


INTRODUCTION
Elbow arthroscopy has been in existence for decades (Chen et al. 2017). With the advent of ever-improving technology, elbow arthroscopy should become technically easier to perform, and the indications broadened. However, there has been surprisingly little innovation in the elbow positioning marketplace in the last several decades. Surgical procedural inefficiency and variability in operative time for orthopaedic surgical procedures have been highlighted in the literature recently (DeCook and Statton 2022; Milone et al. 2019). Early in my career, I performed elbow arthroscopy with patients in the lateral decubitus, prone, and even supine suspended positions. Over a decade ago, procedural time inefficiency, along with the disadvantages that accompany each of these positioning techniques, led me to change to a supine positioning technique that stabilizes the humerus vertically while leaving the forearm free for all elbow arthroscopy procedures.
I refer to this technique as supine elbow arthroscopy (SEA) in order to differentiate it from supine suspended elbow arthroscopy (SSEA), in which a mechanical traction device captures the forearm and complicates intraoperative arm manipulation and positioning to various degrees.
This paper provides an analysis of the data from 298 fully arthroscopic surgical procedures performed using this SEA technique, along with a discussion of other current positioning techniques and the future of patient positioning for elbow arthroscopy.

METHODS
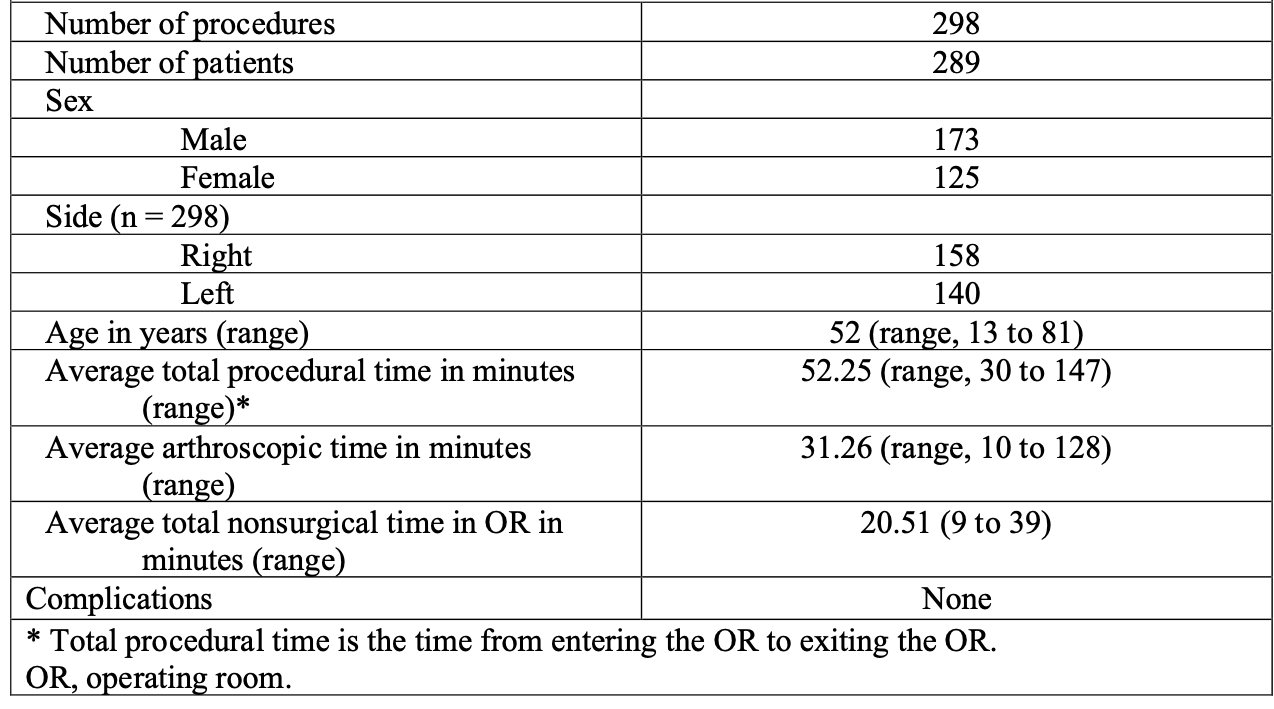
This was a retrospective review of arthroscopic elbow surgeries performed in the SEA position between 2011 and 2021. All surgeries were performed by the author at one multi-specialty surgical center. The physician’s private practice database, along with the surgery center’s patient database, were searched and reviewed to identify fully arthroscopic surgical procedures using current procedural terminology (CPT) billing codes. The CPT codes included in the search were the elbow arthroscopy codes 29830 through 29838. Only procedures that were performed fully arthroscopically were included in the study and reviewed. Surgical procedures that included arthroscopic CPT codes, along with any open procedural CPT codes, underwent additional operative note review and were excluded from this analysis if any component of the procedure was converted to “open.” Facility and physician medical record data were then reviewed for all relevant patient cases and analyzed. All procedural time data points were determined and recorded by the operating room (OR) circulating nurse in charge of the procedure along with the anesthesiologist and entered into the patients’ medical records at the point of care. The purpose of this study was to analyze procedural times (in-room to out-of-room), arthroscopic surgical times, International Classification of Disease (ICD-9 and ICD-10) diagnosis codes, CPT codes, as well as any patient complications. The goal was to analyze the efficiency, safety, and versatility of elbow arthroscopy performed in the supine position with the forearm free (SEA). The demographic data of this review are summarized in Table 1.
.png)
Surgical Technique
All surgical procedures were performed with the patient in the supine position under general anesthetic. Regional blocks, when administered, were performed in the preoperative holding area. A pneumatic tourniquet typically was applied to the upper arm when not contraindicated (dialysis shunt presence, etc.).
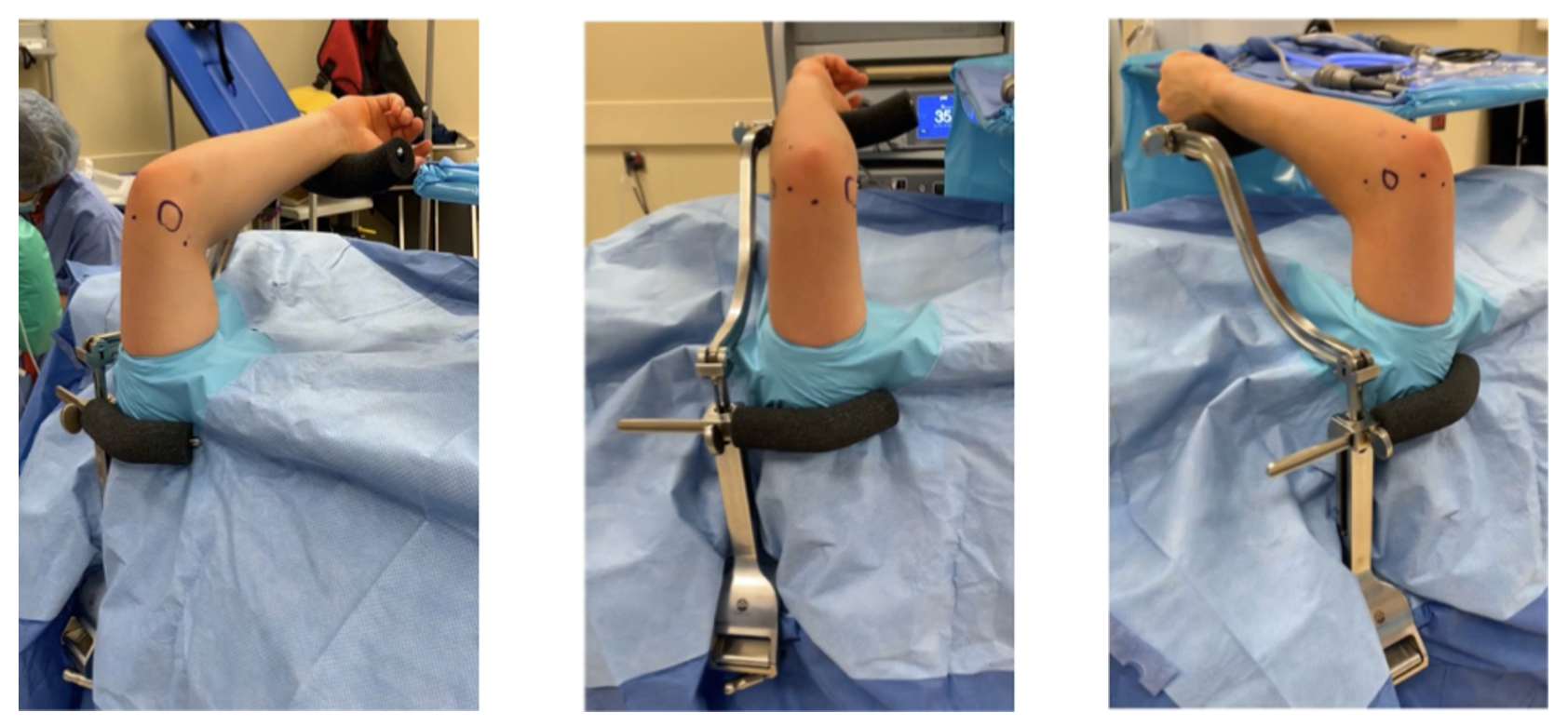
The upper extremity was prepared in a sterile manner, and a sterile arm positioner (ElbowLOC® Supine Positioner Assembly, Hunter Medical, LLC, Columbia, TN) was secured to the operative table railing over sterile drapes. The humerus was thus stabilized vertically, perpendicular to the floor, and the distal forearm was supported at the desired elbow position by the supine positioner component of the assembly. The humerus remained fixed in this perpendicular vertical position throughout the procedure. The forearm was left free to allow unrestricted forearm rotation and dynamic elbow motion (Figures 1A through C).
__posterior_(b)__and_lateral_(c)_views_of_supine_elbow_arthroscopy_(sea).png)
The elbow joint was distended with saline injected though the “soft-spot” area. A standard anteromedial portal was established first, then an anterolateral portal established with the assistance of a spinal needle to ensure ideal positioning. Additional anterior compartment working portals were established as needed. For posterior compartment arthroscopy, the height of the supine positioner component was adjusted by the surgeon as necessary to place the elbow in the desired degree of extension in order to relax the posterior capsule. A soft-spot portal was established along with posterior midline portals and posterolateral portals as needed. Static elbow extension was “dialed in” as needed during the procedure by the surgeon adjusting the height of the supine positioner component. Static elbow flexion was controlled likewise, with maximum hyperflexion achieved by resting the patient’s wrist on the chest. With the humerus stabilized vertically and the forearm free, the surgeon could easily manipulate the elbow into any desired position dynamically throughout the procedure. At the end of the procedure, the arm positioner device was removed, followed by the sterile drapes.
A surgical assistant was used occasionally during these SEA procedures. In these instances, the assistant’s task was to help with additional retractors or other surgical tools, not to hold the patient’s humerus or forearm in a certain static position, as that task was achieved by the positioner device.
RESULTS
Analysis of the surgery center and physician practice data revealed 298 relevant arthroscopic surgical procedures performed on 289 patients between 2011 and 2021. The demographic data are summarized in Table 1. Diagnoses for these surgical procedures, both preoperative and postoperative, are displayed in Supplemental Appendix 1 and cover the spectrum of elbow injuries including traumatic and degenerative conditions.
Notable findings include total procedural times (in-room to out-of-room) averaging 52.2 minutes and arthroscopic (surgical) time averaging 31.2 minutes. These data show that on average 20.5 minutes of the total in-OR procedural time of these cases were dedicated to nonsurgical patient care. Included in this time is anesthesia administration, patient positioning, sterile preparation of the operative extremity, awakening the patient from anesthesia, and patient preparations for the post-anesthetic care unit. No effort was made to carve out miscellaneous outlier reasons for delays. A review of operative notes and medical records revealed no evidence of complications. Specifically, no nerve palsies, unplanned returns to the operating room, arthrofibroses, complex regional pain syndrome, infections requiring an antibiotic prescription, or other complications were identified.
DISCUSSION
Elbow arthroscopy positioning techniques have changed very little over the last several decades, other than isolated, generally small, case study reports (Chen et al. 2017). I believe elbow arthroscopy using all four of the positioning techniques listed in Table 2 can be easily learned and scaled in cadaver labs for surgeon education. There seems to have been little effort to offer large-scale training in the technique of supine or supine suspended elbow arthroscopy such as in cadaver training courses sponsored by the American Academy of Orthopaedic Surgeons (AAOS) and the Arthroscopy Association of North America (AANA). Historically, surgeons in these labs have only been offered training in the lateral decubitus or prone techniques. Given the well-known patient advantages of supine positioning, I find the lack of training options in these courses to be a deficiency in our educational system, particularly for younger surgeons. I addressed this in a “Letter to the Editor” for Arthroscopy back in 2016 (personal correspondence from Hunter, L. to Editor of Arthroscopy, 2016 [copy available upon request]). As further evidence of the lack of promotion of supine or supine suspended elbow arthroscopy, the patient education portal of the AAOS, OrthoInfo, mentions only the lateral decubitus or prone positions in reference to patient positioning for elbow arthroscopy (Athwal and Keener 2021; Keener 2012).
The advantages and disadvantages of the various current patient positioning techniques for elbow arthroscopy have been well documented in the literature. The lateral and prone positioning techniques provide reproducible humeral stability, and thus a stable surgical platform for elbow arthroscopy. However, in my experience, both require laborious preoperative setup and have other significant limitations as other authors have pointed out (see Table 2, which shows a combined analysis from referenced sources). It is worthwhile to note that the Camp et al. articles (Camp, Degen, Sanchez-Sotelo, et al. 2016; Camp, Degen, Dines, Sanchez-Sotelo, et al. 2016; Camp, Degen, Dines, Altchek, et al. 2016), while excellent, do not differentiate between supine and supine suspended techniques. The “cons” of supine positioning that are listed in these articles are attributable to the positioning devices required to use the supine suspended technique. Devices such as the Trimano (Arthrex, Naples, FL) and the Spider (Smith + Nephew, Watford, UK), as well as overhead nonsterile traction devices, affix to the forearm or wrist and do not support the humerus in a reliably stable vertical position. I have found the drifting, swaying, or unstable humerus generally encountered in the supine suspended technique to be a significant distraction, requiring frequent intraoperative arthroscopic reorientation, thus unnecessarily complicating the procedure.
I performed a limited study roughly a decade ago that compared surgical positioning times in my patients who underwent supine elbow arthroscopy (SEA) with those who underwent arthroscopy using the lateral decubitus technique (Hunter 2014). I found the SEA technique remarkably more intuitive to learn and perform, and my data indicated a 20-minute additional positioning time requirement, on average, for the lateral decubitus procedures that I performed at the same facility. This operational inefficiency, in the absence of added value, along with the other benefits of supine positioning, led me to convert exclusively to the SEA technique. Extrapolating the 20 minutes average time savings from that original study to this current case series would suggest that 5,960 minutes or approximately 100 hours of surgical time were directly saved by making the switch to SEA. The downstream economic impact of this times savings to surgeons and facilities is significant.
The benefits of supine positioning to the patient are well-known and well-documented (Baghdadi et al. 2021; Gerken 2013a, 2013b; Wijeratna, Thomas, and Van Rensburg 2012). These include optimal airway access, fewer positioning complications, as well as less inhalational anesthetic load due to shortened overall procedural times versus the same procedure performed in the lateral decubitus or prone position. The benefits to the surgeon and operative team of supine patient positioning are also well-known and well-documented (Baghdadi et al. 2021; Camp, Degen, Dines, Altchek, et al. 2016; Chen et al. 2017; Wijeratna, Thomas, and Van Rensburg 2012). These benefits include accelerated procedural times due to more efficient patient positioning, as well as the ability to convert to an open procedure more quickly and easily if necessary. Experienced surgeons may have acquired the ability to convert to an open procedure with the patient in the lateral decubitus or prone position; however, the supine position provides the surgeon with the most flexibility, the best circumferential access to the elbow joint, and arguably more straightforward intraoperative fluoroscopy (Wijeratna, Thomas, and Van Rensburg 2012).
In my experience, intuitive and efficient SEA relies on creating a stable, vertical humerus oriented perpendicular to the floor. I have found no reason to encumber the forearm and have found that a supported but technically “free” forearm greatly simplifies and expedites both arthroscopic visualization and instrumentation of the elbow joint. Using this SEA technique, the humerus does not sway or drift, thus providing the surgeon with a stable, fixed reference point for orientation. Static positioning can be easily and incrementally adjusted by the surgeon throughout the procedure as the pathology or access dictates without changing the position of the perpendicular, vertical humerus. The surgeon can also range the elbow dynamically in whatever desired manner by manipulating the unencumbered forearm directly, allowing rapid and excellent visualization of large areas of the joint and the entire radial head as needed.
The various ICD codes listed in Supplemental Appendix 1 represent the various pathologies addressed in this case series using the SEA technique. Prior to developing this technique, I performed elbow arthroscopy with the lateral, prone, and even supine suspended position. Since developing this SEA technique over a decade ago, I have used it exclusively for all elbow arthroscopies and have found no contraindications or functional limitations of this positioning technique. Quite the contrary, I have found it improves visualization in both the anterior and posterior compartments and makes manipulating arthroscopic instrumentation easier than other positioning techniques while providing optimum positioning safety and airway access for the patient. Additionally, I personally found arthroscopic surgical orientation to be much more intuitive with a stable, perpendicular vertical humerus.
While many talented elbow surgeons have and will continue to perform elbow arthroscopy using the other techniques with excellent outcomes, I see the inherent limitations with, and well-documented shortcomings of, the other positioning techniques as a real barrier to the proliferation of elbow arthroscopy and arthroscopic innovation. I have found SEA to be safe and efficient, providing reliably excellent visualization and surgical access throughout the elbow.
The case series data in Table 1 demonstrate the safety, utility, efficacy, and efficiency of elbow arthroscopy performed in the supine position with a stable, vertical humerus and a free forearm. I believe the metrics regarding procedural times, arthroscopic surgical times, and nonsurgical times in the OR revealed in this case series would compare favorably to data from similar series with patients positioned in the lateral decubitus or prone position. I would encourage our professional societies and training institutions to consider offering SEA training to surgeons in residency, fellowship programs, and professional cadaver labs.
CONCLUSION
SEA promotes safe, technically easier, and more efficient elbow arthroscopy with improved surgical access, intraoperative flexibility, and accelerated procedural times compared with other current techniques. The author believes that this analysis should promote discussion among elbow surgeons regarding best practices in elbow arthroscopy and motivate consideration of incorporating SEA into their own practices as well as the training of future generations of surgeons performing elbow arthroscopy.