of healing and callus formation. There was no iatrogenic instability of the AC joint (Figure 4). Patient was released to full activities with no restrictions. Discussion with the patient at six months continued to show no complications or pain. At this time, patient declined follow-up imaging due to lack of pain and was back to work. The patient will continue to be monitored.


Discussion
Bone grafting dates back to the 1600s with a xenograft placed into a soldier’s skull (De Boer 1988). Today, there are many methods of bone grafting, each with their own risks and benefits. Autograft has long been the standard for bone grafting techniques. This is advantageous as they contain osteoinductive and osteoconductive properties with negligible infection risk (Campana et al. 2014). Challenges of autografts may include additional donor sites wounds, post-operative pain, and variable bone quantity (Arrington et al. 1996; Campana et al. 2014). Alternative options are allograft and xenograft, but these are limited in use due to cost, processing variability, and decreased osteoinductive properties (Campana et al. 2014).
Depending on desired application from bone graft, options can include cancellous or cortical bone. Cancellous bone is commonly used as a bone graft, as it contains highly osteogenic properties. Cancellous bone is very osteoconductive, osteoinductive, osteogenic, and mildly structurally supportive (Roberts and Rosenbaum 2012). Common sites of cancellous bone used for graft include the iliac crest, posterior superior iliac spine, distal femur, proximal or distal tibia, distal radius, and olecranon (Schmidt 2021). Cortical autografts are comparatively less osteoconductive, osteoinductive, and osteogenic than cancellous bone, but are advantageous for their structural support (Roberts and Rosenbaum 2012). Some examples of sites used for cortical bone graft donation include the fibula and iliac crest (Mahsut Dinçel 2018). In the case presented, the distal clavicle was used as the autograft. Clavicle structure analysis was performed on cadaver bone and showed that it was comprised predominately of cancellous bone (Shah and Routatal 2015). This would then provide the osteogenic properties that support successful bone graft. One example showing the success of distal clavicle autograft is a study in which the graft had been used to reconstruct bone related to glenoid loss (Larouche et al. 2020).
BioBrace is FDA approved for soft tissue reinforcement. BioBrace is described as a highly porous type I collagen matrix and it is reinforced with bioresorbable PLLA microfilaments. This material maintains strength over the course of approximately two years before reabsorbing. The implant has unique characteristics of being able to create supplemental strength through load sharing.
The intent for this patient was to use BioBrace to recreate the periosteal function and serve as a membrane barrier, as this is often disrupted during repeated trauma and prior surgery. Recreating the periosteum is beneficial for new bone callus formation. It was also felt that the distinctive BioBrace soft tissue structure could help retain bone graft material similar to the previously utilized Masquelet technique, without requiring a second procedure.
The Masquelet technique is a two-staged technique designed to reconstruct segmental bone defects. The initial stage is hallmarked by using a cement spacer to induce formation of a pseudosynovial membrane. The second stage then requires removal of the temporary cement spacer and application of bone graft, using the formed membrane to aid in vascularity and corticalisation (Masquelet and Begue 2010). The formed membrane is similar to the original periosteum in location and structure (Alford et al. 2021). In the case presented, the BioBrace is intended to serve as the membrane-like material, effectively mimicking the periosteum, and can be implanted concurrently with the bone graft, therefore eliminating the need for a second procedure.
In addition to the augmentation with the BioBrace collagen, autologous bone marrow aspirate was also applied to the fracture site to improve bone formation. Bone marrow aspirate contains mesenchymal stem cells which are capable of promoting bone formation (Schottel and Warner 2017). In the case presented, the bone marrow aspirate was harvested from the proximal humerus due to proximity to the surgical site and single site surgical preparation. This approach eliminated the need for a secondary wound related to the harvest site and minimized patient morbidity. The proximal humerus and the ileum have both been shown in studies to be reliable sources of active bone marrow (by number of colony-forming units) for augmentation use (Otto et al. 2020). Specific to the healing of clavicle nonunion fractures, a retrospective study found that not only is bone marrow aspirate safe with minimal complications or pain, but it does increase the rate of fracture union (Benshabat et al. 2021).
Summary
We present a novel case of utilizing distal clavicle autograft for nonunion midshaft clavicle repair. Based on the current literature, bone graft was a reasonable treatment option for the patient presented. The choice to use the distal clavicle is supported based on the osteogenic properties provided by this type of bone. Distal clavicle has been successful as an autograft as described by Tokish et al (Taylor et al. 2020). Use of the distal clavicle for clavicle midshaft nonunion has not been reported. Distal clavicle excision has been a mainstay of surgical treatment in the past, as described by Mumford, with minimal complications reported. Augmentation with the BioBrace was used to recreate the membrane formation characteristic of the two-stage Masquelet technique. Additional augmentation by autologous bone marrow aspirate is supported in literature with improving of bone formation, and with minimal morbidity and low cost. This case introduces a novel use of distal clavicle autograft and augmentation with BioBrace collagen in a revision clavicle repair for nonunion.
Limitations
While the case presented was successful with positive patient outcome, it is unknown if distal clavicle autograft would be sufficient for repair without the augmentation techniques. There are multiple confounding factors including distal clavicle autograft, bone marrow aspirate, BioBrace, and a broken plate. Further studies will need to be completed to see the specific benefit of each technique.

Conclusion
This case demonstrates a novel method of using distal clavicle autograft for mid-clavicle nonunion fracture in a revision setting, and augmentation utilizing bone marrow aspirate from the ipsilateral proximal humerus and the BioBrace collagen strips for recreating the periosteum. This case also demonstrates an alternative option for bone autograft in the setting of surgical treatment of clavicle nonunion with minimal morbidity and complications.