



INTRODUCTION
The patella is the largest sesamoid bone in the body. It is embedded within two tendons – the quadriceps tendon proximally and the patellar tendon distally. The articular surface has a vertical ridge that splits the patella into a larger lateral facet and a smaller medial facet. The articular surface is the thickest in the human body, measuring approximately 5.5 mm. The patella plays an important role in the extensor mechanism of the knee by increasing the moment arm of the quadriceps by upwards of 30% (Gao et al. 2018). Patella fractures are relatively uncommon, accounting for just 1% of all fractures. Highly comminuted fractures are even more rare and are particularly challenging in regards to the surgical management and rehabilitation, with less predictable outcomes. Non-displaced and displaced fractures with less than 2 mm intra-articular step off and no disruption in the extensor mechanism are commonly managed non operatively. Surgical intervention is indicated in open fractures, those with significant treatable comminution, intra-articular displacement greater than 2 mm, and those with a disruption in extensor function of the knee (Kakazu and Archdeacon 2016).

Surgical techniques described in the literature include tension band wiring and suturing, lag screw fixation, cerclage, cannulated lag screw with tension band, low profile plating, partial patellectomy, and total patellectomy. Tension-band wiring and cancellous screws have been most commonly used for the management of transverse patellar fractures with several options in tension band wiring configuration and the material used (Singer, Halawa, and Adawy 2017).
Operative treatment of comminuted patellar fractures is much more complex and particularly challenging. Described surgical options are limited to cerclage and wiring, anterior plating with interfragmentary screw fixation, and partial and total patellectomy. Patellectomy leads to a compromised extensor mechanism and results in abnormal joint reaction forces, which ultimately affect the kinematics of the knee. It is a last resort when the comminution cannot be effectively treated (Dietz et al. 2009). Plate and screw fixation systems are used for transverse patellar fractures or inferior pole fractures (Thelen et al. 2012). Open reduction and internal fixation is the treatment of choice for comminuted patella fractures (Gardner et al. 2005). Cerclage wire fixation for comminuted patellar fracture results in relatively poor stability of the construct as it is not ideal for resisting the contraction of the quadriceps femoris or the tension caused by knee flexion. Comminuted fractures of the patellar often require two or more fixation techniques to achieve appropriate stability and maximize likelihood of bony union (Yang et al. 2018) . Fixation techniques such as anterior mesh plating result in prominent hardware that may be more prone to hardware irritation as well as wound breakdown.
In this case report, we present the first-reported rim plating technique as a novel, low-profile method for the surgical management of comminuted patellar fractures as well as a technique for neutralization of the patellar fixation constructs by spanning fixation to the patellar tendon.
SURGICAL INDICATION
A complex, severely comminuted distal third left patellar fracture

PREOPERATIVE PLANNING
Standard radiographic images of the patella fracture include anteroposterior and lateral views. A computerized tomography scan can be helpful in the determination of morphology of the fracture. Patient optimization, preoperative counseling and postoperative rehabilitation should also be discussed.
PREPARATION and PATIENT POSITIONING
General anesthesia with paralysis is preferred to maximize excursion on bony fragments. Well-padded supine position is used with sterile triangles or bumps available intraoperatively for variable knee flexion. The operative extremity is washed and then prepped and draped. A tourniquet is placed as proximal as possible to avoid entrapment of the quadriceps and is inflated to 275 mmHg.

SURGICAL TECHNIQUE
-
Approach
a. A midline skin incision centered over the patella extending from 1-2 cm above the proximal pole and distally to just proximal to the tibial tubercle.
b. Deep incision is then carried sharply to the level of the periosteum of the patella. At this point, the patella fracture is encountered. Hematoma and joint fluid is evacuated, taking care to preserve any loose bone fragments.
c. The fracture edges are carefully exposed, minimizing unnecessary periosteal dissection to maximize perfusion and keep soft tissue attachments to comminuted fragments.
d. The fracture site is carefully debrided of nonviable tissue and any small fragments that cannot be incorporated into the reduction are removed and saved for possible bone grafting.
-
Fracture Reduction
a. In the setting of extensive comminution, reduction clamps may further compromise the reduction. Thus, we use a modified Mason-Allen suture placed through the quadriceps and patellar tendons using a #5 EthibondTM (Cincinnati, OH) suture. The sutures are pulled towards each other to help achieve initial reduction.
b. Provisional K wires are placed out of plane to assist with holding the fixation and can also be used as joysticks for smaller fragments. The EthibondTM (Cincinnati, OH) suture is then temporarily tied together to act as a tension band between the tendons for added provisional fixation.
c. The fracture reduction is then inspected visually and confirmed with orthogonal fluoroscopy.
-
Initial Fixation
a. Two parallel K wires are passed from distal to proximal ensuring they are posterior to the midline of the patella on the sagittal view to prevent any posterior cortex displacement during knee flexion in the setting of a tension band construct. These screws are placed with minimal compression in the setting of comminuted fragments and are used primarily to add a tension band to the construct as well as a means for neutralization of the construct using a Krackow through the patellar tendon that will be described later.
b. A depth gauge is used to measure the screw length and the wires are overdrilled. Two 4-0 ArthrexTM cannulated screws (Naples, FL) are placed in a proximal to distal fashion with washers to maximize distribution of pressure. This is done one wire at a time to minimize risk of losing the reduction.
c. A 2-3 mm incision is made distally and proximally through the patellar and quadriceps tendons about the K-wires for direct access to bone at the level of the screws to avoid any soft tissue interposition for the Arthrex FiberTapeTM (Naples, FL)in order to minimize creep.
d. The Arthrex FiberTapeTM (Naples, FL) is passed through the screws in a figure-of-eight fashion. A 2-0 vicryl suture is passed through the fiber tape suture to shuttle with the fiber tape suture simultaneously. The vicryl sutures will be later used as passing sutures for a Krackow running through the patellar tendon to neutralize the construct. The FiberTape is then tied at the superior pole of the patella to minimize knot prominence, which may be more apparent at the inferior pole.
e. Repeat fluoroscopy is performed to evaluate reduction of the fracture with hardware placement.
-
Neutralization Krackow for Spanning Construct to Patellar Tendon
a. A Krackow suture using #2 fiber wire is passed through the patella tendon and the medial and lateral limbs of the suture are passed respectively through each of the cannulated screws that were placed in step 3B using the passing suture in step 3D. The #2 Fiberwire is then tied at the superior pole of the patella to help take tension off the primary fracture site and effectively neutralizing the construct.
-
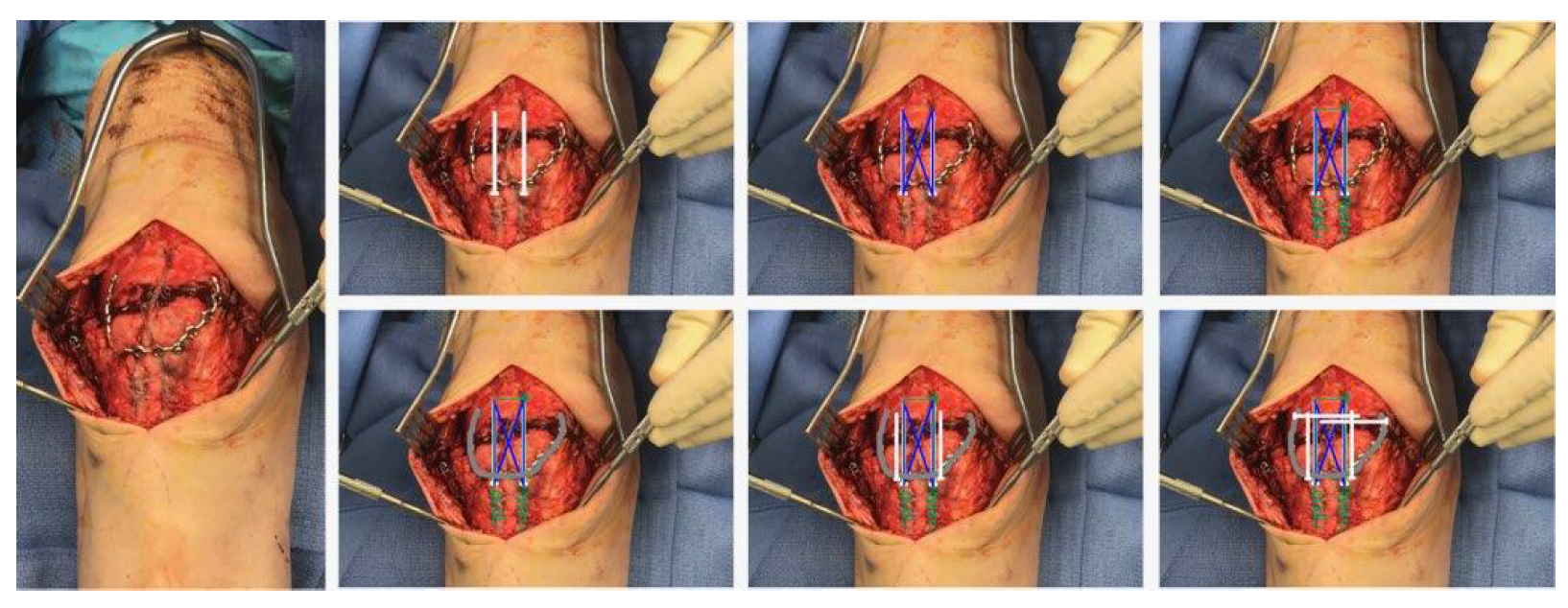
Patellar Rim Plating
a. A 2.4 mm 5x12 variable angle locking Synthes mesh plateTM (West Chester, PA) is cut in a U-fashion and contoured to fit around the rim of the patella as a “sling” to cradle the distal comminuted fragments, ensuring to bridge the fracture site to the proximal intact fragment. This plate can also be contoured circumferentially in the setting of a comminuted proximal fragment.
b. Once templated, the plate is applied to the patella and compressed around the rim, ensuring to place it as posteriorly as possible, but supraperiositeally to minimize any disruption to perfusion. The plate is placed around the rim rather than anteriorly as a mesh in order to minimize hardware prominence, especially in very thin patients with minimal anterior soft tissue coverage.
c. Two non-locking screws are drilled and placed in each bend of the U distally in a distal to proximal direction to compress the plate to the distal pole of the patella.
d. Proximally, the plate is wrapped around the patella supraperiosteally and compressed with a bone clamp.
e. Two locking screws, medial to lateral and lateral to medial, are placed at the proximal tip of the U plate, effectively creating a fixed-angle construct.
f. The ethibond sutures with the modified Mason-Allen suture that were previously placed are now removed.
g. Final orthogonal fluoroscopic images are obtained to assess fracture reduction and hardware placement.
h. The knee is ranged gently to 30-40o to ensure no gapping of the fracture site.
-
Any medial and lateral retinacular tears are closed with #2 high-strength suture.
-
The wound is copiously irrigated and closed in a layered fashion.

POSTOPERATIVE CARE
The patient is placed in a hinged knee brace locked in extension, allowing full weight-bearing while locked out. At two weeks post-operatively, supine flexion is permitted at 0 - 20°. This is increased weekly by 10-15° with physical therapy with a goal of 0-90° by 6-8 weeks post-operatively. Once adequate quadriceps control is noted, ambulation with the brace unlocked is allowed at 6-8 weeks. Strengthening is initiated upon radiographic evidence of fracture healing, at approximately 12 weeks post-operatively. 2-year follow-up radiographs are shown in Figure 3.

EXPECTED OUTCOMES
This technique was born out of a need for minimizing soft tissue irritation and hardware prominence in an elderly patient who was relatively cachectic and had minimal soft tissue anteriorly about his patella. Interestingly, he had a similar fracture a year prior on his contralateral side and was treated at an outside institution with partial patellectomy, resulting in residual pain, development of advanced osteoarthritis and prominent suture knots at the inferior pole of the residual patella that caused irritation and pain with any kneeling. He was interested in preserving his patella, but an anterior mesh plate would have put him at high risk for soft-tissue complications. The use of a contoured rim plate helps minimize hardware prominence and likely reduces the risk of hardware irritation and soft-tissue complications. Moreover, the fixed-angle construct of the plate, in combination with the neutralizing Krackow suture run through the patellar tendon and up through the cannulated screws is an extremely durable construct in the setting of a complex fracture that maximizes fixation while minimizing soft-tissue dissection and irritation.

COMPLICATIONS
Even though this method is less prominent, there is still a risk of hardware irritation. Positioning the plate as posterior as possible and ensuring appropriate contouring can help minimize this risk. Nonunion is also a risk, as is the case with any fracture surgery. Maximizing construct stability and minimizing modifiable perioperative risk factors by encouraging smoking cessation and diabetes control is critical to avoid nonunion. Stiffness in the setting of complex patellar fractures is a major concern and common problem. When a stable construct is able to be achieved despite extensive comminution, early range of motion can be initiated to minimize this risk.
Author Bios
Olusegun Onibonoje, DO, MSc is an orthopaedic surgery resident at Inspira Health Network, Vineland, NJ. He holds a first professional Physical Therapy degree from the University of Ibadan, Ibadan, Nigeria, an MSc in Orthopedics and Sports Physical Therapy from the University of Alberta, Edmonton, Canada and Doctor of Osteopathic Medicine degree from Campbell University School of Osteopathic Medicine, Lillington, NC.
Conflicts of Interest Statement for Dr. Onibonoje
Mark Ayzenberg, MD, FAAOS is a Board-Certified Orthopaedic Surgeon at Premier Orthopaedic Associates who specializes in Sports Medicine, Arthroscopy, and Reconstructive Surgery. His practice focuses on minimally invasive (arthroscopic “key- hole”) surgery of the shoulder, knee, hip, and ankle, as well as total joint replacements of the shoulder, knee and hip. He also treats general orthopaedic trauma, including dislocations and fractures.
Dr. Ayzenberg graduated cum laude with a Bachelor of Arts degree in Biology from the University of Pennsylvania in Philadelphia. He then completed medical school at the The Commonwealth Medical College in Scranton, PA as a Doctor of Medicine and graduated with highest honors, at the top of the class.
Dr. Ayzenberg trained at the prestigious Sports, Arthroscopy and Reconstructive Surgery fellowship at the Southern California Orthopedic Institute (SCOI). Prior to his fellowship, Ayzenberg completed his residency at the Einstein Healthcare Network in Philadelphia, where he served as Academic Chief Resident. He has an active
interest in advancing the field of Sports Orthopedic Surgery and has multiple scientific publications, several of which have been presented at national orthopaedic meetings.
Presently, Dr. Ayzenberg serves as the Assistant Team Physician for the Philadelphia Wings Professional lacrosse team.
Visit Dr. Ayzenberg’s Website
Connect with Dr. Ayzenberg on LinkedIn
Visit the Open Payments Data Page for Dr. Ayzenberg
Conflicts of Interest Statement for Dr. Ayzenberg