


Introduction
Since the introduction and widespread use of electronic health records (EHR), many physicians have spent less time face-to-face with their patients and more time working on a computer. Some studies suggest that U.S. physicians now spend as much time on the computer as they do with patients (Sinsky et al. 2016; Tai-Seale et al. 2017). While the EHR has improved numerous aspects of patient care, many in the medical community are concerned about the association it may have with physician burnout (Melnick et al. 2020; Tajirian et al. 2020). A prior study has demonstrated that physicians who use EHRs have lower satisfaction with the amount of time they spend on clerical tasks and have higher rates of burnout (Shanafelt et al. 2016). Specifically, time spent after hours on EHR and volume of inbox messages were shown to be related to exhaustion and thus higher burnout among primary care physicians (Adler-Milstein et al. 2020). Burnout is a syndrome defined by the principal components of emotional exhaustion, depersonalization, and diminished feelings of personal accomplishment caused by work-related factors (Chopra, Sotile, and Sotile 2004; Maslach, Schaufeli, and Leiter 2001; Rotenstein et al. 2018). Burnout is most likely to occur in jobs requiring extensive care of others, which is likely a major contributing factor as to why physicians have much higher rates compared to other professions (Maslach, Schaufeli, and Leiter 2001). Physician burnout is a serious issue in the United States, with a reported prevalence of 40 to 50% in some studies (Rotenstein et al. 2018). It is associated with an increased risk of major medical errors in addition to lower quality of care, higher costs, and decreased physician satisfaction (Tawfik et al. 2018).
Given the demands of many surgical specialties, there is no surprise that burnout can be especially prevalent in this subset of physicians (Dimou, Eckelbarger, and Riall 2016). Orthopaedic surgeons have remarkably high rates of burnout, ranking in the top 5 for specialties with the most burnout in the U.S (Shanafelt et al. 2016). Sargent et al. showed that despite high levels of job satisfaction, orthopaedic residents and faculty are still amongst those with the greatest rates of burnout. They identified risk factors as well as protective factors against burnout for orthopaedic residents and faculty. Many of the protective factors focused on self-care, including dedicating time for exercise, hobbies, vacations, and spouses as well as having mentors in which to confide (Sargent et al. 2009). Additionally, Arora et al. found that subjective factors such as the perception of an unrewarding career or perceived lack of autonomy showed a stronger correlation to level of burnout than objective factors of caseload, practice setting, or proportion of patients insured (Arora, Diwan, and Harris 2013). While multiple studies have discussed physician burnout and its effect on orthopaedic residents and faculty, the authors are not aware of a study that has focused specifically on the potential detrimental effects of EHR use in orthopaedic surgery.
The aim of this study was to determine the amount of time spent on EHR compared to actual patient interaction in four busy orthopaedic outpatient clinics and its perceived effect on each surgeon. Given the extensive reliance on EHR, we hypothesized that the surgeons spend at least as much time on the EHR as they do interacting with patients on a clinic day.

Methods
Four busy orthopaedic surgeons at one tertiary academic institution were each followed on clinic days to determine the amount of time spent on Epic Hyperspace EHR as compared to face-to-face with patients. Each surgeon’s clinic day included time spent dictating notes, ordering advanced imaging, scheduling surgeries, responding to EHR inbox messages, and navigating the Epic EHR physician user interface. Surgeon 1 is a senior faculty member nine years in practice and works with a resident, fellow, nurse, and two medical assistants in clinic. Surgeon 2 is a junior faculty member one and a half years in practice at the institution and works solely with a medical assistant. Surgeon 3 is a senior faculty member seven and a half years in practice at the institution and works with a resident, fellow, PA, and medical assistant in clinic. Surgeon 4 is a junior faculty member twelve years in practice at the institution and works with a nurse and two medical assistants.
A research assistant recorded how much time the surgeon spent dictating notes, writing orders, or replying to clinical inbox messages (EHR time) and how much time was spent on loading screens or EHR buffering (loading time) during which no actions could be completed. Two separate stopwatches recorded these times, which was deemed more accurate than Epic-recorded data since the EHR was left open between patient interactions. EHR time and loading time were calculated as a percentage of the surgeon’s time spent in clinic. If time was spent on the EHR after clinic hours, such as for note addendums or responding to patient calls, this additional time was reported as percentage of the surgeon’s total time. The present study is in compliance with ethical standards and did not require IRB approval.

Results
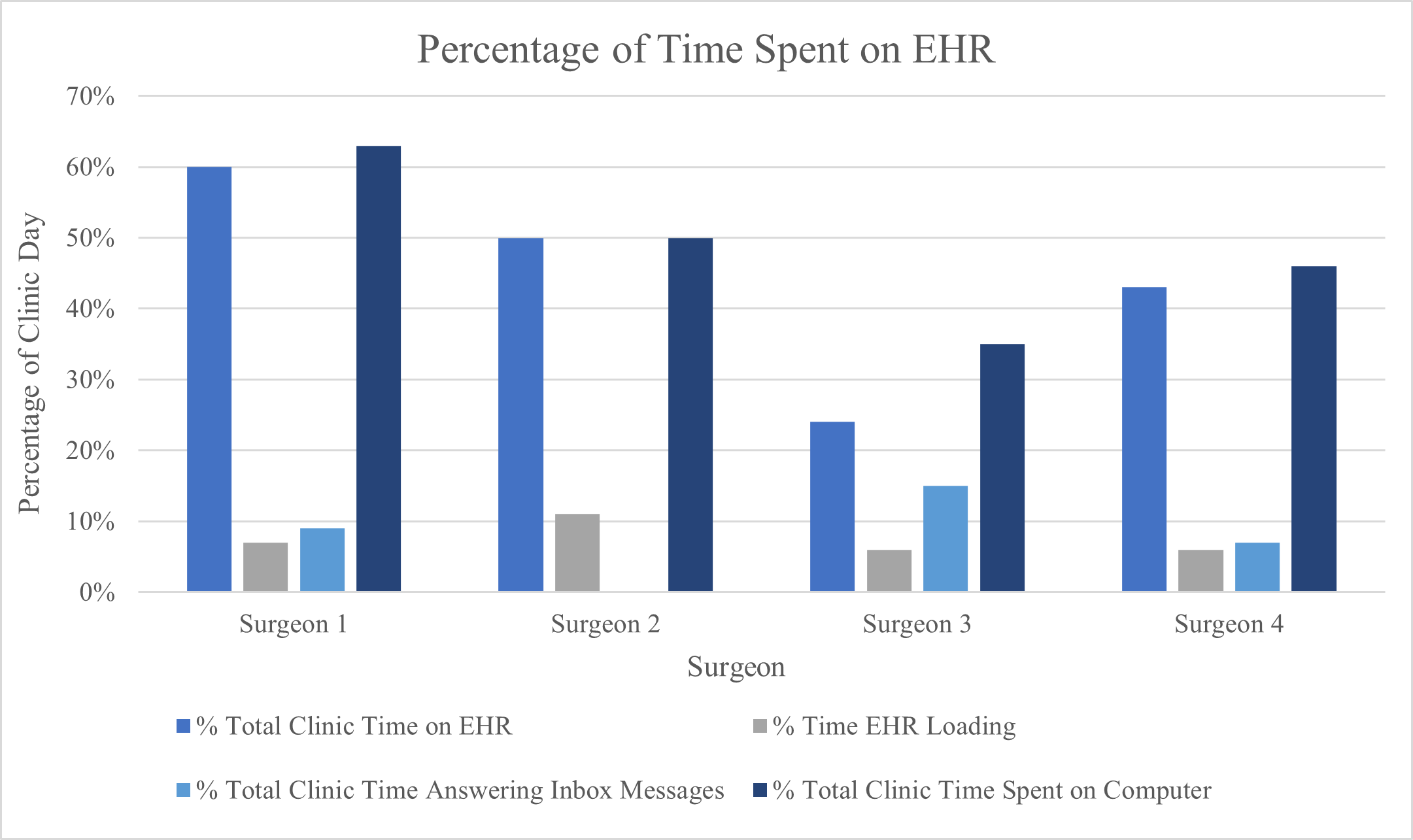
Surgeon 1 saw 60-65 patients from 7:30am to 3pm on each clinic day. On the first day Surgeon 1 spent 4 hours and 46 minutes using the EHR, 23 minutes of which was loading time. This accounted for 64% of his time in clinic. He spent 1 hour after clinic responding to inbox messages (12% of total time). In total, 68% of the surgeon’s day was spent on the computer. On another day, Surgeon 1 spent 4 hours and 10 minutes using the EHR, 15 minutes of which was loading time. This comprised 56% of total clinic time. A total of 30 minutes was spent after hours responding to inbox messages (6% of total time), totaling 58% of the day spent on the computer. Averaging the two days, Surgeon 1 spent 63% of his time on the computer.
Surgeon 2 saw 25-30 patients from 8am to 3:15pm on each clinic day. On the first day Surgeon 2 spent 3 hours and 33 minutes using the EHR, 16 minutes of which was loading time. This accounted for 49% of clinic time. On another day Surgeon 2 spent 3 hours and 42 minutes using the EHR, 32 minutes of which was loading time. This accounted for 51% of total clinical time. Surgeon 2 responded to all his inbox messages during clinic time. Averaging the two days, Surgeon 2 spent 50% of his days on the computer.
Surgeon 3 saw 25 patients from 8:00am to 4:15pm on clinic day one and 42 patients from 7:30am to 4:15pm on day two. On the first day Surgeon 3 spent 2 hours and 16 minutes using the EHR, 6 minutes of which was loading time. This comprised 28% of total clinic time. A total of 93 minutes was spent after hours responding to inbox messages (16% of total time), totaling 39% of the day spent on the computer. On day two Surgeon 3 spent 1 hour and 40 minutes using the EHR, 8 minutes of which was loading time. This accounted for 19% of total clinic time. A total of 87 minutes was spent responding to inbox messages (14% of total time), totaling 31% of the day spent of the computer. Averaging the two days, Surgeon 3 spent 35% of his days on the computer.
Surgeon 4 saw 18 patients from 7:30am to 12:30pm on clinic day one and 25 patients from 7:45am to 1:45pm on day two. On the first day Surgeon 4 spent 1 hour and 51 minutes using the EHR, 8 minutes of which was loading time. This comprised 37% of total clinic time. A total of 25 minutes was spent after hours responding to inbox messages (8% of total time), totaling 42% of the day spent on the computer. On day two Surgeon 4 spent 2 hours and 53 minutes using the EHR, 9 minutes of which was loading time. This accounted for 48% of total clinic time. A total of 20 minutes was spent after hours responding to inbox messages (5% of total time), totaling 51% of the day spent on the computer. Averaging the two days, Surgeon 4 spent 46% of his days on the computer.

Discussion
While orthopaedic surgeons are known to have high reported rates of burnout, limited studies have focused on EHR usage amongst residents and faculty in this specialty (Sargent et al. 2009; Arora, Diwan, and Harris 2013; Barrack et al. 2006). The current study found that approximately half of each surgeon’s time was spent entering information into the EHR or waiting for it to load during a typical day in clinic. When accounting for time spent after hours responding to inbox messages, time on a computer surpassed actual face-to-face patient interaction for one of the surgeons. While the most recent American Medical Association CPT® Evaluation and Management Guidelines allow use of total encounter time for coding purposes, the lack of face-to-face interaction in today’s age of technology likely contributes to the increasing rates of burnout amongst physicians (“CPT® Evaluation and Management | American Medical Association,” n.d.). A study with primary care physicians found that time spent after clinic hours on the EHR correlated with higher rates of burnout (Adler-Milstein et al. 2020). Given the amount of time utilized on inbox management after hours in orthopaedic surgery clinics, this may be an important factor related to high rates of orthopaedic surgeon burnout as well. Surgeon 2 was able to complete this task during clinic, but still spent about half his time on the computer despite seeing less than half of the patients in a given day. This is because the other surgeons have trainees and ancillary staff who help with taking histories, writing orders and notes, and scheduling surgery while Surgeon 2 must take care of all these tasks on his own. This demonstrates the reliance and requirement of EHR usage at multiple levels of training. For all four surgeons, the time spent on the EHR for documentation and responding to inbox messages was alarmingly high. Similar results are seen in other specialties. Arndt et al. found that primary care physicians spend over half their time on the EHR and performing after hours clerical tasks (Arndt et al. 2017). With the higher rates of burnout in orthopaedic surgeons, the amount of time dedicated to computer tasks may be even more detrimental in contributing to burnout compared to other specialties. Many of the risk factors for burnout that Sargent et al. identified could be related to excessive EHR use. Almost all of the identified risk factors revolved around not having enough time – to sleep, to have a successful relationship, to enjoy home life, to exercise, to have hobbies (Sargent et al. 2011). Given the amount of time spent on loading screens and non-clinical care tasks during clinic hours, there is room for great improvement. Surgeons in particular must maximize efficient usage of clinic time due to limited clinic days and the need to prioritize patient face-time in the context of surgical indications. With less time spent on the EHR each day, specifically on clerical tasks, orthopaedic residents and faculty would have more time to themselves likely resulting in less burnout (Sargent et al. 2011).
With patient and physician well-being in mind, the amount of time spent in front of a computer is alarming. Despite the known negative effects of the EHR on physician burnout, there is no simple solution to solve this prevalent issue (Adler-Milstein et al. 2020; Downing, Bates, and Longhurst 2018). The simplest and likely most effective solution would be having more user-friendly EHRs with less documentation required for each physician. This would allow more patient interaction and less time spent recording information for reimbursement purposes. Given the amount of time spent on loading screens for each surgeon, one of the easier solutions would be to create a quicker interface that limits or eliminates loading time while the provider toggles between screens. This would include limiting pop-up windows and third-party applications for imaging or surgical scheduling, which caused the majority of downtime in the current study. Although likely more challenging, another solution is to decrease the time required for computer documentation. Unfortunately, documentation requirements continue to become more stringent and continue to add-on rather than take away responsibilities for the physician. Since only a few EHRs control the market and their main goal is to streamline billing and are not necessarily designed to improve physician efficiency, this is highly unlikely to change any time soon given the lack of financial incentives to the EHR companies. The medicolegal climate in the United States also necessitates more detailed documentation. Other potential solutions include the use of scribes or advanced care team models, where a clinically trained individual assists with documentation, nonphysician order entry, and inbox management amongst other tasks. Institutions should also consider effective standardized templates and dot phrases which capture the appropriate billing information but also minimize the time required for chart completion. In addition to the above changes, limitations on work hours and mindfulness training may also have a significant effect on reducing burnout in both residents and faculty (West, Dyrbye, and Shanafelt 2018). A 2021 systematic review reported multiple physician-suggested interventions to address EHR-related burnout and physician well-being (Nguyen et al. 2021). These recommendations spanned three central themes including policy interventions, organizational policy, and information technology which collectively focused on reducing the burden caused by documentation requirements and improving overall usability and productivity. Specific interventions suggested by physicians included (1) provide EHR training and ample time for this training as well as offer on-site EHR support services for physicians, (2) limit displaying irrelevant information on screen, (3) offer capabilities to automatically populate visit notes with select content from prior visits, among many others (Nguyen et al. 2021). It is important to note that the physicians’ recommendations described in this study applied to all eight dimensions of the sociotechnical model for health information technology, a model established by Sittig and Singh that has been successfully applied to evaluate health information technology interventions, thus highlighting the diverse array of factors that lead to workflow inefficiencies and EHR-related burnout (Sittig and Singh 2010). Ultimately, a multifactorial approach combining numerous solutions is likely the only way to make a significant dent in the widespread pandemic of physician burnout.
The current study has a number of strengths and weaknesses. This study successfully quantified the amount of time spent on the electronic health record for a typical clinic day of an orthopaedic surgeon. In addition, a breakdown of time spent on different tasks was given as a comparison to total clinic time. This study design allows for an accurate assessment of the time spent on EHR tasks compared to typically measured parameters. Lastly, all four surgeons are within the sports medicine division of the same tertiary institution and typically work with the same medical assistants. This limits potential confounding factors that could alter time spent on EHR by each surgeon, but also decreases the representativeness of this study for other health systems. In this study, we also investigated total time spent after hours responding to inbox messages. It should be noted that different physicians are likely to respond in a varying level of detail. While it is difficult to standardize the level of detail of these message responses between physicians, we believe that this data is useful to consider as a percentage of the surgeon’s overall time spent in clinic. Furthermore, future research that collects additional data points across multiple surgeons, institutions, and practice settings would increase the generalizability of the data. To limit bias the current study included two senior faculty and two junior faculty and followed them over multiple days. Additionally, this study did not investigate how visit type may have influenced time spent on the EHR or how other subspecialties utilized the EHR. While variations in clinic flow and number of patients exist between subspecialties, we believe similar findings would be found in any orthopaedic subspecialty. However, the primary aim of this study was to determine the amount of time spent on EHR compared to actual patient interaction, so including this type of analysis is likely more appropriate for future research investigating differences in EHR usage among orthopaedic surgeons across subspecialties and practice settings. Another limitation resides in the manual recording of data, which may result in systematic error due to use of stop watches. However, this is unlikely to affect the overall findings in any way. Finally, only one EHR platform was studied, and other health systems may have more efficient platforms.

Conclusion
Physician burnout is widespread in the field of orthopaedic surgery. Excessive usage of the electronic health record may be contributing, with some surgeons routinely spending over half of their clinic time using the EHR. While numerous approaches to improve the current system have been proposed, there is not a clear answer to the problem. The solution likely involves a multifactorial approach, including inherent changes to EHRs, widespread use of scribes or advanced care teams, work hour limitations to reduce the overall exposure to EHR-related factors leading to physician burnout, and mindfulness training to residents and faculty.

Ethical Approval
Not applicable. No ethical approval was required.
Competing interests
There were no relevant competing interests that impacted this study design, methodology, data acquisition or analysis.
Authors’ contributions
All authors were active participants, including contributing to the conception and design of the study, acquisition of data, and analysis and interpretation of data. All authors had full access to all the data in the study, and take responsibility for the integrity of the data and the accuracy of the data analysis as well as the decision to submit the manuscript for publication. All authors contributed by drafting, revising, editing and approving the final manuscript for submission.
Availability of data and materials
Not applicable. No datasets were used.
Acknowledgements
None
Conflict of Interest
None
Funding/Sponsorship
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.