



Introduction
Total Knee Arthroplasty (TKA) is a commonly performed procedure primarily used to manage refractory, debilitating end-stage knee osteoarthritis. Over 700,000 TKAs are performed annually in the US, with the procedure presenting a significant resource burden (Carr et al. 2012; Sloan, Premkumar, and Sheth 2018). Key operative aims include pain relief, restoration of mobility and independence, and the attainment of functional knee flexion and Range of Motion (ROM) (Chiang et al. 2017). In addition to patient selection and surgical technique, these aims can be assisted by careful observation to identify complications early, rehabilitation to achieve milestones, regular contact with care providers, and patient motivation and compliance with postoperative orders.
Though an efficacious and safe procedure, several early postoperative complications may prevent these goals being realised, including surgical site infection and postoperative restricted flexion ROM (fROM). These may result in poor patient outcomes and dissatisfaction, as well as necessitate revision TKA (Chiang et al. 2017; Agarwal, Smuck, and Shah 2017). Given the association between early postoperative ROM and longer-term ROM, the rapid attainment of ROM and avoidance of complications are desirable goals (Chiang et al. 2017).
Remote patient monitoring may include technologies that enable the monitoring of patients outside of conventional clinical settings, such as in the home or remote areas, which may increase access to care and decrease travel and healthcare delivery costs. Wearable technology, in addition to telehealth, is a recent innovation applied to healthcare with the aim of providing continuous, objective and multi-modal health metrics, thereby improving patient and institutional outcomes. These technologies may allow for earlier and safer discharge from the hospital as well as the more pragmatic monitoring of patients in their actual daily activities (Dias and Paulo Silva Cunha 2018). This may allow for the increased and earlier detection of complications, allowing for timely intervention and better outcomes, as well as may provide motivation for patients. A number of promising early reports have emerged, particularly for postoperative monitoring (Amin et al. 2021).
Traditionally, post-TKA patients are monitored using a practitioner-dependent combination of periodic office assessments, self-reported questionnaires, goniometry for ROM, and functional tests such as the Timed Up and Go. However, these are problematic given their subjectivity, infrequency and poor correlation with actual daily activities performed by patients (Patterson et al. 2020; Small et al. 2019). Complications may also be detected at these follow ups, eventually raised by patients or on presentation to an emergency room depending on severity (Chiang et al. 2017; Ramkumar et al. 2019). The potential use of remote monitoring for post-TKA patients by reporting on novel methodologies and technologies as well as highlighting the feasibility of the technology, potential clinical utility, and positive stakeholder experiences have been described previously (Patterson et al. 2020; Small et al. 2019; Ramkumar et al. 2019; Mehta et al. 2020; Youn et al. 2018; Sharifi Renani et al. 2020; Youn et al. 2020; Bini et al. 2019). However, these studies have generally had small samples, pilot and/or non-pragmatic methodologies, and have not reported on the clinical utility of these technologies. The purpose of this prospective observational study was to assess the application of remote monitoring using wearable devices in the early post-TKA period by characterizing the overall progress and recovery kinetics of a cohort of 435 patients with multiple surgeons.

Material and methods
Study Design
This prospective multi-centre, multi-surgeon study was conducted to assess application of remote monitoring using wearable devices in the early post-TKA period. All patients were provided informed consent for participation via the consent screen on the wearable device Patient app (described later). Patients did not receive compensation for their participation. This study was reported using the STROBE Guidelines for cohort studies and IRB approval was attained through Northwestern Memorial Hospital and the University of Miami.
Study Population
All English-speaking adult patients (>21 years) scheduled to undergo elective unilateral primary TKA for end-stage osteoarthritis at participating institutions and treated by participating surgeons were deemed eligible for inclusion in the study. Exclusion criteria involved non-English speaking patients, patients undergoing bilateral or revision TKA, treatment for cancer as well a significant co-morbidity which may impact mobility including cardiorespiratory, gastrointestinal, haematological, and neurological pathologies.
Recruitment
Eligible patients were recruited from June 2018 to June 2021. Recruitment occurred through participating surgeons at their clinics. Potential subjects were informed on the pros and cons of participating in the study. The study aims were also provided to local physicians who were encouraged to refer suitable patients to the investigators for potential recruitment. All patients who agreed to participate in the study provided informed consent. All patients were informed that they could withdraw at any time with no compromise to the quality of their care. Patients were not compensated for their participation. Participating patients were contacted preoperatively by a representative from the wearable device company providing the equipment to educate them about how to use the equipment, including devices and phone application. Eligible patients agreeable to participation and did not have a suitable smartphone were provided one for the duration of the study.
Wearable Monitoring System
The TracPatch Duo Knee System (TracPatch Health; Sacramento, CA, USA) is composed of two wearable sensor units, each containing a 9 degree of freedom (DOF) inertial measurement unit (IMU) that incorporates 3 dimensions of linear acceleration, angular velocity, and magnetometry. One device is placed on the thigh of the affected leg, approximately 6-10 inches (15-25cm) above the affected knee joint line on the lateral side (Fig 1). The other device is placed on the shin of the affected leg, approximately 2-4 (5-10cm) inches below the tibial tuberosity on the lateral side. The devices are secured to the skin by means of a plastic carrying tray with fabric layer and medical grade adhesive. The tray is replaced approximately every two weeks, but the same location of the tray is confirmed by marking the skin with a marker using landmarks on the tray for consistent replacement of the carrier tray. Each night the devices are removed from the carrying tray and placed in a wireless charging tray.

The IMU on each device samples between 30-50 Hz. The data from the shin unit is transmitted to the thigh unit via Bluetooth Low Energy (BLE) and fused with data from the thigh unit to calculate knee angle in the sagittal plane. The maximum and minimum knee angle values (which represent the extreme values of flexion and extension, respectively) are calculated each minute and stored in the device’s flash memory. This is a passive process and will communicate the data to a handheld smart device (iOS or Android). A streaming mode is also used to provide real time feedback back for users to conduct a range of motion test (seated lift) and for conducting guided set and rep schemes for 6 exercises.
Data from the IMU sensors are also used to count the number of steps taken each minute by the individual wearing the devices. The devices store maximum and minimum knee angle values and step counts for each minute that the device is worn, and that data can be uploaded to the Patient mobile application via Bluetooth low energy, by selecting the sync data command in the application. Data from the application is immediately uploaded to a database hosted on a secure cloud server. The data is reported to the patient using a patient mobile application as well as to a healthcare provider mobile application and a web application. Additional features of the application are a series of surveys relevant to the to the TKA specialists, the ability to upload wound photos, the ability to rate their pain, and a HIPAA compliant telemedicine feature to allow the patient to communicate with their provider.

Study Methodology
All enrolled patients were preoperatively educated on the day-to-day use and upkeep of the remote monitoring system, including the skin-mounted monitors and the smartphone application by a company support representative. General instructions included wearing the monitoring system whenever awake and not showering, as well as answering the daily pain score questionnaire on the application and performing ROM tests and a series of exercises relevant to the TKA rehabilitation. The surgeons were additionally given access to and trained on the specific smartphone application designed for providers which allowed them to review their patient’s relevant data, including recent values and overall trends. All enrolled patients received postoperative monitoring, with the choice of preoperative monitoring and the durations of monitoring periods left to the discretion of the patient’s surgeon. Standard TKA procedures were performed by all surgeons. Patients did not engage the remote monitoring system on the day of surgery and resumed, or began, from the following day. Standard postoperative follow ups occurred according to the surgeon’s usual protocol.
Study Outcomes
The primary outcomes were flexion ROM (fROM) and Total Daily Step Count (TDS). Secondary outcomes were extension ROM, patient-reported pain scores as well as early postoperative Surgical Site Infections (SSIs) and restricted fROMs requiring Manipulation Under Anaesthesia (MUA).
Statistical Analysis
Patients with a minimum of two weeks of preoperative and six weeks of postoperative data (per parameter) were included in the statistical analysis. To define overall recovery progress and kinetics, de-identified raw patient data were converted to weekly averages, including mean TDS, mean maximal daily fROM, and mean minimum daily extension ROM (eROM). All values were reported as mean (SD), as appropriate.
To establish whether the devices were overall able to track the expected recovery kinetics with the established literature, paired samples t-tests were used to compare preoperative baseline values with postoperative 6-week values. The threshold for statistical significance was set at a p value of 0.05. All statistical analyses were performed using Excel (Microsoft). All graphing was performed using Python Pandas (Wes McKinney, Open Source) or Excel.
Results
Patient Demographics and Monitoring Data
A total of 435 patients were included in the study. The cohort had an average age of 66 ± 13 years and was 66% female. The average BMI was 29 ± 11. Operations to the right knee consisted of 57% of all surgeries. A total 6 surgeons performed all operations. The average monitoring duration was 2 weeks preoperatively and 6 weeks postoperatively. No wearable systems or sponsor-provided smartphones were damaged or lost during the investigation.
Remote Monitoring Data
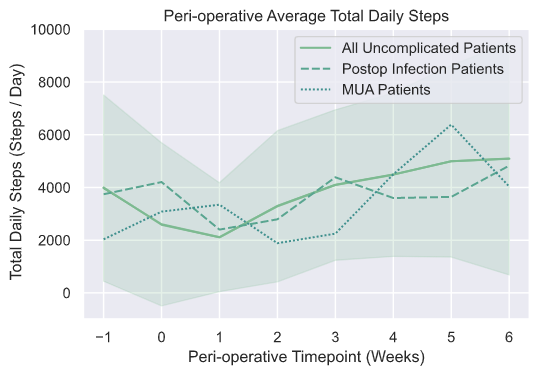
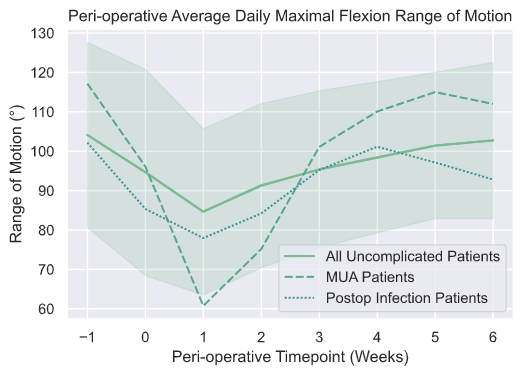
The primary wearable monitoring outcomes, fROM and TDS, generally improved over the defined study monitoring period (Table 1). Maximal daily fROM changed from a preoperative mean value of 104.1° ± 23.5° ° to a low of 84.6° ± 21.1° in postoperative week 2, before improving to 101.5° ± 18.6° at 6 weeks. TDS reduced from a preoperative mean value of 3976 ± 3532 steps per day to a low of 2112 ± 2066 in postoperative week 2, before improving to 4997 ± 3637 at 6 weeks postoperatively. TDS had the only significant difference with a higher step count relative to baseline.
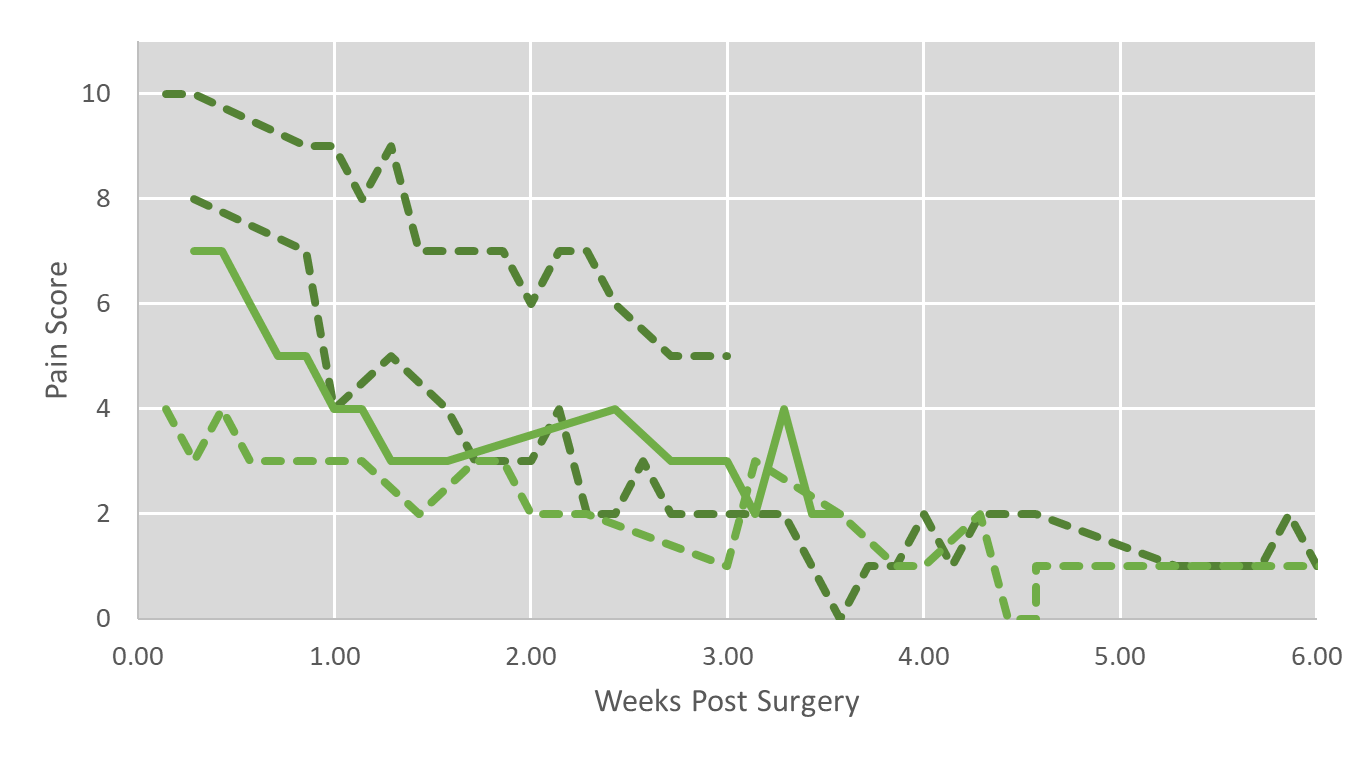
The secondary outcome of patient-reported pain scores was not reported in detail in this manuscript as the input screens on the patient app were changed during the study, based on patient feedback and overall useability, resulting in incompatible or incomplete data. However, various case samples are included (Fig 2) as representative of the data that is currently collected using the patient app.

Complications
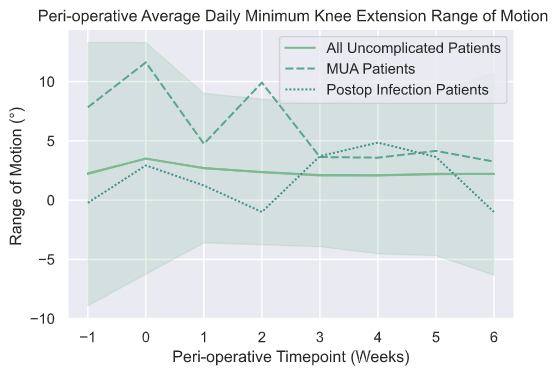
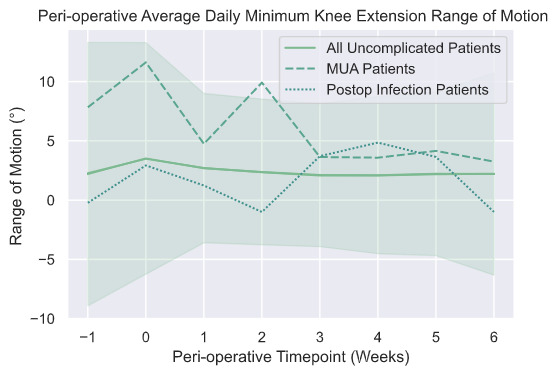
A total of 3 deep / prosthesis infections requiring surgical intervention occurred during the monitoring period. Infective complications were managed by the treating surgeons and associated medical team through a combination of antibiotics and revision surgery. A total of 4 patients had manipulation under aesthesia (MUA) during the monitoring period. All 4 patients continued to have favourable outcomes as demonstrated by their post-complication trend lines for primary outcomes and pain. The average data by metric for each cohort are reported by week along with 95th % confidence intervals are provided in Figs 3-5.


.jpeg)
Discussion
This study demonstrates the feasibility of using remote monitoring via periarticular wearable devices to monitor patients after TKA to assess overall progress and recovery kinetics using a large cohort of patients (n=435) from multiple surgeons (n=6) and institutions (n=4). The primary outcomes demonstrated both postoperative recovery (fROM and TDS) as well as surgically gained improvements over pre-operative function (TDS). Although the fROM at 6 weeks postoperatively was still marginally under the preoperative value (preoperative mean value of 104.1° ± 23.5° to 101.5° ± 18.6° at 6 weeks postoperatively), a significant difference from baseline was not observed. Chiang et al. report that knee ROM post-TKA almost returned to pre-surgical baseline by 6 weeks postoperatively, though considerable variation in the rate of improvement was apparent (Chiang et al. 2017). A fROM of 100° is generally seen as a functional and minimum satisfactory ROM, with failure to attain this being the most frequent post-TKA complication and a major cause of patient dissatisfaction.
Ramkumar et al. found that TDS, described as “mobility” in their study, returned to baseline within 6 weeks postoperatively (Ramkumar et al. 2019). In this study, TDS increased significantly over the preoperative level (preoperative mean value of 3976 ± 3532 steps/day to 4997 ± 3637 at 6 weeks postoperatively). The TDS improvements may be due to the protocol of this study where patients were able to perform daily exercises which are embedded within the patient application.
While many cohort studies using wearable monitoring postoperatively report incremental improvement to activity levels from baseline up to 1 year postoperatively, there is a lack of research demonstrating the different patterns of improvement and their clinical utility. As Small et al. discuss, a widely-accepted and well-evidenced target recovery curve is necessary, so that clinicians and patients have a reference and aid throughout the recovery and rehabilitation process (Small et al. 2019). The concept of monitoring day to day recovery using objective measuring tools has been discussed in the past using spinal interventions (Mobbs and Betteridge 2020), though this is a relevant concept for any intervention, including TKA as demonstrated with this dataset. In this manner, wearable technology may allow for a more objective and quantified demonstration of the attainment of surgical goals.
Patients anecdotally reported that the device was motivating and assisted with goal setting, rehabilitation assistance and a perceived enhanced connection with their treating surgeon, though a minority found the adhesives and device uncomfortable. Patient scoring through the end of care survey was high in the areas of patient satisfaction, patient compliance, patient motivation, and patient referral, however this will be subject to a future publication. Patients with sub-optimal outcomes were particularly less amenable to continued monitoring and participation in the study. This is in keeping with the findings of Ramkumar et al. regarding patients exhibiting poorer engagement with monitoring also demonstrated poorer outcomes, namely failing to achieve a fROM of 90° by 2 weeks (Ramkumar et al. 2019).
Limitations and Future Research
As a prospective proof-of-concept cohort study, the primary limitations include a lack of a control arm and the heterogenous monitoring durations for patients, as different surgeons preferred different monitoring time periods from 2 to 6 weeks postoperative. The study also had a low number of complications, which resulted in not being able to draw conclusions in differences in recovery relative to non-complicated patients. The postoperative monitoring period was also relatively short where continued improvements were expected beyond the 6 week time point. Ramkumar et al. demonstrated TDS exceeding baseline by 30% and a mean fROM of 119° by 3 months postoperatively, which is suggestive of considerable ongoing functional improvement (Ramkumar et al. 2019). Further research should focus on an acceptable and clinically relevant time period for objective patient monitoring.
It was reported in the methods sections that the devices continuously monitor leg position throughout the day when the patient is wearing the devices. This allows for the ability to understand the recovery kinetics of patients daily and not at defined timepoints in clinic or at the PT clinic. In future studies we will provide insights into the role of continuous monitoring for baselining and tracking recovery of patients following total knee arthroplasty. Such tracking measures could be useful for early identification of high risk patients for conditions such as arthrofibrosis.
Researchers should build on these findings with studies similarly conducted at a large scale and in a clinically relevant manner, ensuring a control arm, ideally randomised trials comparing remote monitoring with standard monitoring protocols, as well as a rigorously defined monitoring duration and protocol. Impact analysis, including of patient outcomes and institutional net costs (factoring in potentially earlier discharges and minimisation of the severity and progression of complications) should also be considered. The aims of such studies may also address how a combination of remote monitoring may supplement or be an adjunction for formal physical therapy and subsequent perioperative costs of care. Additionally, protocols will need to consider other variables such as complexities (ex: operative time) and operative plan (ex: cementation).
Conclusions
This study demonstrates the feasibility and prospect of clinical utility for remote monitoring of patients following Total Knee Arthroplasty using a large cohort of prospectively monitored patients. The data provided, range of motion and total daily step counts can be used by providers to set expectations for recovery following intervention. Further work is required to comprehensively investigate the effect of continuous monitoring with standard and/or hybrid measures for longer-term utility and the overall health and economic impacts.