

INTRODUCTION
In the United States, it is estimated that 30-45 million youth ages 6 to 18 years participate in some form of organized or recreational athletics (Brenner and American Academy of Pediatrics Council on Sports Medicine and Fitness 2007; McGuine 2006). The steady increase in youth sports participation has also produced an increase in youth sport specialization, year-round intensive training in a single sport at the exclusion of other sports (Wiersma 2000). Coaches and/or parents frequently encourage young athletes to focus on a single sport as early as middle school, often unaware of the potential risks this poses (Johnson 2008). Several studies and national organizations such as the American Academy of Pediatrics (AAP) council on sports medicine and fitness, have cautioned against early sport specialization, citing an increased risk of injury and burnout (Bell et al. 2016; Jayanthi et al. 2015; Swenson et al. 2013).
The Centers for Disease Control and Prevention (CDC) reported that injuries from organized and unorganized sports account for 775,000 annual emergency room visits for children ages 5-14 (National Council of Youth Sports, n.d.). Among children ages 12-17, sports related injuries, including overuse injuries, are the leading cause of emergency room visits (National Council of Youth Sports, n.d.). Several studies investigating acute and overuse injuries within the context of single sport training and sport specialization focus primarily on male athletes or group data on male and female athletes (Myer et al. 2015; Post et al. 2017). This approach fails to consider that certain injuries are more prevalent in female athletes like ACL injuries which occur 3-8 times more frequently in females compared to males (Arendt and Dick 1995). Additionally, female athletes have higher rates of knee injuries overall, including a higher incidence of early-onset degenerative changes (Silvers and Mandelbaum 2007; Murphy, Connolly, and Beynnon 2003; Gillquist and Messner 1999; Lohmander et al. 2004). When discussing sex-specific concerns among female athletes, it is also necessary to consider the female athlete triad: low energy availability with or without disordered eating, menstrual dysfunction, and low bone density (Nattiv and Lynch 1994). Given that the incidence of some injuries may be increased among females that train exclusively in one sport, it is possible that occurrence of one or more components of the female athlete triad is also increased in this specific population.
The primary aim of this study was to determine if there was an association between training exclusively in one sport and injury prevalence in adolescent female athletes. A secondary aim was to determine the most common anatomic locations of injuries within single and multi-sport athletes. Additionally, we sought to identify possible factors that may have contributed to injuries, and determine what role, if any, that intensive training in a single sport may have on menstrual functioning, bone density and body image. We hypothesized that female athletes who selectively trained in a single sport would have higher prevalence of sport-related injury, menstrual dysfunction, and negative body image.

METHODS
Study Design & Setting
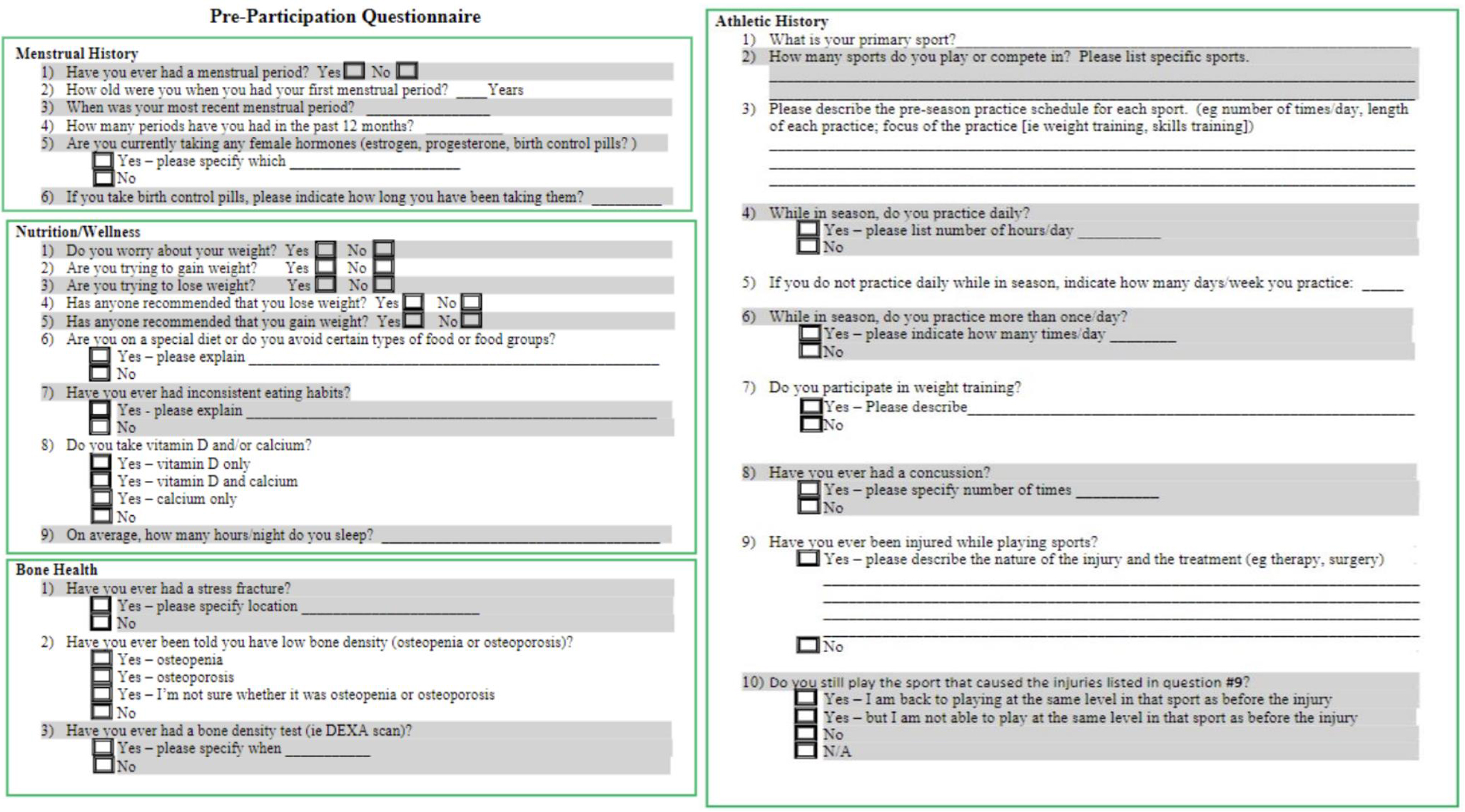
Pre-participation questionnaires were created by the senior author, the team physician for several local all-girls high schools. The original purpose of the questionnaire was to gather general information on the athletes and data was analyzed retrospectively [IRB 2018-528]. The pre-participation questionnaires were distributed in person to all female athletes from five local high schools participating in school required pre-sport physicals between June 2017 to August 2017. Participants were 13-18 years of age. A copy of the questionnaire has been provided in Figure 1.

Approximately 640 female athletes completed the questionnaire [IRB 2018-528]. Athletes that did not indicate whether they were a single or multisport athlete were excluded from the statistical analyses, leaving a total of 611 athletes who were included in this study. Athletes that reported participation in just one sport, regardless of the amount of time spent playing that sport during the year, were classified as single sport (SS) athletes. Those that participated in multiple sports (MS) were asked to designate one sport as their primary sport and others as secondary sports.
Statistical methods
Data was summarized as frequencies and proportions (%) and means ± standard deviations. Odds ratios (OR) and 95% confidence intervals (CI) were calculated to investigate the association between specialization and sport-related injuries, irregular menses, stress fractures, and body image concerns (a priori p ≤0.05). Frequencies, proportions, means, standard deviation, effect size (d) analyses were determined using Microsoft Excel, version 2016 (Redmond, WA). Odds ratios, comparison of means via t-test and 95% CI analyses were calculated using MedCalc statistical software (v 18.2.1) (Ostend, Belgium).

RESULTS
Single Sport vs. Multi-Sport
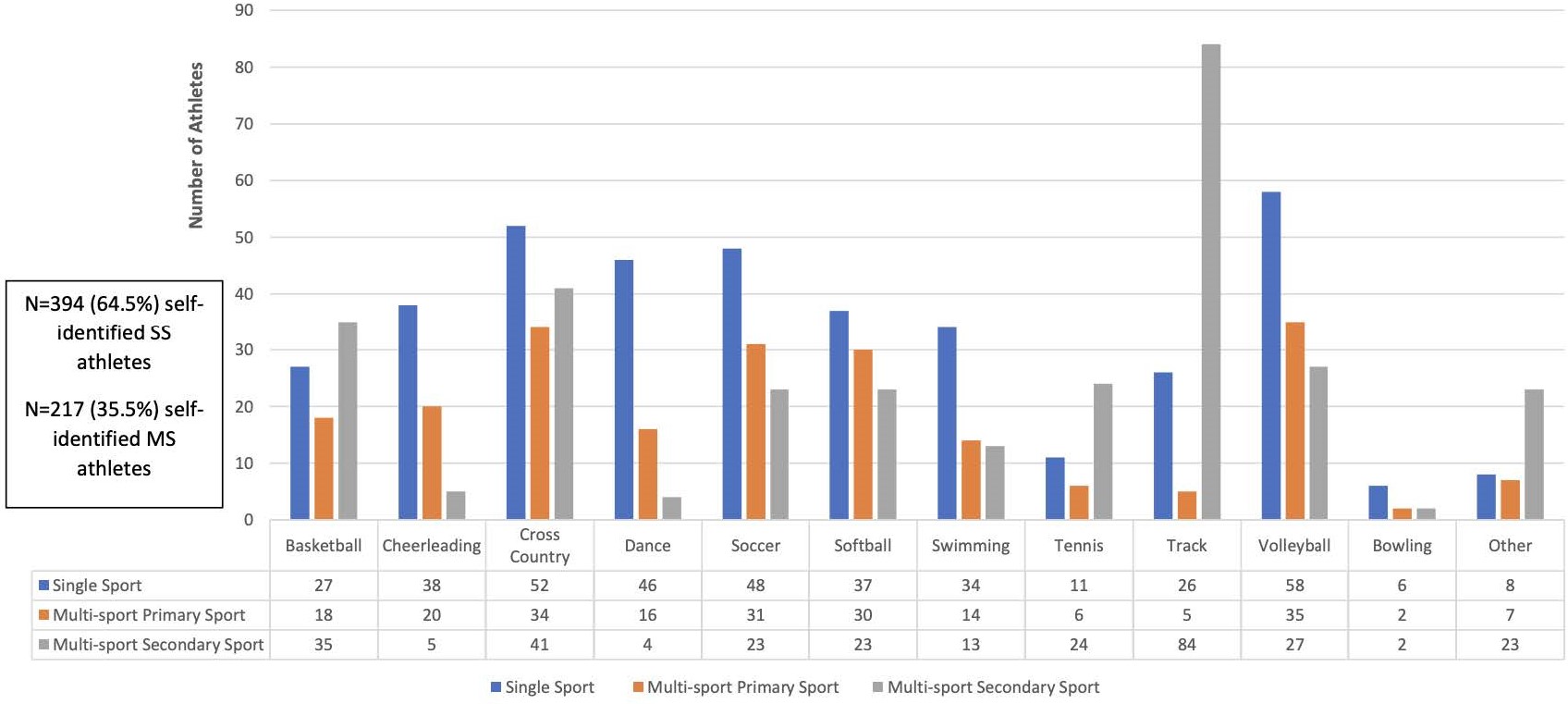
A total of 611 female athletes, ages 13-18 completed the questionnaires distributed prior to their sports physical. 394 of 611 (64.5%) participants reported participating in only one sport (SS), while 217 (35.5%) participated in multiple sports (MS). Among SS athletes, volleyball (58, 14.8%) and cross-country (52, 13.3%) had the greatest number of participants (Figure 1). Volleyball (35, 16.1%) and cross-country (34, 15.7%) were also the most frequently reported primary sports among MS athletes. Track and field (84, 38.2%) and cross-country (41, 17.1%) were the most common secondary sports among the MS group (Figure 2).

SS athletes were less likely to have daily practice compared to MS athletes (p <0.01; OR,0.55; 95% CI, 0.39-0.78). Though a greater proportion of MS athletes reported practicing daily, SS athletes that practiced daily had significantly longer practice hours than their MS counterparts who were also practicing daily (1.94 ± 0.54 vs 1.80 ± 0.51, p=0.01, d=0.27). When comparing athletes who did not practice daily, there was no significant difference in the number of practice days between SS and MS athletes (3.09 ± 1.05 days vs 3.29 ± 0.90 days; p=0.17, d=0.20).
Athletes that trained in only one sport did not have higher rates of injury compared to their MS counterparts (p=0.48; OR,0.88; 95% CI, 0.62-1.25). Of the 394 SS athletes, 132 (33.5%) reported a history of 178 total injuries while playing their respective sport, while 79 of the 217 MS athletes (36.4%) reported a total of 102 injuries. Several different injuries were reported, including stress fractures, ACL tears, patellar tendonitis, fractures, and sprains. The most common injuries were to the ankle, hand, knee, and shoulder (Table 1).
Anatomical Locations and Injuries
When reported injuries were grouped by anatomical body part, ankle injuries were the most common injury type reported within both groups. Among injured SS athletes, 36 (27.3%) reported a history of at least one ankle injury, compared to 28 (35.4%) injured MS athletes. Knee injuries were the second most common injury reported for each group, with 27 (20.5%) injured SS athletes and 16 (20.3%) injured MS athletes reporting at least one knee injury. Playing only one sport was not associated with increased risk of ankle injury (p=0.21; OR,0.68 95% CI, 0.38-1.24) or knee injury (p=0.97; OR, 1.01; 95% CI, 0.51-2.02). Additionally, SS athletes were less likely to have a history of stress fracture than MS athletes (p=0.03; OR, 0.50; 95% CI, 0.27-0.92).
Soccer and volleyball players made up the largest proportion of injured SS athletes, with each sport having 26 (19.7%) injured athletes (Table 2). There were 26 (54.2%) SS soccer players and 26 (44.8%) SS volleyball players that reported a history of at least one injury. MS athletes who indicated that cross-country and volleyball were their primary sport, made up the largest proportion of injured MS athletes (15 each, 19.0%). Within those groups, 15 (44.1%) MS cross-country athletes and 15 (42.9%) MS volleyball players reported a history of injury. Among injured MS athletes, those that participated in track and field as one of their secondary sports accounted for the greatest proportion of injured MS athletes, 36 (45.6%). Compared to injured SS athletes, injured MS athletes were more likely to be track runners (p < 0.01; OR,8.81; 95% CI, 4.20-18.46).
Menstrual Dysfunction
There was a significant decrease in the number of menstrual cycles within the last 12 months among SS athletes compared to their MS counterparts (11.1 ± 2.1 cycles vs 11.7 ± 1.3 cycles, p=0.02, d=0.34). Although this result was statistically significant, given the small difference in the length of menstrual cycles, this finding is likely not clinically significant. There was no difference in the proportion of SS and MS athletes who reported worrying about their weight, 82 athletes (21.1%) vs 43 athletes (20.5%), respectively. However, SS athletes were more likely to report trying to lose weight (p=0.01; OR, 1.65; 95% CI, 1.11-2.47).
A comparison was also performed between athletes playing sports that were more likely to be diagnosed with the female athlete triad. For this study, the sports that fit this classification were cheerleading, cross country, dance, swimming, and track. Of these sports, SS athletes from dance (14), track (12), and swimming (8), had the most injuries when compared to their multi-sport counterparts with 2, 1 and 3 injuries respectively. The injury rates between SS and MS athletes from cheerleading (9 SS and 11 MS) and cross country (15 SS and 15 MS) were not statistically significant. When doing an analysis between single sport track and single sport cross country, there was a higher percentage of SS cross country athletes (11.4%) who suffered from injuries than SS track (9.1%).
DISCUSSION
Despite previous reports that selectively training in one sport leads to increased injury rates among specialized athletes, our data shows that participating exclusively in one sport is not associated with a higher risk of injury in female high school athletes. Athletes that play one sport and those that play multiple sports do report different practice schedules and time spent per practice. Additionally, it is possible that the number of sports played may affect other outcomes, such as menstrual health, risk of stress fracture, and body image.
Previous studies have demonstrated that more female athletes self-classify as SS athletes compared to their male counterparts (Bell et al. 2016; Strand 2006; Buckley et al. 2017). However, few primary research studies have focused on female athletes that choose to compete exclusively in one sport. Though prior studies have reported that exclusive participation in a single sport can cause higher injury rates among athletes, our study found higher injury rates among athletes that played multiple sports (Beese et al. 2015; Hall et al. 2015; Kristiansen and Stensrud 2017). However, some conclusions made by prior single sport specialization studies did hold true among this population of female athletes.
Female athletes have previously been reported to have high rates of lower extremity injuries including patellofemoral pain, patellar tendinopathy, and ACL injuries which occur 3-8 times more frequently in female athletes (Arendt and Dick 1995; Silvers and Mandelbaum 2007; Beese et al. 2015; Padua et al. 2009). Similarly, this study found that lower extremity injuries made up a large percentage of injuries reported by both SS and MS athletes. Additionally, the high rates of knee injuries in both SS and MS athletes is in accordance with previous reports that female athletes have a high risk for knee injuries regardless of the number of sports they play (Beese et al. 2015). Female athletes who specialize in a single sport reportedly have a high risk of patellofemoral pain, Sinding Larsen Johansson/patellar tendinopathy, and Osgood Schlatter Disease (Hall et al. 2015). One athlete in our study, a SS athlete, specified being diagnosed with patellofemoral pain syndrome. The questionnaire did not ask participants for a specific diagnosis when describing their injuries. Therefore, it is possible that more athletes had patellofemoral pain, patellar tendinopathy, or Osgood Schlatter Disease and those specific diagnoses may be associated with continuously training in a single sport. Higher rates of lower extremity and knee injuries among females has been reported to be due to biomechanical factors such as decreased flexion of the knee, hip and trunk, increased knee valgus and tibial rotation (Arendt and Dick 1995; Beese et al. 2015; Padua et al. 2009). These biomechanical factors may hold true regardless of the number of sports a female athlete plays.
It is possible that more significance should be given to the types of sports female athletes choose to combine. The finding that injured MS athletes were more likely to be track and field runners suggests the number of sports and the number of hours played may not in itself inherently increase a female athlete’s risk of sustaining an athletic injury. Instead, the addition of track to a female athlete’s self-selected primary sport may put them more at risk for injury. Further research should explore the combination of sports that may be associated with higher risk of injury among female athletes. More specifically, further research should examine the possible association between having track & field as a secondary sport and increased risk of injury in female athletes.
Conditioning programs that focus on reducing neuromuscular deficits can reduce sports-related injuries in male and female adolescent athletes.{Dalton, 1992, Overuse injuries in adolescent athletes} (Dalton 1992; LaBella et al. 2008; Myer et al. 2011; Alentorn-Geli et al. 2013) These programs should incorporate exercises that reduce quadriceps muscle imbalance, which can lead to patellofemoral pain and increased musculoskeletal stress. Preseason and in-season injury prevention programs consisting of neuromuscular conditioning, plyometrics, and agility training are particularly effective in female athletes (Silvers and Mandelbaum 2007; LaBella et al. 2008; Renstrom et al. 2008; Mandelbaum et al. 2005; Grindstaff et al. 2006). Considering that both SS and MS athletes reported high rates of lower extremity injuries, injury prevention training recommendations may need to better target all female athletes, as they show high rates of lower extremity injury regardless of whether they play a single sport or multiple sports.
This study found that athletes participating in a single sport have more negative outcomes such as decreased number of menstrual cycles, higher proportions of stress fractures, and increased concern about their weight; a conclusion consistent with past data showing high rates of stress fracture susceptibility and menstrual dysfunction in female athletes (Prather et al. 2016). Previous studies have also shown an association between intensive training leading to low energy availability and the development of the female athlete triad (Stanton et al. 2002; Otis et al. 1997). It is now understood that the three components of the triad exist on a spectrum from optimal health to disease, seen as menstrual dysfunction, low energy with disordered eating, and low bone mineral density leading to increased rates of stress fractures (Nur, Romano, and Siqueira 2007; Nattiv, Loucks, Manore, et al. 2007). It is estimated that up to 16% of all female high school athletes have all three components of the triad, while up to 54% have at least one component (Hoch et al. 2009; Nichols et al. 2006; Barrack, Ackerman, and Gibbs 2013; Fredericson and Kent 2005; Gibbs, Williams, and De Souza 2013). Considering the number of SS and MS athletes who reported concerns regarding their weight, menstrual cycle irregularity, and history of stress fractures, it is important that physicians, coaches, and parents be prepared to intervene if any signs of the triad are identified. It is also necessary to further explore the prevalence of female athlete triad components within certain sports, as some sports may put female athletes at an increased risk of disordered eating, menstrual irregularity, and low bone density.
Limitations
There are several limitations to this study. Given the retrospective nature of this review, we were limited by the questions asked in the questionnaire. The questionnaire did not ask athletes to indicate the number of months per year they spent playing each sport. For that reason, single sport athletes could not be deemed truly “specialized” as the amount of time they dedicated to their single sport during the year was unknown. The 3-point specialization classification system proposed by Jayanthi et al. is now widely regarded as an improved measurement of specialization, as it classifies athletes as being either low, medium, or highly specialized (Jayanthi et al. 2015). The single/specialized vs. multi-sport classification, a method of classification that was frequently used before the 3-point system, does not account for athletes that consider their sport participation as more casual and only sporadically play a single sport (Jayanthi et al. 2015; Hall et al. 2015). Further research applying the 3-point specialization scale, which accounts for different levels of competition, to female athletes may prove useful in identifying additional injury risk among female athletes. Second, as the questionnaire did not require that athletes provide a timeframe for their injuries, it is unclear when the injuries occurred. Third, patients in this study were asked to recall injuries, practice hours, and a variety of other information that created the opportunity for recall bias. The questionnaires were not reviewed with subjects after completion, thereby creating the possibility of inaccurate or incomplete information. This is an inherent limitation of retrospective reviews. Fourth, given the study population, we did not incorporate a question asking subjects to specifically identify if their injury was an acute or overuse injury. Fifth, we did not use a validated instrument to assess body image. Sixth, this study only evaluated female athletes in a specific geographic location (i.e. the South) and hence, results may not be generalizable to the rest of the country.
PRACTICAL APPLICATIONS
This study demonstrated that female athletes who chose to exclusively play a single sport did not have higher rates of injuries compared to female athletes that played multiple sports. Further research on injury patterns among female athletes using various specialization classifications is necessary to determine the risk of injury associated with sport specialization in adolescent female athletes. Additional research focused on potential associations between the type of sport and associated injury patterns is also necessary.