




Introduction
Total knee arthroplasty (TKA) is a treatment option for individuals with symptomatic osteoarthritis who have failed conservative therapy. The primary goal of this surgical procedure is to decrease pain, improve mobility, and increase patient quality of life. The incidence of total knee replacement internationally is approximately 175 procedures/100,000 population with the highest of 234 procedures/100,000 population for the United States (Kurtz et al. 2011). While there appears to be no clear accounting of TKA volume in the US, it has been estimated that over 1.025 million TKAs were performed in 2020 with estimated volumes growing to 3.4 million yearly TKAs by 2040 (Singh et al. 2019).
Although TKA has proven to be an effective surgical option for osteoarthritis, this surgical intervention is not free from complications. Potential post-operative complications include surgical site and joint infection, edema, hematoma, joint instability, continued pain, limitations of range of motion, implant failure, joint dislocation, vascular injury, and nerve damage (Curtis et al. 2018). Studies have reported that the dissatisfaction rate after TKA is as high as 19% with most of the patient concerns attributed to lack of pain relief, chronic edema, and lack of knee joint function (Bourne et al. 2010). Significant joint swelling is common following TKA surgery. One report noted a post-operative swelling prevalence of 15.6% among patients after TKA (Choi and Ra 2016). Additionally, total knee arthroplasty is noted to be the most common cause of non-cancer surgery-related post-operative causation of lymphedema (Dean et al. 2020). As the number of TKA procedures continues to increase at an accelerated rate, it is imperative to sufficiently mitigate potential preventable complications, both prior to and after the surgical procedure, to address the patient post-procedure dissatisfaction rates.
Herein the authors will describe the pathophysiology of post-operative edema and explore the patient dependent factors potentially contributing to lymphatic dysfunction and thus directly influencing the TKA postoperative course. The authors will also present their thoughts on a proposed multimodal perioperative protocol focused on identifying limb edema/lymphedema preoperatively, intraoperative technique changes that may decrease swelling, and lastly mitigating acute postoperative swelling response with the intent of decreasing pain, improving patient outcomes, and reducing the morbidity of chronic postoperative edema.

The Pathophysiology of Post-operative Edema
The universal response of tissue to injury, whether traumatically or surgically induced, is inflammation. If left unchecked, a swelling tsunami can ensue. Increased vascular permeability enables extravasation of fluid into the extracellular tissue spaces. Much of the fluid becomes displaced to the subcutaneous tissue (Tuckey et al. 2021). Increases in vascular permeability are believed to be the result of histamine and histamine-like permeability factors released because of the surgical intervention. Additional theories adhere to the belief that increased vascular permeability is directly due to overt vascular or cellular injury (Tuckey et al. 2021). Extensive surgical dissection results in endothelial cell disruption and may take several days to weeks for repair and regeneration to begin. The more extensive the procedure, the more damage cellular structures sustain, resulting in a prolonged state of edema. If leg edema (lymphedema, chronic venous insufficiency, or lipedema) existed prior to the surgical procedure, the edema is typically exacerbated postoperatively, prolonging recovery and potentially increasing complication occurrence.
Lymphatic vessels play a key role in removing the protein-rich fluid from the tissues and rapidly dilate to several times their normal caliber early in the inflammatory phase to increase overall lymphatic flow rates (Tuckey et al. 2021; Brown et al. 2023; Azhar et al. 2020; Schwager and Detmar 2019; Sung et al. 2022). Increased tissue edema and dermal lymphatic stasis results in a proinflammatory state. Normal functioning lymphatic mechanisms and venous drainage are required for the body to remove inflammatory mediators from the subcutaneous tissues (Brown et al. 2023; Azhar et al. 2020; Schwager and Detmar 2019). Impaired vascular perfusion at the microvascular level results not only in subcutaneous fluid build-up in the tissues, but also an accumulation of pro-inflammatory substances which have been attributed to the continuous nociceptor activation and related pathophysiological states including central nervous system sensitization and neuroinflammation (Tuckey et al. 2021; Brown et al. 2023; Azhar et al. 2020; Schwager and Detmar 2019; Sung et al. 2022). It is well-established that persistent, peripheral nociceptive sources can initiate, maintain, and perpetuate chronic pain states, with tissue injury and inflammation leading to the local release of substances including glutamate, serotonin, bradykinin, Substance P, nerve growth factor, and norepinephrine (Tuckey et al. 2021). These substances are transmitted to the central nervous system by primary afferent nociceptors resulting in a lower set point for nociceptor activation thresholds in the periphery, hence contributing to chronic pain (Tuckey et al. 2021). To put it succinctly, swelling and associated dermal lymphatic stasis directly contribute to acute postoperative pain and play a part in the initiation of chronic pain states.
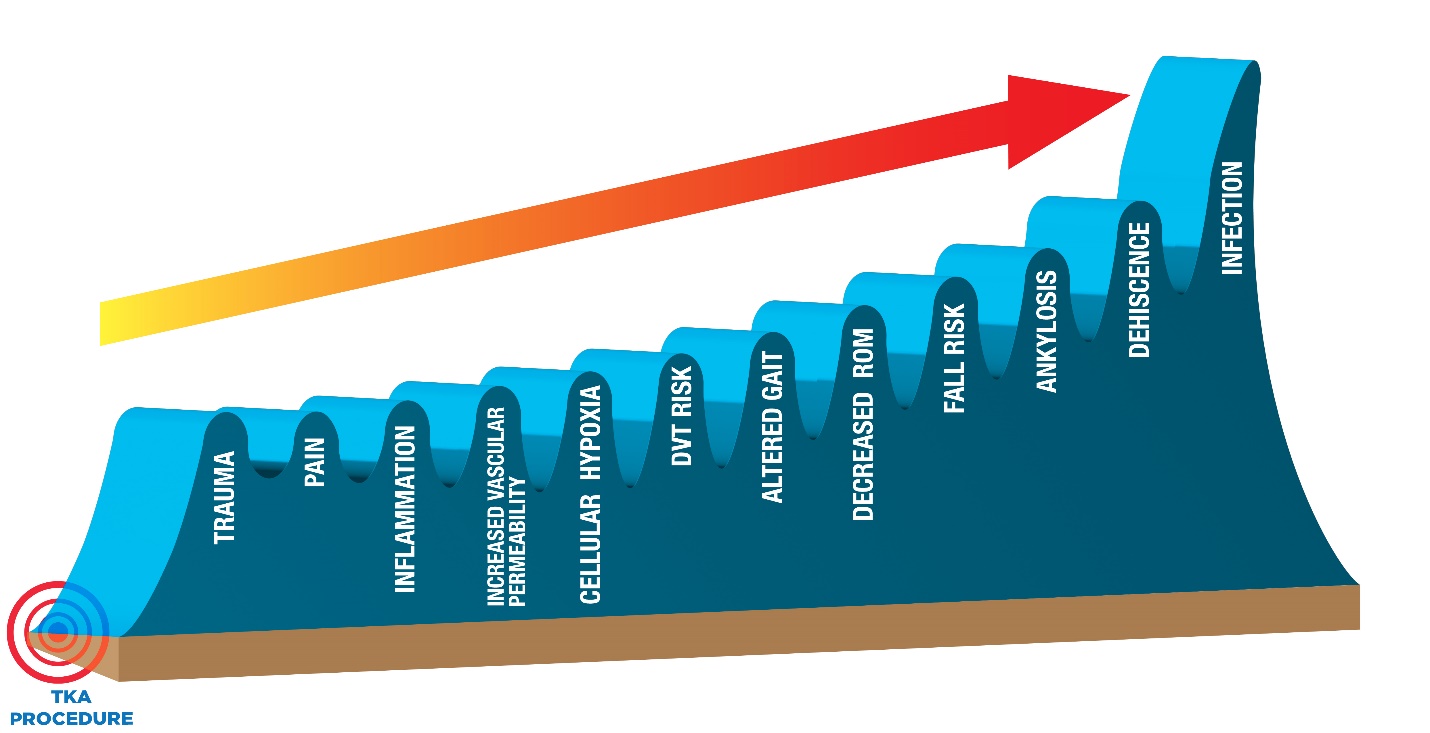
Swelling and pain related to joint replacement procedures are the most frequent post-operative patient complaint, being associated with increased emergency department visits, readmissions, poorer patient outcomes and contributing to escalating total cost of care. Following TKA, 13.8% of patients will have at least one emergency department visit (Kelly et al. 2018). The most frequent symptoms were pain (15.8%) and swelling (15.6%) (Kelly et al. 2018). The thirty-day readmission rate for primary TKA and revisional TKA was 4.8% and 7.2% respectively (Papakostidis et al. 2021). In the acute post-operative phase of healing, uncontrolled post-operative swelling and pain can lead to hospital re-admission for pain management and/or arthrofibrosis and excessive scarring (Cheuy et al. 2017). Arthrofibrosis can contribute to decreased range of motion (ROM) and alterations in gait mechanics which may subsequently increase the likelihood of DVT development and increase fall risks (Cheuy et al. 2017). Additionally, chronic tissue edema leads to cellular hypoxia which can lead to surgical site infections (SSI), surgical site dehiscence, scar tissue formation, and joint ankylosis. These multiple effects can result in a post-operative swelling Tsunami. (Figure 1)

Measuring Post-operative Edema
Postoperative edema is an anticipated sequela of TKA. However, swelling has extreme patient variability, as some patients have minimal swelling, and others develop remarkable postoperative edema. This variability may be due to preoperative undetected or underappreciated edema/lymphedema, chronic venous insufficiency, lipedema, genetics, or variation in operative technique and post-operative protocols. Consistent, reproducible, economical measuring of pre-operative and post-operative edema can be a challenging task. Localized assessment of edema can be done with simple circumferential measurements using a tape measure. However, this method does not differentiate edema volume and muscular volume and provides only a rough estimate of volume changes at best. Thus, these measurements are likely the least reliable for the assessment of post-orthopedic edema trends. Quantitative measurement of peripheral edema of the leg can be measured either directly by water-displacement, bioimpedance spectroscopy (BIS), ultrasound (US), MRI, or indirectly by calculation of the volume based on circumferential measurements (Brodovicz et al. 2009). At present, it appears that bioimpedance devices may have the most utility and validated published data of the available options.
Various edema measurement methods are further described in Table 1, along with the authors’ clinical experience and observed advantages and disadvantages.
Two important studies quantified post-operative swelling using bioelectrical impedance technology. In 2015 a study by Pua and colleagues examined the time course of knee swelling post total knee arthroplasty (TKA) (Pua 2015). Eighty-five patients with unilateral TKA were enrolled in the study. Extracellular fluid volume was quantified using BIS preoperatively and on post-operative days 1, 4, 14, and 90 (Pua 2015). Knee swelling increased ~35% from preoperative levels when measured one day post-op. Additionally, knee swelling reduced but remained at ~11% above preoperative levels on post-op day 90 (Pua 2015). In longitudinal, multivariable analyses, knee swelling was associated with quadriceps weakness (P<0.01) and slower gait speed (P=0.03) (Pua 2015). The investigators concluded that interventions to reduce post-TKA knee swelling may be indicated to improve patient function and satisfaction.
A second study by Loyd et al provided the first published data regarding normative reference data following TKA (Loyd et al. 2020). Like Pua, Loyd and his group used bioelectrical impedance assessment (BIA) to track post-operative swelling. From this information, the research group used statistical predictions to develop a swelling curve for the first 7-weeks after TKA (Loyd et al. 2020). The researchers observed that edema increased approximately 10% per day for the first 3 post-operative days peaking between post-op days 6-8 (Loyd et al. 2020). Patients in the 10th percentile demonstrate a peak swelling of approximately 22%, while patients in the 90th percentile peak at 46% (Loyd et al. 2020). This work highlights that patients who have excessive swelling immediately post-op will have long-term swelling issues compared to their counterparts who had less swelling. Loyd et al observed that even at 7 weeks after surgery, the patients that reached the 90th percentile swelling remained approximately 34% more swollen than pre-operatively while the lowest centile still contended with 12% more swelling (Loyd et al. 2020). The investigators concluded that the use of their reference chart provided a novel framework to monitor swelling following total knee arthroplasty, providing an objective measure to guide clinical decisions in order to improve postoperative swelling management.

How common the assessment of edema is performed before or after TKA is unknown. Judging from the relative lack of swelling research papers in the past decade, there appears to be a paucity of providers routinely assessing perioperative leg swelling. Historically, if measurements were obtained, it was through the rudimentary use of a tape measure. There is a need for a simple, validated, cost-effective edema measuring device to accurately assess the efficacy of edema reducing interventions. Ideally, this tool would enable providers to initiate edema reducing interventions in a consistent and timely manner to better mitigate swelling complications.
Of the devices available on the market, the lead author uses a bioelectrical impedance spectroscopy tool as it can be easily performed by a medical assistant pre- and post-operatively, and it discretely assesses for edema. Two clinically available devices are the In Body system, a BIA (Bioelectrical Impedance Analysis) device, and the SOZO which uses BIS. The recently published research utilizing these types of devices provide some basis upon which to measure a patient’s edema status post-operatively allowing appropriate management if/when edema is trending higher than the mean. Furthermore, with advances in remote monitoring technologies, one could easily envision an app-based system that would allow the provider to track a patient’s progress regarding edema, ROM, activity, and intervene when data demonstrates values falling outside the norm. Widespread adoption of swelling monitoring would be welcomed and feasible in the space by providers and patients alike (Ridner et al. 2014).
Peri-operative protocols
This section summarizes the authors’ recommendations for peri-operative protocols gleaned from evidence-based practices. The aim of this work is to provide surgeons with a pre-, peri-, and post-operative protocol to minimize the negative impact of edema on post-surgical outcomes. These algorithms were designed to improve lymphatic and immune function, decrease post-op swelling, and reduce post-operative pain therefore improving patient mobility, decreasing surgical site complications and potentially accelerating post operative patient outcomes. Additionally, the authors hypothesize that attention to this topic will decrease hospital readmission rates, reduce need for post-surgical care related to post-operative complications, reduce ER visits and the use of narcotics/opioids, and most importantly improve patient outcomes and satisfaction.

Pre-operative Stage
Based on clinical experience, it is the authors’ belief that individual patients have a unique inherent inflammatory response to trauma. Therefore, each patient will exhibit a distinctive swelling recovery curve based on various local and systemic factors including the efficiency of their lymphatic transport system and the function of their venous tributaries. Primary and secondary lymphedema impacts a significant demographic of the general population. General prevalence is estimated to be 5.4 per 1,000 people in individuals aged >65 and 10.3 per 1,000 individuals aged >85 years (Moffatt et al. 2003). The incidence may be higher in patients that have had deep venous thrombosis, significant trauma, prior history of malignancy with lymph node resection (Moffatt et al. 2003). A thorough pre-operative patient assessment should include screening for chronic venous insufficiency (CVI) and lymphedema. CVI has been demonstrated to increase implant-related complications, venous thromboembolism events (VTE), length of stay (LOS), overall costs of care, and readmission rates (Summers et al. 2021). Chronic lymphedema is often associated with advanced CVI (known as Phlebolymphedema) and may be associated with increased surgical site infections (SSIs) and progressive postoperative edema secondary to progressive lymphedema (Kolz et al. 2020).
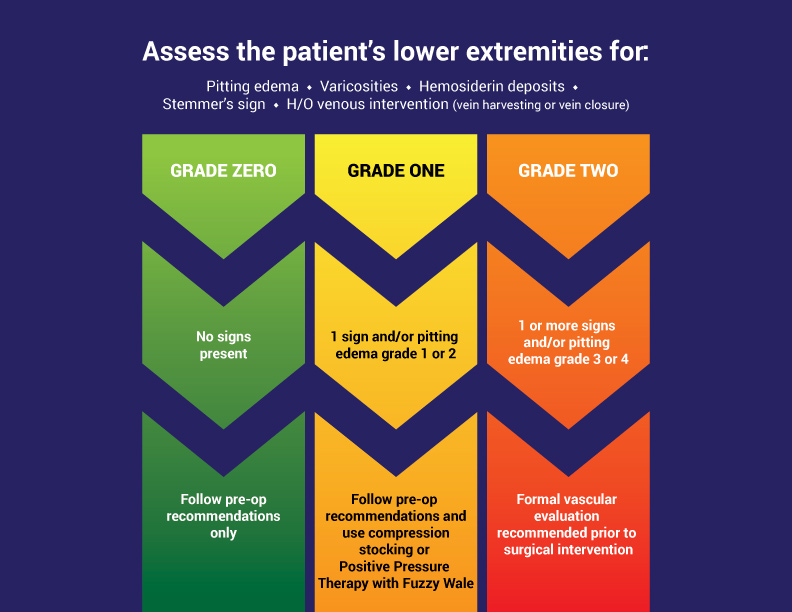
Orthopedic surgeons performing hip and knee replacement should implement a peri-operative patient swelling optimization pathway within their practice. This algorithm would be in addition to other optimizations goals such as tobacco cessation, controlling sleep apnea, HGBA1C, anemia, albumin, etc. The authors propose the following decision tree and subsequent lifestyle interventions be implemented in the weeks to months prior to surgical intervention. The authors propose dividing patients preoperatively into three groups, with the understanding that there is no current validated classification system. (Figure 3)

Clinicians should also complete the following patient assessments:
-
Evaluate medication list. Work with primary care provider to modify/stop medications that contribute to lower extremity edema (such as Amlodipine/Norvasc), ideally 4 weeks prior to the planned surgical procedure (Largeau et al. 2021).
-
Patients >70 years of age or <70 and a history of current or previous tobacco use and/or diabetes may have increased risk for PAD (Hirsch 2001). Consider an arterial vascular evaluation (such as Ankle Brachial Index and/or arterial ultrasound) in these at-risk patients.
-
For those patients with clinical evidence of chronic venous disease (hemosiderin deposition, varicose veins, history of venous leg ulcers, history of deep vein thrombosis, chronic leg edema) a venous competency ultrasound should be performed to evaluate both superficial and deep venous anatomy for valvular reflux. Consider consultation with vascular surgery or vein specialist if significant venous reflux is present. This type of ultrasound is distinctly different than a “rule out DVT ultrasound”. The authors recommend meeting with a vascular specialist and certified lymphedema specialist prior to implementation to:
-
review your goals
-
understand how treatments differ based on underlying edema etiologies (arterial issues, CVI, lymphedema, mixed causes),
-
reassess program at quarterly intervals until steady state.
All three specialists need to “buy-in” to 21st treatment. Otherwise, this step will likely lead to frustration for patient and orthopedic surgeon. In addition, create education pamphlet for patients describing what benefits they will see with this additional intervention (eg reduced complications) to drive patient compliance.
-
In addition to the above, all clinicians should recommend the following patient lifestyle modifications.
-
Ideally, normalization of BMI with a target between 20-30, but even a small drop in BMI has been correlated with lower post-op complications. Consider nutritionist evaluation/consult (van der Heijden et al. 2017).
-
Initiation of an anti-inflammatory diet (Mediterranean diet style food choices) (Cooper et al. 2022)
-
Cessation of all tobacco use, including cigarettes, vapes, and smokeless tobacco.
-
Limit alcohol intake to 1 drink daily
-
A low sodium diet and no added salt to foods supports a decrease in dermal edema and improved microvascular function (Martin et al. 2023)
-
Begin exercise plans to improve leg lymphatic and muscle pump function. The following are sample regimens.
-
Walk, bicycle, swim, or use elliptical or rowing machine for 15-30 minutes daily based on pain tolerance.
-
During breakfast, lunch and dinner do 10 calf raises and twenty march in place exercises (Padberg, Johnston, and Sisto 2004).
-
Diaphragmatic breathing 2x/hr while awake.
-
-
Initiate nutritional supplements 2-4 weeks pre-operatively to support post-operative healing (protein [egg whites, protein powders or drinks], vitamins A, B [B12, B6, folic acid], C, D, and zinc). Additionally, diosmin micronized purified flavonoid fraction (MPFF) has been demonstrated to decrease tissue edema in patients with lymphedema or chronic venous disease. MPFF should be initiated in patients demonstrating venous disease or lymphedema 2 weeks to 2 months preoperatively and continued for 2-4 months post-op for the best results (Penny et al. 2022).
Pre-operative Compression Utilization in the TKA population
Routine/traditional prescription and utilization of compression garments in this patient population can be a challenge in both the pre- and post-operative phase due to limited ROM and difficulty with donning compression over the surgical site. Innovative textiles such as the longitudinal elastic stockinette or Velcro adjustable wraps applied from foot to thigh offer post-surgical patients an alternative to ‘old school’ knee high compression stocking. The authors of this work have had significant reduction of edema in both the pre-operative and post-operative patient following the inclusion of the longitudinal elastic stockinette. This innovative textile is inexpensive, patient friendly and effective at edema reduction without impairing the patient’s functional movement. The authors want to caution the reader regarding the antiquated utilization of TED stockings or elastic wrap (ace wrap) to manage lower extremity edema in the peri-operative phase, as there is no validated data for either. TED stockings should only be used for post-operative DVT prevention and must be used per manufacturers standards and only in non-ambulatory patients (Sachdeva, Dalton, and Lees 2018). TED stockings are contraindicated for use in ambulatory patients (Sachdeva, Dalton, and Lees 2018).

Intra-operative Stage
The authors recommend incorporating the following intra-operative/PACU checklist into TKA algorithms. This list was developed through a culmination of personal experiences and best practices noted in current literature.
-
Sequential compression device to the non-operative leg (Nester and Borrelli 2022)
-
Consider foregoing intraoperative tourniquet use, as there is theoretical risk of injury to the ventromedial lymphatic bundle that could increase post-operative edema/lymphedema occurrence. A study found that TKA with tourniquet use was associated with increased risk of skin necrosis and deep wound infection, also noting this group had less postoperative swelling and a lower incidence of wound complications in the early post operative period (P<0.05) (Liu et al. 2017).
-
Surgical atraumatic technique. Consider using a scalpel versus electrocautery (Tammachote and Kanitnate 2018)
-
Leave medullary canal undisturbed (Napier et al. 2014; Wu et al. 2019)
-
Consider kinematic alignment versus conventional mechanical alignment for less ligament releases (McEwen et al. 2020)
-
Closure of the capsule and skin in flexion (Napier et al. 2014; Wu et al. 2019)
-
Adding topical Tranexamic acid (TXA) in addition to IV or PO route (Huang et al. 2014). The author’s preferred method of delivery is closure of capsule followed by injection of 10cc (1GM) TXA into the suprapatellar pouch.
-
Consider applying compressive post-operative dressing or garment. The authors currently recommend the patented EdemaWear® product (Compression Dynamics) as it provides dermal interaction and light compression (8-12mmHg) using the thigh high “small-shaped” product for patients with thigh circumference less than 24" and the medium thigh high product for thighs measuring >24". It is easier for patients to apply, making compliance more likely and has characteristics not found in other devices on the market at present.
-
Leave the knee in 90 degrees flexion post-operatively until physical therapy for up to six hours maximum or until physical therapy is initiated to decrease bleeding and decrease downstream edema (Han et al. 2021)
Post-operative course
Postop protocols vary widely from surgeon to surgeon, and few are comprehensive and multidisciplinary. Up until the initiation of Bundled Payments for Care Improvement (BPCI) and other bundled payment programs, many patients were discharged to an inpatient rehabilitation center followed by outpatient therapy for multiple more weeks. Home-based physical therapy has shown merit and can result in overall cost savings and improved patient satisfaction (Hoogeboom et al. 2014). The trend towards home-based therapy was significantly accelerated by the Covid pandemic. Contemporaneously, the opioid epidemic helped push innovation in the post discharge arena with many surgeons redefining postoperative protocols.
The following protocol is what we believe to be the ideal post-op protocol to reduce swelling at the present time. It is the amalgamation of the authors’ experiences with postoperative patients combined with the Loyd et al (Loyd et al. 2020) swelling curve chart as well as swelling interventions from the literature. Importantly, patients need education preoperatively regarding the protocol using written and video tutorials to explain why adherence leads to better outcomes and lower pain and swelling. Postoperative education in a daily method for the first 4 weeks after TKA describing normal findings and encouraging adherence to the protocol is the key to success.
HOME RECOVERY weeks 1 thru 2
-
Tranexamic acid plan (3 additional doses q 4 hours OR one dose daily for 14 days). Multiple TXA TKA studies have been published without reports of patient seizures, but the lead author believes that a single daily dose for 14 days may be the best option (Murao et al. 2021; Wang et al. 2019).
-
Continue low sodium, anti-inflammatory diet
-
Continue micronutrient supplements as previously detailed in the lifestyle modification section (amnio acids and micronized purified flavonoid fraction (MPFF))
-
Employ an easy-to-use compression device or bandage such as longitudinal elastic stockinette or Velcro adjustable wrap covering the limb from foot to mid-thigh.
-
Physical therapy (Stevenson and Wickline 2020) to include:
-
Limited weightbearing with assistive device for 1 week minimum
-
5-8 minutes of range of motion exercises per hour while awake.
-
seated knee flexion/heel slides (10/hr)
-
passive/active assisted knee extension (10/hr)
-
10 ankle pumps/hr
-
walk 5-10 steps/hr
-
10-minute heel hang 3x/day
-
Elevation of limb 40min/hour for first 10-14 days (toes above nose)
-
Ice 40 minutes/hour to surgical limb for first 10-14 days
-
Limit stair descent/ascent as much as possible.
-
Isometric quadriceps sets in full extension, no isotonic or closed kinetic chain strengthening
-
focus on ROM with minimum goal of 0-110 by POD #14
-
-
Step count
-
750 steps/day maximum WEEK 1
-
1200 steps/day maximum WEEK 2
-
-
Consider additional intervention for patients not meeting post-operative milestones (ROM <90 or >35% edema at POD 7, ROM <105 and edema >25% at POD #14) such as manual lymphatic drainage, sequential compression device and/or electrical muscle stimulation devices.
HOME RECOVERY week 3-6
-
Continue anti-inflammatory diet
-
Continue micronutrient supplements and MPFF for 2-3 months to assist in edema reduction
-
Employ an easy-to-use compression device
-
Physical therapy to include:
-
progress away from assistive devices as tolerated.
-
5-8 minutes of range of motion exercises 6x/day
-
Elevation and icing of limb 40min 3x/day at minimum, more if needed.
-
isometric quadriceps sets in full extension, no isotonic or closed kinetic chain strengthening until 6 weeks post-op
-
Focus on ROM—ideally achieving maximum intra-op best ROM by week 4.
-
-
Step count
-
2000 steps/day maximum WEEK 3
-
2750 steps/day maximum WEEK 4
-
3500 steps/day maximum WEEK 5
-
4500 steps/day maximum WEEK 6
-
progress by 1000 steps/day in each subsequent week letting pain/swelling be the guide.
-
-
Consider additional intervention such as manual lymphatic drainage, sequential compression device, electrical muscle stimulation device if needed
-
Carefully consider returning to work prior to 6 weeks post-op. It is the authors’ experience that this generally results in loss of range of motion and may lead to a less than optimal outcome for many patients. Consider patient progress and job requirements and how the job specifics will influence the potential for increased swelling (standing/stairs/lifting increases swelling) to develop the appropriate return to work plan.

Conclusion
While knee arthroplasty is routinely performed by orthopedic surgeons, an interdisciplinary approach to collaborative patient care can improve management and mitigation of the common malady termed post-operative swelling. Given the high incidence of post-operative swelling, it remains an enigma that upstream consistent therapy application remains largely absent in most orthopedic practices. The national rates of 30- and 90-day readmissions after primary TKA were 4% (95% CI, 3.8%-4.0%) and 7% (95% CI, 6.8%-7.2%), respectively (Kurtz et al. 2017). Decreasing these readmission rates may be possible by pre-operative identification of potential peri-operative factors contributing to lymphatic dysfunction and post-operative edema development. This specifically allows upstream management and accelerated outcomes for pain control, decreased opioid use, improved ROM and decreasing the complications of SSI, DVT and limited mobility. A positive impact on these negative post operative outcomes has a high potential to improve patient satisfaction.
The identification, treatment, and long-term management of lymphedema and lower extremity edema is not a commonly taught discipline within medical education (allopathic, podiatric, physician assistants, nurse practitioners). Too often, this undiagnosed swelling tsunami negatively impacts surgical outcomes, leaving the surgical team with the challenge of treating “in the moment” the costly effects of a SSI, DVT or a joint infection, while in fact the source of the issue existed long before the incision on the skin overlying the knee was performed.
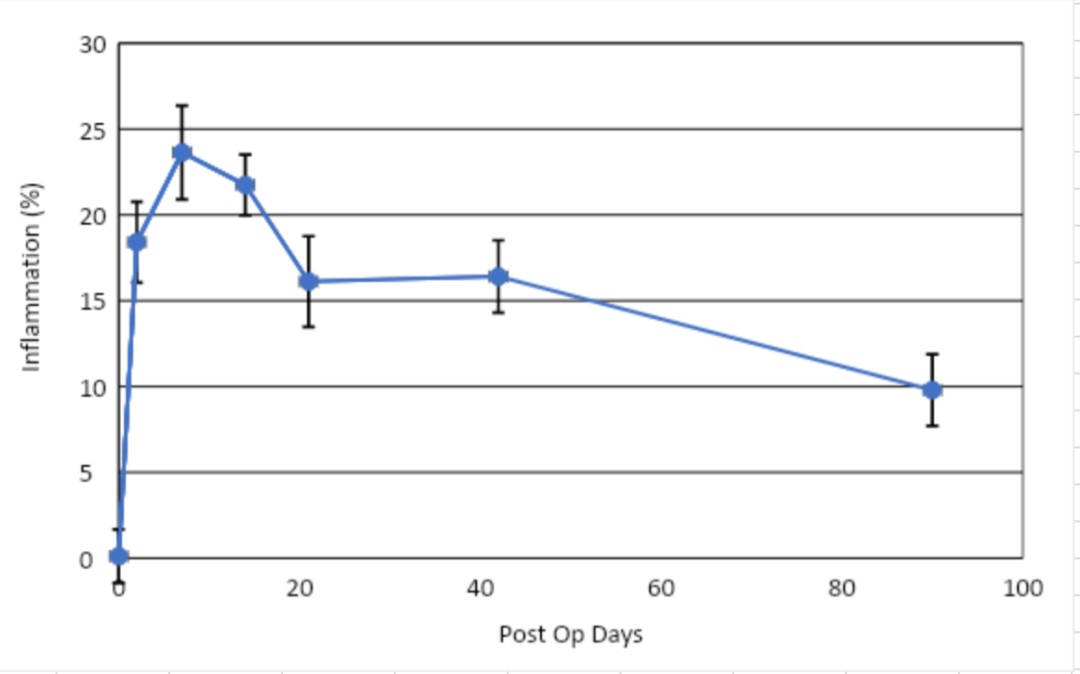
Perioperative patient assessments and interventions can have multiple tangible effects on patient outcomes, limiting swelling, decreasing pain, and increasing joint function. Early intervention and dedicated post-operative protocols have proven to be beneficial in the lead authors’ clinical practice. Using the same bioelectrical impedance assessment measuring device and by applying some, but not all, of the principles outlined in this manuscript, the lead author has been able to demonstrate a roughly 20%/10% reduction in max/avg swelling at POD7 and 14. (Figure 4—Y axis BIA, X axis post-op days)

Upstream thinking and checklist applications pre-operatively can vastly improve TKA outcomes for the orthopedic surgical teams, though most importantly for the patients and families we serve. To successfully achieve this goal, the authors suggest the following “call to action” steps:
-
Develop a standardized swelling grading system for the TKA population
-
Validation of cost-effective swelling measurement devices and accompanying reference curves
-
Development of a multicenter data registry to compile swelling data based on perioperative protocols
-
Set the following clinical goals
-
Identification of those patients’ at-risk pre-operatively
-
Develop a consensus on optimal interventions to reduce swelling and limb volume
-
Follow RTW (Return to Work) data, opioid usage, 90-day costs, and 90 day recidivism
-
Determine current actual secondary lymphedema occurrences related to TKA and then determine whether or not aggressive intervention for all patients is beneficial
-
Prove/disprove that swelling reduction yields faster RTW, lower opioid use, decrease complications and/ or lower 90-day costs
-
Preparation is the key to success. Optimizing patient outcomes following knee replacement requires proactively managing the expected postoperative total knee swelling tsunami.
Acknowledgements
The authors would like to recognize Amanda Godwin and Luis Ignacio Pintos of the American Vein & Lymphatic Society for their assistance in creating the figures presented in this manuscript.