

Introduction
The use of surgical tourniquets in orthopaedic surgery has been well described (Alcelik et al. 2012; Fan et al. 2014; Wang et al. 2016). Benefits of tourniquet use include decreased intraoperative blood loss as well as improved visualization of the operative field. For these reasons, it has become common practice to place a tourniquet about the thigh for orthopaedic procedures involving the knee (Alcelik et al. 2012).
Although rare, accounting for only 0.05-1.0% of all complications in total knee arthroplasty and knee arthroscopy, arterial injury is a known and potentially devastating complication, with the possibility of significant morbidity and mortality (DeLee 1985; Small 1986; Sundaram et al. 2020). Several authors have attempted to define positions of the knee that displace the popliteal artery furthest from the posterior tibial cortex (PTC), offering a lower risk of arterial injury during surgery. Matava et al. defined the distance of the popliteal artery from the posterior cruciate ligament (PCL) tibial insertion, showing that with increasing knee flexion angles, the risk of arterial injury during PCL reconstruction was reduced by displacing the popliteal artery further from the PCL tibial insertion (Matava, Sethi, and Totty 2000). However, no study to date has evaluated the effects of a thigh surgical tourniquet on the spatial anatomy of the popliteal neurovascular structures, most notably the popliteal artery, as it relates to the bony and ligamentous anatomy of the knee.
The purpose of this study is to evaluate whether an inflated thigh surgical tourniquet alters the distance that the popliteal artery rests from both the PCL tibial insertion and the PTC directly anterior to the artery. The authors hypothesize that inflating a thigh tourniquet would tether the arterial system proximally, thus translating the popliteal artery closer to the posterior tibia.
Methods
Institutional Review Board approval was obtained for human subjects research. 6 knees were evaluated in 4 different subjects between July of 2017 and April of 2018. All subjects were male volunteers over 18 years old, with an average age of 29 years. None of the subjects had previous surgical procedures on the knee being evaluated, skeletal deformities, previous or known ligamentous injury, joint contractures, history of deep venous thrombosis or peripheral vascular disease, magnetic resonance imaging (MRI)-incompatible implants, and pregnancy. Using 3 Tesla MRI, 2-dimensional proton density weighted axial images at the level of the PCL tibial insertion were obtained in both full extension and 90 degrees (°) of flexion, with and without a thigh tourniquet inflated to 200 millimeters of mercury. Tourniquet inflation was limited to 200 millimeters of mercury for subject comfort. The level of the tibial PCL insertion was then confirmed using localizer images.
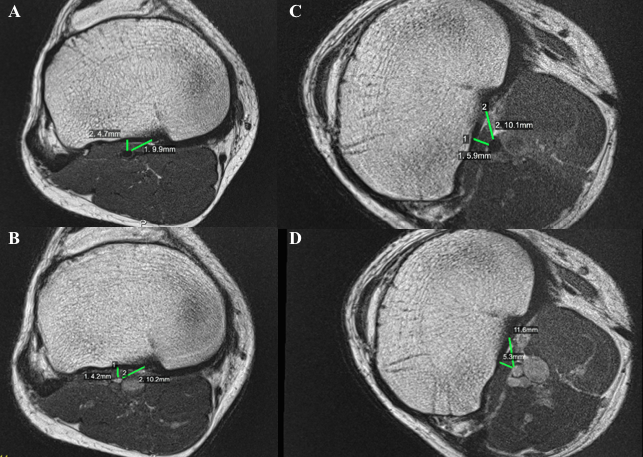
Extension was evaluated first (Figure 1A). A tourniquet was placed on the thigh of each subject, and the knee was first imaged with the tourniquet deflated. Localizing imaging as well as 2-dimensional proton density weighted images were obtained. This series took an average of 5 minutes. Each subject then inflated the tourniquet to 200 millimeters of mercury, and the knee was re-imaged (Figure 1B). Subjects were instructed to hold the extremity still as the same prior localizers were used for subsequent imaging with the tourniquet inflated. This series took an average of 3 minutes.

The exam was then repeated at 90° of flexion (Figures 1C and 1D). In order to allow for proper fitting of subjects into the MRI tube with the knee flexed to 90°, each subject assumed a lateral decubitus position corresponding to which ever knee was being studied; for example, if the left knee was being studied, the patient assumed a left lateral decubitus position.
The distance to the popliteal artery was then measured from both the PCL tibial insertion and the PTC directly anterior to the anterior margin of the popliteal artery at the level of the PCL tibial insertion. Measurements were performed on axial rather than sagittal views to obviate the necessity of accounting for obliquity. Any images affected by subject movement were discarded and re-performed. Of note, no pre-inflation exsanguination was conducted.
Changes in popliteal artery position following application of the tourniquet were assessed using Related-Samples Wilcoxon Signed Rank tests at each angle of flexion. Analyses were carried out using SPSS Version 22 (International Business Machines Corporation, Yorktown, New York) and significance was determined for values of p<0.05. The effect size was subsequently calculated with Cohen’s d.
Results
The popliteal artery could be traced proximally from the posterior distal femur to the level of the PCL tibial insertion in all MRIs. The popliteal artery was found posterior and slightly lateral to the PCL tibial insertion in all knees.
Descriptive statistics are shown in Table 1 with statistical comparisons between the relative position of the popliteal artery in flexion and extension both with and without the tourniquet. Initial measurements were obtained without the tourniquet inflated. In full extension, the mean distance between the PCL tibial insertion and the popliteal artery was 9.82 (±1.36) millimeters (mm), and the mean distance between the PTC and the popliteal artery was 6.88 (±1.49) mm. In 90° of flexion, the mean distance between the PCL tibial insertion and the popliteal artery was 10.45 (±3.14) mm, and the mean distance between the PTC and the popliteal artery was 9.43 (±3.43) mm. There was a statistically significant increase in the distance from the PTC to the popliteal artery when going from full extension to 90° flexion, both with and without tourniquet use (p=0.046 for both groups).
Subsequent measurements were obtained with the thigh tourniquet inflated to 200 millimeters of mercury. In full extension, the mean distance between the PCL tibial insertion and the popliteal artery was 10.23 mm, and the mean distance between the PTC and the popliteal artery was 6.17 (±1.13) mm. In 90° of flexion, the mean distance between the PCL tibial insertion and the popliteal artery was 10.38 (±2.44) mm, and the mean distance between the PTC and the popliteal artery was 7.95 (±1.96) mm.
Statistical analysis of the effect of the tourniquet on relative popliteal artery position is shown in Table 2, accompanied by the calculated effect sizes for each condition. When comparing the distance between the PTC and the popliteal artery in both flexion and extension, there was a statistically significant decrease in the distance when a tourniquet was used, compared to when it was not (p=0.028 and p=0.046, respectively). As noted in Table 2, the effect size for this decrease was moderate in both flexion and extension (d=0.53 and d=0.54, respectively).
Discussion
This study is the first of its kind to evaluate the in vivo effects of an inflated thigh surgical tourniquet on the spatial anatomy of the popliteal artery using MRI. Our results suggests that while using an inflated thigh tourniquet, the popliteal artery rests slightly closer to the PTC in both flexion and extension versus if no tourniquet were utilized. Our study also suggests that flexion of the knee displaces the popliteal artery further from the PTC, confirming previous findings, and demonstrates that this effect is limited by an inflated tourniquet (Matava, Sethi, and Totty 2000; Ahn et al. 2007; Shetty et al. 2003). Furthermore, these findings have a moderate effect size, indicating that the approximation of the popliteal artery and the PTC may be large enough to have a clinical impact above and beyond the implications of a statistically significant difference.
There has been extensive prior investigation to define the safest intraoperative position of the knee during open and arthroscopic surgery to minimize the risk of vascular injury. Both cadaveric and human studies utilizing ultrasonography, MRI, and angiography have been conducted. Shetty et al. demonstrated a statistically significant increase in popliteal artery distance from the PTC with increasing knee flexion from 0° to 90° via duplex ultrasonography in the majority of human knees tested (Shetty et al. 2003). In a cadaveric study by Matava et al., increasing knee flexion caused the popliteal artery to rest further away from the PTC (Matava, Sethi, and Totty 2000). Ahn et al. performed a cadaveric angiographic study in which they measured the relationship and distances between the popliteal artery and the posterior cruciate ligament (Ahn et al. 2007). The authors found that the distance between the popliteal artery and the PCL at the joint level increased after flexion of the knee joint (Ahn et al. 2007). We found similar results to prior studies regarding the distance between the popliteal artery and the posterior aspect of the proximal tibia. Cosgarea et al. found a mean sagittal distance of 9.7 mm between the PCL tibial fovea and the popliteal artery with knees in 90° flexion in 9 specimens (Cosgarea et al. 2010). Without tourniquet use, our results show a mean of 10.23 mm between the popliteal artery and PCL tibial fovea in 90° flexion, consistent with prior results. Keser et al. showed that in the majority of knees evaluated with MRI, the popliteal artery sat lateral to the central axis at the joint line (Keser et al. 2006). Similar findings were seen in our study.
There are several limitations to this study. The study carries a small sample size, all of whom are young adult males. This study was not powered to evaluate other factors that may contribute to popliteal artery displacement, such as height, body habitus, and exact placement of thigh tourniquet. Furthermore, in order to evaluate knee flexion, subjects had to lay in the lateral decubitus position to allow proper fitting in the MRI tube, theoretically eliminating a gravity-driven posterior displacement of the popliteal artery. The tourniquet inflation was limited to 200 millimeters of mercury. While this was necessary for subject comfort, tourniquets are often inflated higher when used intraoperatively, we believe that this may further decrease the distance between the popliteal artery and the PTC. Finally, we were unable to exsanguinate the limbs prior to evaluation, as this would have required subjects to undergo localizing imaging with the tourniquet inflated, adding more time than the three minutes required for each series.
Conclusions
The primary objective of this study was to redefine the previously described spatial anatomy of the popliteal artery to account for the effects of an inflated thigh surgical tourniquet. Based on our findings, inflating a thigh tourniquet results in the popliteal artery resting approximately 1 mm closer to the posterior aspect of the tibia (p=0.028), and it does not change the distance between the popliteal artery and the PCL with any statistical significance. Further investigation is required to assess the clinical significance of this effect on the risk of vascular injury in the context of knee surgery.