


Introduction
The use of the direct anterior approach (DAA) for primary and revision total hip arthroplasty (THA) has increased over recent years (Patel, Shah, and Erens 2019). DAA-THA has been associated with a lower risk of dislocation and revision due to instability, shorter hospital length of stay, and early postoperative function compared to posterior-based approaches (Singh et al. 2020; Bendich et al. 2021; Charney et al. 2020; Kurkis et al. 2021; Ponzio et al. 2018; Elstad et al. 2021). However, an increase in wound complications has been demonstrated following DAA-THA, likely due to increased exposure to anatomical bacterial reservoirs compared to the direct lateral (DL) and posterior approaches (PA) (Kurkis et al. 2021; Purcell et al. 2018; Shohat et al. 2021). Separately, obese patients are at greater risk of surgical site infection in all THA regardless of approach (Purcell et al. 2018, 2016). Furthermore, increased body mass index (BMI) has been associated with increased operative duration, wound dehiscence, dislocation, and all cause reoperation, all of which persisted after controlling for comorbid conditions (Purcell et al. 2018, 2016; Hartford, Graw, and Frosch 2020; Antoniadis et al. 2018; Watts et al. 2015; Russo et al. 2015; Jahng et al. 2016). As a result, increased wound complication rates following DAA-THA are of particular concern for obese patients, and in fact obese patients have been shown to have an increased risk of superficial wound infections following DAA-THA compared to PA-THA (Jahng et al. 2016). The DA incision often crosses the groin crease; a damp area that in obese patients may be mechanically irritated by a pannus, potentially predisposing these patients to superficial wound complications.
Various postoperative dressings have been implemented to decrease the risk of wound complications. Two of these include incisional negative pressure therapy (iNPT) and polyester mesh (PM) with a liquid adhesive dressing. While both have been associated with decreased infection and complications when compared to historical standards of care such as silver-impregnated hydrofiber dressing, to our knowledge no study has compared the rates of complications between the two in the setting of THA (Cooper et al. 2022; Ailaney et al. 2021; Cooper et al. 2018; Anderson et al. 2020). The purpose of this study was to retrospectively compare the rates of wound complications in DAA-THA with the use of incisional negative pressure therapy (Prevena, KCI) and polyester mesh with 2-octyl cyanoacrylate liquid adhesive (Prineo, Dermabond, Johnson and Johnson).

Methods
Study settings and population
Institutional Review Board approval was obtained prior to study initiation. This single-center, multi-surgeon retrospective cohort study reviewed consecutive patients undergoing DAA-THA with iNPT or PM dressings from January 2016 to April 2021. Patients were identified through an institutional database. Patients receiving dressings other than iNPT or PM, approaches other than DA, and patients who were lost to follow-up before 3 months post-operatively were excluded from our study population. Only patients achieving the full 3 months of follow-up and therefore documentation of presence or absence of complications for the full study period were included. Closure was standardized between surgeons. This was a layered closure including a facial closure of #2 barbed monofilament, a subcutaneous #0 barbed monofilament suture and lastly a subcuticular #3-0 barbed monofilament suture. Postoperative dressing was selected by the attending surgeon after closure based on their individual preferences, and patients were routinely screened by multiple providers for adhesive and medication allergies pre-operatively. All three surgeons utilized both dressings among their patients, and which surgeon performed the procedure was not associated with any of our outcome measures (p = 0.81 for overall wound complications).
The pre-operative cleaning protocol at the surgical site consisted of a chlorhexidine gluconate soap followed by two scrubs with prep-sticks containing 2% w/v chlorhexidine gluconate in 70% v/v isopropyl alcohol. This was done in the operating room. Per surgeon operative protocols, there was minimal variance in incision length between patients. Obese patients did typically have larger incisions by no more than 2 centimeters to facilitate visualization of the operative field. Patients were instructed to remove the dressings at home at one week post-operatively. While patients are routinely advised to pursue a healthy BMI pre-operatively and high BMI was considered a contributor to poor surgical candidacy, this study included a range of BMI from a minimum of 15 kg/m2 to a maximum of 45 kg/m2. Patients were instructed to stop all tobacco smoking by 6 weeks pre-operatively, which was confirmed with cotinine testing. Patients were classified as smokers in this study if they were active smokers at the time of their pre-operative visit prior to this timepoint.
Data collection
Usual patient demographic information was collected, which included age, gender, medical comorbidities, and pre-operative BMI. Dressing type and any superficial or deep wound complication within 90 days of surgery were recorded. Superficial wound complications included superficial infection, dehiscence, keloid formation, persistent or purulent drainage not found to be deep infection, seroma, and delayed wound closure. Deep wound complications included periprosthetic joint infection (PJI).

Analysis
Wound complication rates were reported as a percentage of all patients and compared using 2-sample proportion z-tests. Relative risk ratios with 95% confidence intervals were also calculated. Demographics were compared using student’s t-test with Welch’s correction and Chi-square tests, where appropriate. Comorbidities, BMI, and dressing type were included in logistic regression. A p-value of < 0.05 was considered statistically significant. Statistical analysis was performed with use of Excel (Microsoft Inc, Redwood, WA) and RStudio Version 1.3.1093 (RStudio, Boston, MA).
Demographic Characteristics
711 patients were included in the analysis (N=711). Overall, 311 patients were men (43.7%) and 400 were women (56.3%). Mean age was 63.5 years, mean ASA level was 2.3, and mean BMI was 27.6 kg/m2. Only 1.1% of patients had BMI over 40 kg/m2. There was no difference in sex or age between the iNPT and PM cohorts (p = 0.21, p = 0.99, respectively; Table 1). Patients treated with iNPT had significantly higher ASA scores than those treated with PM (2.45, 2.19, p < 0.001, respectively; Table 1). The iNPT group also had significantly higher BMI than the PM group (30.29, 26.45, p < 0.001, respectively; Table 1).
Medical comorbidities were also recorded for analysis. Overall, 66 patients (9.28%) had a diagnosis of diabetes mellitus (DM), 31 (4.36%) were pre-operative smokers, 25 (3.52%) had liver disease, 39 (5.49%) had chronic kidney disease (CKD), and 25 (3.52%) had anemia. Differences in comorbidities by dressing cohort are listed in Table 2.
A post hoc power analysis (α = 0.05, β = 0.2) using the overall rate of wound complications in either cohort indicated that the sample size required to detect the difference would be 472 patients and that with our current sample of 711 patients the calculated power is 89.4%.


RESULTS
Postoperative complications
Post-operative complications within three months after DA-THA included superficial infection, dehiscence, keloid formation, persistent or purulent drainage, seroma, hematoma, delayed wound closure, erythema, incision swelling, wound irritation, and periprosthetic joint infection (Table 3). Wound dehiscence was the most frequent complication, affecting 26 patients (3.66%) overall, 16 (7.51%) in the iNPT cohort and 10 (2.01%) in the PM cohort. Other frequent wound complications among both groups included persistent drainage, superficial infection, and irritation with superimposed erythema.
The rate of periprosthetic joint infection (PJI) was 0.42% overall, 0.94% in patients treated with iNPT and 0.20% in patients treated with PM (p = 0.45, Table 2). The overall reoperation rate was 1.69%. The reoperation was 3.29% with iNPT and 1.00% with PM (p = 0.065, Table 2).
Of note, several patients receiving initial postoperative PM dressings were switched to other dressings after presentation of wound complications. One patient with wound infection was switched to iNPT dressings after an incision and drainage procedure. One with dehiscence and swelling was given daily bacitracin dressing changes. Four patients with dehiscence and/or drainage were switched to Silvadene dressings. Patients were grouped by their initial postoperative dressing prior to their first presentation with complications (i.e. a patient initially given PM dressing which was then switched to iNPT after presentation with superficial wound infection is coded as a complication in the PM cohort).
Superficial Wound complications
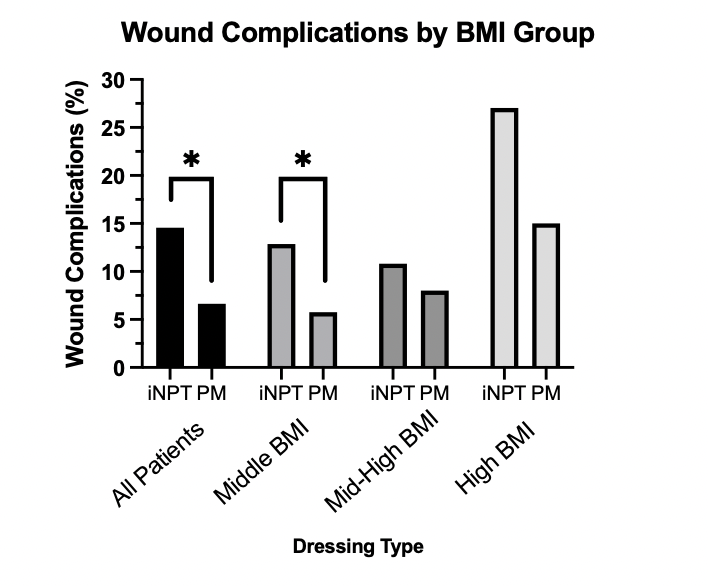
Overall, the rate of superficial wound complication among all patients was 9.00%. When stratified by BMI, the high BMI (> 35 kg/m2) cohort showed rates of wound complications of 18.84% overall, 27.03% for iNPT and 15.00% for PM. In the middle-high BMI (30 – 35 kg/m2) cohort, the rate of wound complications was 8.86% overall, 10.81% for iNPT, and 8.00% for PM. In the middle BMI (< 30 kg/m2) cohort, rate of wound complications was 7.16% overall, 12.87% for iNPT, and 5.75% for PM. In the setting of demographic differences in this retrospective cohort study between the iNPT and PM cohorts, logistic regression was performed to account for confounding effects of co-occurring risk factors.
Patient BMI, smoking, diabetes mellitus (DM), liver disease, chronic kidney disease (CKD), and anemia were included in the regression model alongside iNPT versus PM use. Adjusted odds ratios (aOR) are shown in Table 4. Controlling for the demographic factors listed above, PM dressing use was significantly associated with decreased odds of superficial wound complication, with an aOR of 0.555 compared to iNPT (p = 0.047). Secondarily, increased BMI and smoking were also significantly associated with increased wound complications (p < 0.05). For BMI, the model showed that an increase of 1.0 kg/m2 was associated with increasing odds of wound complication by 7.2%. The aOR for tobacco smoking was 3.258.

DISCUSSION
In this study, we compared the rate of wound complications following DAA-THA with dressing choice of either iNPT or PM, using a logistic regression model that included dressing type, BMI, smoking, DM, liver disease, CKD, and anemia. We found evidence that increased BMI and smoking were associated with increased risk of superficial wound complications and that use of PM was associated with decreased risk of wound complications compared to iNPT (aOR = 0.555).
While DAA has become increasingly popular as a muscle sparing approach for THA, complications such as wound dehiscence and surgical site infections are commonly reported (Jahng et al. 2016). In fact, multiple studies suggest that wound complications may be more common with DAA than with other approaches, with overall risk of wound complication requiring intervention of 4.4-11.5% (Purcell et al. 2016; Jahng et al. 2016; Jewett and Collis 2011). The overall risk of wound complication in this study (9.00%) is within the range of previously reported rates of wound complication following DAA-THA. This may be due to thinner skin, higher shear forces, proximity to waist crease, mechanical irritation, and difficulty maintaining hygiene. Factors previously associated with increased risk of wound complication and increased rates of reoperation include increased BMI, diabetes mellitus diagnosis, and smoking tobacco. In one study, the odds ratio of wound complication following DAA THA for the highest BMI cohort (> 40 kg/m [Singh et al. 2020]) was 9.71 compared to normal BMI (Jahng et al. 2016). In another study, the rate of major wound complication was 4.8% among “low risk” patients and 25% among “high risk” patients, with BMI ≥ 30 kg/m2 and pannus included as “high risk.” (Kwon et al. 2018) Notably, the effect of increased BMI on wound complication after THA is greater with DAA than with the posterior approach, supporting hypotheses about the proximity to the pannus as a contributor (Watts et al. 2015). Our study supports this existing literature, showing increased risk of wound complications with increased BMI (aOR 1.072 on 1.0 unit of change, p = 0.007) and smoking tobacco (aOR = 3.258, p = 0.009). We did not find a significant association with DM diagnosis.
Previous studies on dressing use following THA or femoral incision have supported the use of both PM and iNPT separately. PM dressings were found in one retrospective analysis to be associated with significantly lower risk of delayed wound healing compared to silver-impregnated occlusive dressings (Herndon et al. 2020; Meffert et al. 2020). Similarly, iNPT has been found to significantly reduce major wound complications, reoperation, and readmission compared to standard gauze dressings in “high risk” cohorts (8.5% vs. 25% rate of wound complications) and to decrease surgical site complications compared with silver-impregnated dressings (Kwon et al. 2018; Scalise et al. 2015; Higuera-Rueda et al. 2021). Decreases in superficial infection, sero-hematoma formation, and dehiscence specifically with use of iNPT have been documented (Scalise et al. 2015). No studies were found directly comparing the use of these two dressings in the orthopaedic setting. One study was found comparing iNPT with PM directly in the setting of abdominoplasty, which demonstrated decreased fluid drainage and earlier drain removal with iNPT (Abesamis et al. 2019). Our findings show that after controlling for BMI and other medical comorbidities, use of PM was associated with decreased risk of wound complications compared to iNPT (aOR = 0.555, p = 0.047). Logistic regression models were utilized to account for significant differences in BMI and medical comorbidities between the PM and iNPT cohorts and adjusted odds ratios are reported.
There are several limitations of this study. Given that this is a retrospective cohort study, there was a significant prescription bias for iNPT in obese and medically complex patients. Using logistic regression, we were able to evaluate the effect of dressing type on wound complications while controlling for BMI and comorbidities. However, it is possible that prescription bias exists for variables other than those included in the regression, and therefore there theoretically could have been confounders not controlled for in this study. While operative technique was consistent over the study period for all patients, including a standardized incision that by protocol was no more than 2 cm larger in obese individuals, we could not perform statistical analysis using exact incision length with the available data. Incision length may contribute in small part to the increased overall complications among higher-BMI patients but was theoretically controlled for, at least in part, with the BMI variable in our regression. Another limitation is the smaller sample size of middle-high and high BMI patients. Furthermore, it was not possible to verify at-home compliance with post-operative wound care instructions or device malfunction after discharge. The data reported in our study therefore represents the outcomes associated with the prescription of either wound dressing for post-operative wound care with the intention of dressing use as prescribed. There is some chance that a subset of patients may not have maintained the seal on the iNPT device, in which case our conclusions may not represent “perfect use.” However, this is in itself an important consideration for providers when choosing a post-operative dressing for their patients. We believe that analysis of outcomes associated with surgeon choice of either dressing is of value for clinical practice. Finally, this study included three surgeons at one medical center. This is both a strength and a limitation; the different surgeons may have different criteria for choosing iNPT versus PM, and protocols may not be entirely uniform across the group. However, the use of patients from three surgeons also diminishes the likelihood of the specific practices of one surgeon influencing the overall results of the study and bolsters the generalizability of our findings.
Overall, these results indicate that after controlling for medical comorbidities, PM use is associated with a decreased risk of wound complication following DAA-THA compared to iNPT. Consistent with previous literature, greater BMI and tobacco smoking are associated with increased wound complications. These findings help inform wound care practices and identify modifiable risk factors after THA to improve patient outcomes and decrease the impact of complications.