

Introduction
Total hip arthroplasty (THA) is a commonly performed procedure in the current practice of Orthopaedic Surgery, with over 400,000 primary and revision THAs performed yearly (Levett et al. 2023). This common procedure is not without its risks however, as the development of local malignancy associated with THA has become increasingly recognized in the literature. Although osteosarcomagenesis is rare, questions regarding patient risk and its association with implant articulations continue. Recent literature has been published implicating Metal on Metal (MoM) articulation debris as a source of local inflammatory disease (Bozic et al. 2012), as well as increasing suspicion that prosthetic joint implant articulations may provoke a biological reaction that leads to the development of malignant tumors (Gillespie et al. 1988). The question remains whether there are particular types of implants that increase the likelihood of developing such malignancies. Until now research seems to have pinned the development of bone sarcomas to MoM or metal-on-poly articulations, while ceramic articulations have rarely been implicated. In January 2023 the first report of osteosarcoma around a Ceramic-on-Ceramic (CoC) THA was published (Levett et al. 2023), and here we report the first case report in the literature describing a high-grade osteosarcoma developing at the site of a ceramic on UHMWPE cementless total hip arthroplasty three years after undergoing index arthroplasty procedure. Osteosarcomas are extremely rare, comprising only 4% of all diagnosed sarcomas, with known risk factors including radiation, chronic infections, or exposure to chemicals in drinking water such as Fluoride or Radium (Burningham et al. 2012). This report opens the argument that the literature may have been wrong in their association of osteosarcomagenesis with metal, as a patient with no other risk factors developed such a malignancy, and that we may have to allocate more resources into investigating ceramic articulations as well.

Case History
The patient was a 50-year-old male who had initially sustained a dislocation of the right hip after a motor vehicle accident as a young adult. He ultimately developed post-traumatic arthritis of the right hip following an open reduction of the traumatic hip dislocation. The patient’s only pertinent past medical history included deep vein thrombosis and thoracotomy secondary to lung abscess.
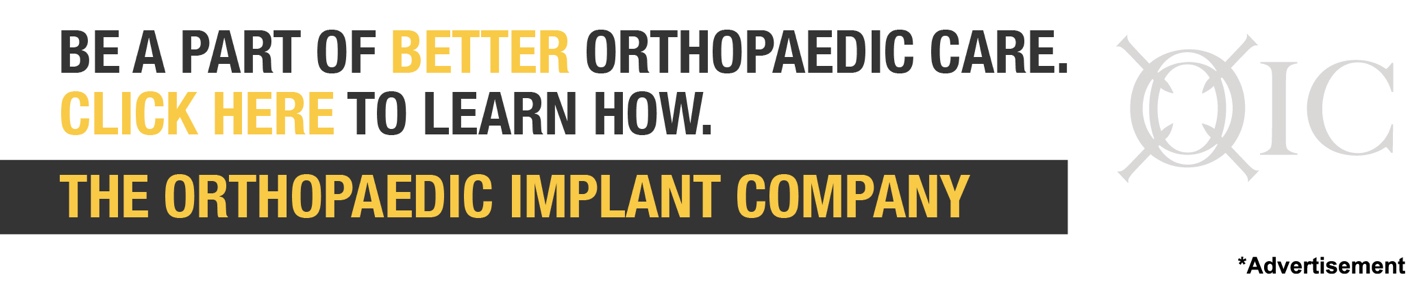
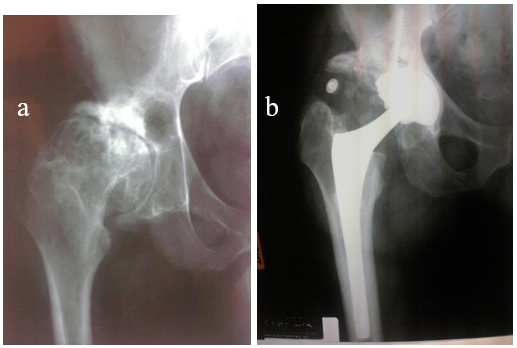
He underwent a total hip arthroplasty in January of 2008 for the post-traumatic arthritis, without postoperative complications. Radiographs at that time demonstrated no concerning findings (Fig. 1), and the patient recovered uneventfully from that procedure. At the time of the hip arthroplasty, no unexpected intraoperative findings were noted, and despite the prior trauma history the patient did not undergo perioperative hip radiotherapy for heterotopic ossification prophylaxis. The index pathology found no evidence of malignancy, noting “degenerative joint disease with a large subarticular pseudocyst and extensive fibro cartilaginous surface proliferation.” Three years postoperatively, the patient presented back to the primary arthroplasty surgeon, complaining of 1 week of ipsilateral hip and groin pain. On physical exam the patient had an antalgic gait but had painless PROM of the operative hip. Radiographs were without radiographic signs of loosening, nor aggressive features (Fig. 2).

_and_ap_radiograph_1-year_post-operative_(b)_confirming_the.png)
_and_ct_scan_of_gluteus_medius_muscular.png)
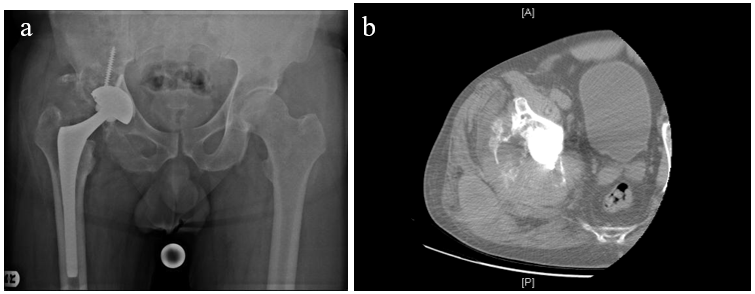
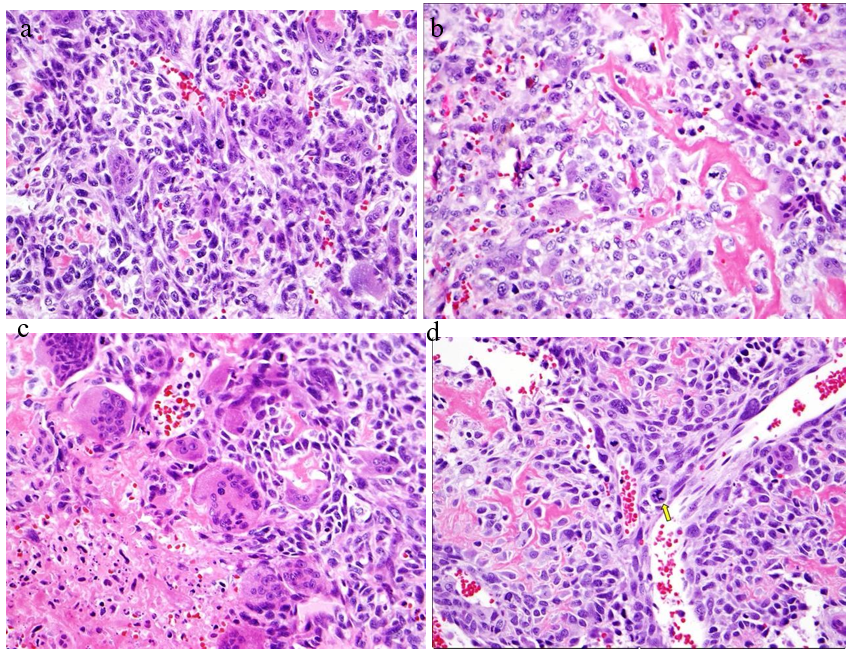
Three months later, the patient presented to our senior author with increasing pain in the right hip. At that time, in March 2011, the patient was admitted to the hospital and underwent a workup in suspicion of a periprosthetic joint infection. However, preliminary results were inconclusive for infection, and the decision was made to proceed with arthrotomy for tissue sampling. At the time of surgery, copious sanguineous fluid was yielded. Cultures and soft tissue samples for pathology were obtained. All final cultures were reported as negative; however, initial frozen sections revealed high grade osteosarcoma in all soft tissue samples (Fig. 3).
The patient was found to have developed a high-grade soft tissue osteosarcoma juxtaposed to the site of ceramic on cross linked polyethylene THA with metastatic lung disease, and was treated with palliative care, and subsequently expired.
._atypical__polygonal_oste.png)

Discussion
In a review of the available English language orthopaedic literature, there are no prior reports of osteosarcoma associated with alumina ceramic on UHMWPE articulations. Over the last 30 years, there have been approximately 40 number of cases associating in 8 series of bone and/or soft tissue tumors around the site of THA (Levett et al. 2023; Gillespie et al. 1988; Keel et al. 2001; Schuh et al. 2004; Lucas et al. 2001; Min et al. 2008; Rana et al. 2001; Syed et al. 2002; Stephensen et al. 1999; Visuri, Pulkkinen, and Paavolainen 2006; Memoli et al. 1986; Paavolainen et al. 1999). In humans, complications resulting from a THA vary from infection to the development of periprosthetic tumors. In our review, it is suggested that factors related to the surgery provide the trigger to tumorigenesis, though a definitive reason has not been determined. More likely, the presence of a foreign body is the predisposition. Such tumors may likely occur as a result from the wear and debris of implants, and can present as benign pseudotumors or could be associated with sarcoma (Levett et al. 2023). Serum levels of heavy metal ions in MoM articulations have been extensively reviewed, and osteosarcoma associated with CoC have recently been reported. The literature suggests that over time metallic implants will eventually corrode, and it is arguable that products of corrosion may be important in tumorigenesis (Bozic et al. 2012). This would seem less likely in ceramic articulations, where only the stem taper may be implicated. Although there are assumed etiologies of the development of periprosthetic masses and pseudotumors, the metastasis of such sarcomas is where the question remains. The majority of case reports of osteosarcoma following THA have been in canines, rather than humans. Interestingly, the wide time range to development of osteosarcoma in both canines and humans has been similar with intervals reported between 5 months and 19.5 years (Bozic et al. 2012; Gillespie et al. 1988; Burningham et al. 2012; Keel et al. 2001; Schuh et al. 2004; Langkamer et al. 1997; Goodfellow 1992; Solomon and Sekel 1992; Prasad et al. 2002; Dunn et al. 2012; Murphy, Parker, and Woodard 1997). Oncogenesis around the prosthesis has been revealed in animal experiments (Rana et al. 2001). According to large cohorts, however, the incidence of malignant tumors in THA patients is lower or similar to that in the general population (Syed et al. 2002). The causes of osteosarcomas can range from pubertal growth spurts, recessive DNA mutations, hereditary cancers, environmental/chemical exposures, and prior high dose radiation treatments (Burningham et al. 2012); none of which were relevant with our patient. In addition, the patient’s preliminary labs and imaging ruled out any preexisting malignancy or infection at the site of his THA, suggesting a potential association with his ceramic on UHMWPE cementless THA and the development of his osteosarcoma.

Summary
We report a patient with hip pain three years post THA, diagnosed with high-grade osteosarcoma at the site of the arthroplasty with metastatic lung disease, causing his eventual expiration. While the Orthopaedic implant may be associated in some individuals with local malignancy, the potential risk at this time remains theoretical, and causality has not yet been established in humans. It is undeniable that the benefits of THA far outweigh the risks of possible malignancy, while the nature of tumor development remains obscure (Prasad et al. 2002; Apley 1989). Moreover, the possibility remains that the development of a malignancy may be coincidental. Therefore, we conclude that it is prudent to report all documented cases to help shed light on this exceedingly rare but devastating situation.
Acknowledgement
The author(s) confirm that informed consent has been obtained from the involved patient(s) or if appropriate from the parent, guardian, power of attorney of the involved patient(s); and, they have given approval for this information to be published in this case report (series).