



INTRODUCTION
The first stemless humeral component for total shoulder arthroplasty (TSA) was introduced in Europe in 2004 (Churchill and Athwal 2016). However, it was not until 2015 that the first stemless implant was FDA approved for use in the United States (Maslow et al. 2019). A stemless humeral component provided a solution to some common problems associated with stemmed implants. Most notably, preservation of proximal humerus bone stock, intraoperative and post-operative fractures, and difficulty with removal during revision. The metaphyseal fit of the stemless implant eliminates the stress shielding seen with its stemmed counterpart and removal of stemless implants results in much less bone destruction (Churchill and Athwal 2016). Numerous studies have shown good short-term and mid-term results when comparing stemmed to stemless humeral components for TSA (Berth and Pap 2012; Churchill and Athwal 2016; Liu et al. 2020). The largest US based study to date with mid-term results has also shown favorable outcomes for stemless humeral implants in TSA for the treatment of glenohumeral arthritis comparable to those seen with stemmed implants (Churchill et al. 2016). With the first FDA approval for its use in the United States coming in 2015, stemless humeral implants are still a relatively new option for US based orthopedic surgeons. As such, mid-term data on clinical and radiographic outcomes for US based surgeons is limited and long-term outcomes are non-existent.
A major advantage of stemless humeral components is the ability to perform arthroplasty independent of the humeral shaft. Stemmed options are constrained by the ability to pass an intramedullary implant. This may be affected by deformity, congenital abnormalities, other implants, and a variety of other factors. Proximal humerus fractures are common orthopedic injuries representing about 81% of shoulder girdle injuries in patients over 65 years of age (Park et al. 2021). These are often managed non operatively with good outcomes. However, in the event of post-traumatic arthritis necessitating arthroplasty, deformity of the proximal humerus from a previous proximal humerus fracture creates considerable difficulty for the surgeon. The purpose of this case report is to demonstrate the use of a stemless humeral component in the setting of significant varus malunion of the proximal humerus for the treatment of severe glenohumeral joint arthritis. We highlight the ability to perform the desired procedure without the added morbidity of a proximal humerus osteotomy. Furthermore, we report mid-term clinical and radiographic outcomes for the stemless TSA at 6 years follow up.

CASE PRESENTATION
The patient is a 65 57 year-old right hand dominant female who initially presented to our office in 2014 at the age of 57. Her main complaint at that time was severe, progressive right shoulder pain refractory to non-surgical treatment. She reported significant functional limitations in both her home and work related activities as well as difficulty sleeping due to her pain. She was taking narcotic pain medications daily. She had failed extensive non-surgical management and presented for surgical consultation. Her history is most significant for an old right proximal humerus fracture treated nonoperatively that went on to heal in about 40 degrees of varus. This fracture was managed elsewhere and unfortunately, no further information regarding this injury is available. Past medical history is significant for hypertension, depression, and anxiety. She worked as an accountant. She was a former 1 pack per day smoker. and drinks alcohol occasionally. She did not take any blood thinning medications.
On examination, she was noted to be alert and oriented x3, and in no acute distress. The skin about her right shoulder was intact. She had limited range of motion of her right shoulder in all directions with associated severe pain and crepitus. There was tenderness to palpation diffusely about the shoulder with positive impingement signs. She was neurovascularly intact distally. Radiographs and CT scan of the right shoulder were performed revealing a healed proximal humerus fracture in about 40 degrees of varus malunion. Additionally, she was noted to have severe glenohumeral joint arthritis with subchondral cysts, a Walch B2 glenoid, degenerative changes of the acromioclavicular joint, and multiple intra-articular loose bodies.
A long discussion was had with the patient regarding her treatment options. She was severely symptomatic from her glenohumeral joint arthritis and had failed years of conservative treatment. We discussed the role for shoulder arthroplasty to address her pathology. Due to her severe varus malunion, a stemmed humeral prosthesis would not be possible without preceding osteotomy of her proximal humerus. We discussed the risks of osteotomy including additional surgical time, blood loss, chance of ongoing malunion or nonunion at the osteotomy site, and iatrogenic injury to critical neurovascular structures. At that time, stemless humeral prosthetics were being used in Europe and were showing good results. Unfortunately, in 2014 these implants were not FDA approved in the United States. Given her severe deformity, pain, and functional limitations, we felt that a stemless total shoulder arthroplasty would give her the best chance at having a good functional outcome with the least amount of risk. Aside from sparing her an osteotomy, we felt that a stemless implant would allow us to keep her cuff at the pre operative length and prevent stiffness that may have resulted from correcting the deformity and lengthening her cuff. We therefore proceeded to obtain a one-time use exemption from the FDA through their compassionate care program. The surgery was ultimately approved and on 12/19/15 the patient underwent a right total shoulder arthroplasty with a stemless humeral component and a trabecular titanium (TT) metal back modular glenoid.
After induction of general anesthesia, The procedure was started via a standard deltopectoral approach in a beach chair position. In addition to severe glenohumeral arthritis, She was noted to have a small full thickness rotator cuff tear in the critical zone in the anterior leading edge of the supraspinatus tendon which was mobilized and repaired to the greater tuberosity with heavy suture. The biceps tendon was noted to be severely diseased and was tenodesed in the groove and a large anterolateral acromial spur was removed using a rongeur and rasp. The humerus was then addressed. Osteophytes were removed and the head was removed using an osteotomy in the patient’s anatomic version as best as could be determined secondary to the malunion. A standard glenoid exposure was performed with a subscapularis tenotomy leaving a cuff of tissue on the lesser tuberosity for repair and tagging the medial tendon for retraction and identification at time of closure. Attention was turned toward the glenoid. After standard glenoid exposure, the center portion of the glenoid was determined. Secondary to the mild amount of posterior wear the glenoid was eccentrically reamed. The metal backed TT glenoid was placed with excellent fixation. Attention was turned back to the humerus. The metaphyseal bone of the proximal humerus was noted to be of good quality. The stemless total shoulder arthroplasty was then implanted in accordance with the Lima technique guide. Trial implants were placed, the shoulder was reduced, and it was noted to be stable in all directions with excellent range of motion. Final implants were inserted. Wounds were irrigated and subscapularis was repaired to the lesser tuberosity using #2 TiCron. The deltopectoral interval was closed with heavy suture. Subcutaneous layer was closed with 2-0 Vicryl and skin was closed with staples.
The patient was placed in a sling post operatively and discharged uneventfully on post op day #1. She was seen in the office on 12/31/15. Her pain was well controlled, her surgical wound was healing well, and she had excellent passive shoulder range of motion. Staples were removed and she was given a prescription for physical therapy. She was seen back at 2 weeks, 6 weeks, 3 months, and 6 months post operatively. She improved significantly at each visit. She did not return for her 1 year appointment but did come back to the office in 2018 for evaluation of her left shoulder. She was most recently seen in December of 2021 for the left shoulder. The right shoulder has been doing excellent and she has no complaints regarding the right shoulder at her most recent visit.
Her post operative restrictions included sling for the first two weeks. At two weeks post op she was allowed to perform passive range of motion, except limited external rotation to 0-20° for the next 4 weeks. At 4 weeks post op she started active assisted range of motion in the supine position with gradual progression to upright. Isometric deltoid and periscapular strengthening started 3 months postop.
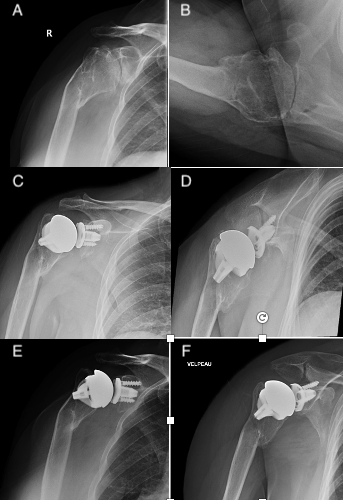
Functional outcomes were evaluated with the American Shoulder and Elbow Surgeons (ASES) score and the visual analog scale (VAS). Preoperative ASES and VAS scores for her right shoulder were 45/100 and 5/10 respectively. At six year follow up in December of 2021 her ASES and VAS scores were 98/100 and 0/10 respectively. Figure 1 shows the comparison between her pre op, 6 week post op, and 6 year post op x-rays of her right shoulder. Pre-operative range of motion was noted to be limited i all directions with forward elevation and abduction to 140°, external rotation to 30°, and internal rotation to her posterior buttocks. Post operative range of motion at six years is shown in Figure 2 with forward elevation to 180°, abduction to 160°, external rotation to 60° and internal rotation to her thoracolumbar junction.
__6_weeks_post_op_(c_d)__and_6_years_post_op_(e_f)_radiographs_of_right_shoulde.png)

DISCUSSION
This case report highlights the benefit of a stemless total shoulder implant with a metal backed glenoid for the management of glenohumeral arthritis in the setting of a proximal humerus deformity that would preclude the passage of an intramedullary humeral stem. A proximal humerus osteotomy would certainly have been an option to allow for a stemmed implant but this creates additional concerns including more implants with potential need for removal, blood loss, nerve/vessel injury, increased surgical time, and the need to heal the osteotomy. Furthermore, Boileau et al. described worse functional outcomes in patients having a total shoulder arthroplasty that required an osteotomy when compared with those that did not require an osteotomy (Boileau et al. 2001). While osteotomy was discussed with the patient, we felt the risks associated with this procedure were unacceptable when compared with a stemless implant despite the lack of FDA approval. As a result, we were able to obtain FDA approval for a one time use of a stemless humeral implant under their compassionate care program.
Although the stemless shoulder design has been approved in Europe since 2004, FDA approval in the United States did not come until 2015. As a result, there is limited US data on mid-term outcomes and even less when used in the setting of proximal humerus deformity. Overall, the data has shown comparable functional outcomes between stemmed and stemless systems for the management of glenohumeral arthritis (Berth and Pap 2012; Churchill and Athwal 2016; Liu et al. 2020). Ballas et al. present short term outcomes for stemless shoulder arthroplasty in the setting of proximal humerus malunion and highlight the ability of the implant to avoid osteotomy while allowing for good functional outcomes (Ballas, Teissier, and Teissier 2016).
A case report from Johns Hopkins by Park et al. demonstrates a similar case to our patient with functional and radiographic outcomes at 2.5 years (Park et al. 2021). Their patient had a malunion from a conservatively managed proximal humerus fracture and went on to develop post-traumatic arthritis of her glenohumeral joint. She subsequently had a stemless TSA. Her ASES score improved from 45 preop to 97 and VAS improved from 7 to 0 at 2.5 years. This is in line with our results which showed improvement in ASES from 45 to 98 and VAS from 5 to 0 at six years.
While our patient experienced excellent results, the obvious weakness of this study is the case-based nature of it. Unfortunately, the combination of recent FDA approval and the relative rarity of having to perform a TSA in the setting of significant proximal humerus deformity makes it difficult to have a large number of patients.
This case report presents radiographs and functional outcomes at six years following a total shoulder arthroplasty using a stemless humeral implant for varus malunion of the proximal humerus. Our patient has maintained excellent range of motion with ASES and VAS scores of 98 and 0 respectively at 6 years follow up. We present this case as one of the only US based reports to show mid-term follow up for a stemless humeral implant in the setting of a proximal humerus malunion.

CONCLUSION
Current literature suggests that patients achieve similar clinical outcomes when undergoing total shoulder arthroplasty using either a stemmed or stemless humeral implant. Our case report supports the use of a stemless implant in the setting of a proximal humerus deformity with excellent radiographic and functional outcomes at six year follow up.