

Introduction
Total joint arthroplasties (TJA) are among the most common procedures performed in the United States, and each year, the volume of these procedures is increasing. By 2030, an estimated 635,000 total hip arthroplasties (THA) and 1.25 million total knee arthroplasties (TKA) will be performed annually (Sloan, Premkumar, and Sheth 2018). Many arthroplasty surgeons perform multiple TJA procedures over the course of a single surgical day, with some utilizing more than one operating room (OR) in a staggered fashion. Since primary TJAs are largely elective and predictable, surgeons can organize case order as they see fit, however patients often express personal scheduling preferences with many desiring to be the first case of the day (Ahmed and Ali 2020; Kamran et al. 2019; Ozen et al. 2016). Many believe that afternoon/evening surgeries may take longer or may have worse outcomes due to surgeon or staff fatigue (Janhofer, Lakhiani, and Song 2019; McCormick et al. 2012). In the existing literature, few studies provide actual evidence that can guide these patient discussions.
In the orthopedic spine literature, studies have shown that afternoon anterior cervical discectomy and fusions (ACDFs) and posterior lumbar fusions (PFLs) have increased LOS when compared to morning start cases (Mayo et al. 2016; Neifert et al. 2020). After-hours orthopedic trauma cases have also been shown to have higher mortality and complication rates (Halvachizadeh et al. 2019). In the arthroplasty literature, however, the results have been less consistent. In 2016, Keswani et al. found that patients undergoing THAs after 2 PM had significantly longer LOS than those before 2 PM (Keswani et al. 2016). In this study the average LOS for both groups was greater than three days, and recent THA trends have shifted dramatically towards shorter LOS’ and more ambulatory operations (Fu et al. 2017; McClatchy et al. 2021). In 2020, when studying periprosthetic joint infection (PHI) risk, Yildiz et al. found no difference among TJA patients who were operated on in the morning or afternoon (Yıldız et al. 2020). Kwon, et. al., conducted an randomized control trial of ambulatory THAs and found that patients who underwent afternoon surgery had a more rapid return to baseline inflammatory marker levels (cortisol, IL-6, and IL-8) (Kwon et al. 2019).
In this study, we investigate the effect of surgical start time on operative duration for patients undergoing elective TJA. This study aims to provide clinicians with data that can inform scheduling and pre-operative patient discussions.

Methods
Cohort Selection
This was a retrospective cohort study, and the study population was identified via chart review from our large, urban, academic medical center. Patients who underwent primary TKA or THA between May 2014 and May 2018 were identified by querying for CPT codes 27447 and 27130 (primary TKA and THA, respectively). Patients were included only if they were older than 21, if their surgeon was arthroplasty fellowship trained and conducted >50 TJAs annually, and if they did not have a -22 CPT modifier attached for increased operative complexity. Patient demographic information (age, sex, BMI, ASA score, self-reported race, and insurance status) was recorded for each patient. For each operation, operative start time, whether it was the surgeon’s first case of the day, and operative duration (from incision to closure) were recorded. Anesthesia times, set-up times, and turnover times were not collected in this study. Assuming a 12-hour OR day, operative start times were categorized into three 4-hour periods: 1) “early” non-first start cases starting between 7:00 AM to 11:00 AM; 2) “mid-day” cases starting between 11:00 AM and 3:00 PM; and 3) “late” cases starting after 3:00 PM. An additional sub-group analysis of early cases was performed specifically for the first-start case of each operative day. This study was approved by our institutional review board.
Statistical Analyses
First, association between patient demographics and operative start time were determined using chi-squared tests. Second, the association between operative start time and overall operative length was analyzed using one-way ANOVA. Finally, to better account for patient and operation specific factors, a multivariate linear regression (MLR) model was built to determine the association between operative start time and operative lengths while holding all other variables equal. Coefficients with 95% confidence intervals were calculated for each variable to estimate effect size on operative times for both THA and TKAs. P-values less than 0.05 were considered significant. All statistical analysis was done in R (version 3.6.2, Rstudio Inc, Boston, MA).
Results
Our search yielded 869 TKAs and 791 THAs. Among TKA patients, 319 (36.7%) early, 437 (50.3%) were mid-day, and 113 (13.0%) were late cases. Of patients in the early group, the majority (211; 66.1%) were first-start cases. Patients who underwent surgery in the early group were more likely to have ASA scores 1-2 (p<0.001), have lower BMIs (p=0.012), and have commercial insurance (p<0.001) (Table 1). We found no correlation between case start time and sex or self-reported race.
Among THA patients, 407 (56.6%) early, 297 (37.5%) were mid-day, and 87 (11.0%) were late cases. Of patients in the early group, the majority (327; 80.3%) were first-start cases. Patients operated on in the morning were more likely to be less than 60-years-old (p<0.001), self-report as white race (p=0.018) and have ASA scores 1-2 (p<0.001). (Table 1). We found no significant correlation between early cases and sex, BMI, or insurance status.
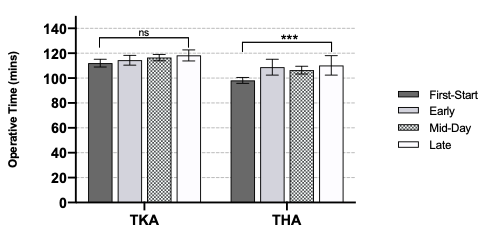
When analyzing the effect of start time on operative lengths, our ANOVA identified a statistically significant difference among the four start time groups for THA patients (p<0.001), but not for TKA patients (Figure 1). However, when considering all other variables, our MLR identified that for TKAs, mid-day cases were 4.9 minutes longer (p=0.04) and late cases were 7.3 minutes longer (p=0.013), when compared to first start cases. Similarly, for THA mid-day cases were 9.1 minutes longer (p<0.001) and late cases were 11.8 minutes longer (p<0.001) on average (Table 2).

Discussion
Although TJAs are some of the most common elective procedures done in the United States, little has been published about how operative scheduling affects outcomes. In the non-arthroplasty orthopedic literature, afternoon or evening start times have been associated with increased operative times, LOS, and complication rates (Halvachizadeh et al. 2019; Mayo et al. 2016; Neifert et al. 2020). The arthroplasty literature, however, has been more ambiguous. Some studies showing afternoon cases having increased LOS, while others show no difference in other outcomes measures (Keswani et al. 2016; Kwon et al. 2019; Yıldız et al. 2020). In this study, we analyzed the association between operative start and overall surgery length for total hip and knee arthroplasties.
We found several demographic variables were predictive of early start time. Specifically, white, younger, healthier patients (ASA 1-2) with commercial insurance were more likely to be scheduled as an early case. In addition, non-obese patients were more likely to be scheduled in the AM when undergoing TKA. Yet despite variations in surgical start time, our findings indicated that surgical start time has a minimal effect on the operative length for THAs. Our MLR demonstrated having a THA surgical start time other than first start was associated with a statistically significant increase in operative times by 9.1 to 11.8 minutes. For TKA patients, our MLR demonstrated significant differences in operative times among the mid-day, and late cohorts with operative durations increasing 4.9 to 7.3 minutes. While these differences were significant when controlling for confounding factors such as age, self-reported race, ASA score, and insurance type, the actual magnitude of time increased was small. These results indicate that time-of-day scheduling has only minimal effects on surgical efficiency for TJAs. These findings better inform conversations with patients who desire early operation or first start cases.
Non-first start times being associated with a slightly increased operative length for TJAs may be explained by a confluence of factors. First, this could be a result of surgeons intentionally scheduling more complex patients later in the day. At our institutions, surgeons have complete discretion over their surgical schedule, and in general, surgeons will perform more routine operations earlier in the day and more complex operations later to prevent early delays. Complex cases will logically take longer to complete than routine ones. Next, surgeon fatigue may play a role in later cases. Another factor that may explain these findings is that TJAs require a coordinated, interdisciplinary operative team to properly utilize hip and knee implantation systems. Additionally, at our academic center, fellows and resident physicians are the first assists for the vast majority of cases. The amount which an attending physician involves a resident can vary based on a myriad of factors including time of day. Cases with more active resident education inherently have some additional degree of inefficiency. Additionally, during non-first start cases, dedicated arthroplasty scrub-technicians may have been handed off to non-arthroplasty scrub-technicians. These unfamiliar surgical assistants may require more time and guidance in properly assembling the surgical tools (Doll et al. 2017; Epstein et al. 2017; Giugale et al. 2017). Finally, our surgeons routinely utilize intra-operative fluoroscopy to confirm implant positioning. Radiology technicians working the later shift may be less familiar with intraoperative imaging protocols and can cause significant delays.
Ultimately, this study has multiple inherent limitations. First, the study’s retrospective design makes it impossible to draw causal links between start time and operative length. The study design was also reliant on billing data to identify patients and exclude complex cases – billing data inherently has some inaccuracies, and .22 CPT code modifiers may not appropriately stratify patients with severe deformities or lower pre-operative function. Additionally, in this study we did not consider deviations between scheduled start time and actual operative start time. This study also did not analyze other systemic factors, like anesthesia times and OR turnover times, which increase as the day progresses. Furthermore, this study was done at a single large academic medical center. This may limit the generalizability of our findings given every institution has an individual culture and protocol. Finally, this study does not provide insight into patient outcomes like LOS, PJI rates, or discharge disposition. Nonetheless, we believe this study serves as a promising starting point for future research which will even better elucidate the effects of operative start times on the quality of care for TJA patients.
Conclusion
Overall, this study has demonstrated that for TKA, patients surgical scheduling has little effect on operative length. For THA patients, non-first-start times are associated with slightly increased operative lengths of 9.1 to 11.8 minutes. For TKA patients, mid-day or evening start times are associated with mild operative length increases of 4.9 to 7.3 minutes. Understanding that surgical start time has minimal effects on operative lengths may better inform physician decisions and patient discussions when scheduling TJA.

Tables
Table 1: Patient demographics and operative characteristics stratified by start-time for TKA and THA patients. Significance measured using Chi-Squared Test
Table 2: Coefficient values for multi-variable linear regression model for both TKA and THA patients.