








Introduction
Pediatric distal radius fractures are among the most common fractures seen in children, accounting for 35-45% of all pediatric forearm fractures and 20% of all pediatric fractures in general (Beekman and Sullivan 1941; Pierog and Pierog 1985; Cheng et al. 1999). These fractures frequently occur after a fall on an outstretched wrist during play or sports and often are Salter-Harris II injuries (Do et al. 2003; Bae 2008). While the majority of Salter-Harris II injuries displace dorsally due to the mechanism of injury, much like a Colles’ fracture, Cha et al. described a case series of pediatric volar Barton fractures that were unstable and tended to displace volarly (Cha and Shin 2019). Due to open physes and remodeling potential, the majority of pediatric distal radius fractures can be reduced and managed by immobilization and casting with excellent clinical outcomes (Do et al. 2003; Bae 2008). In fact, in a study by Houshian et al., remodeling after a Salter-Harris type II distal radius fracture was observed in all age groups, with greater potential noted in children up to 10 years of age, and no substantial long-term impact on wrist range of motion and grip strength (Houshian et al. 2004).
As children have a thick, vascular, and highly osteogenic periosteum that is rarely torn circumferentially, fracture reduction techniques must be tailored to the pediatric physiology (Bae 2008). While the periosteum can be used to aid in fracture reduction, excessive traction and tension can also block reduction (Bae 2008). For adolescents in particular, who may end up being treated as adults in the general emergency setting, fracture reduction can be deceptively challenging, since the periosteum is not visible on plain radiography.
Both of our cases were adolescents referred from adult accident and emergency departments after manipulation and reduction of their distal radius fractures. What might be a straightforward procedure in an adult was complicated by displacement of volar fracture fragments resulting in tenting of the tendons and neurovascular structures. These case reports highlight the importance of appreciating the thicker periosteum in children and the correct technique of reducing pediatric distal radius fractures.

Case Report
Case Presentation
Case 1
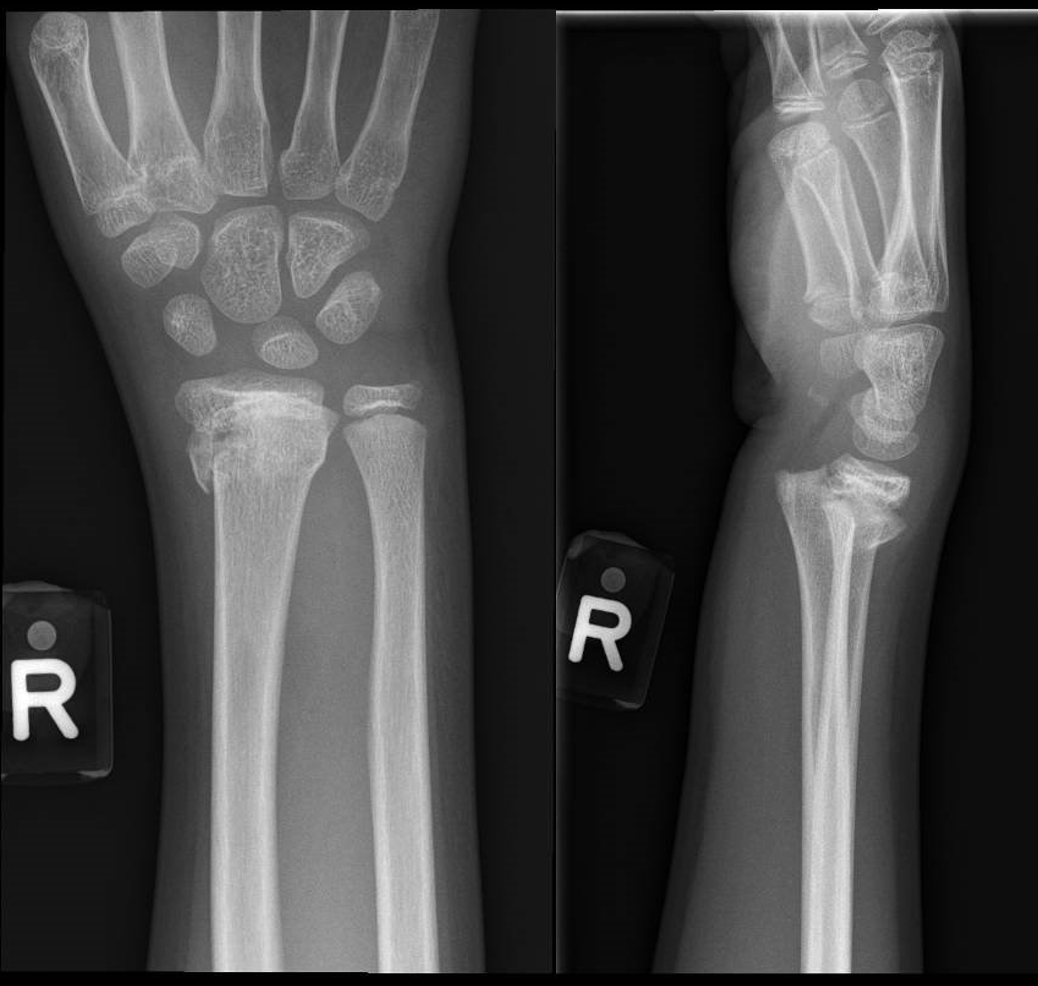
A right-hand-dominant 12-year-old boy presented to the accident and emergency department of an adult hospital with right wrist pain and swelling after falling from the top of a two-meter slide and landing on his outstretched right hand. There were no other injuries. Examination showed a swollen, deformed and tender right wrist. There was no broken skin or neurovascular deficits. Initial radiographs showed a displaced, comminuted Salter-Harris II distal radius fracture (Figure 1). Manipulation and reduction were attempted twice under Bier’s block and the fracture was immobilised in a plaster of Paris slab. While post-reduction radiographs showed reduction of the Thurston-Holland fragment, there was displacement of the volar fracture fragment (Figure 2). The child was subsequently transferred to the children’s emergency department for a pediatric orthopaedic surgical consult. Although the child did not develop symptoms of acute carpal tunnel syndrome by the time he arrived at the children’s emergency department, skin tenting was noted upon arrival. Closed manipulation and reduction at the children’s emergency department was unsuccessful.


Case 2
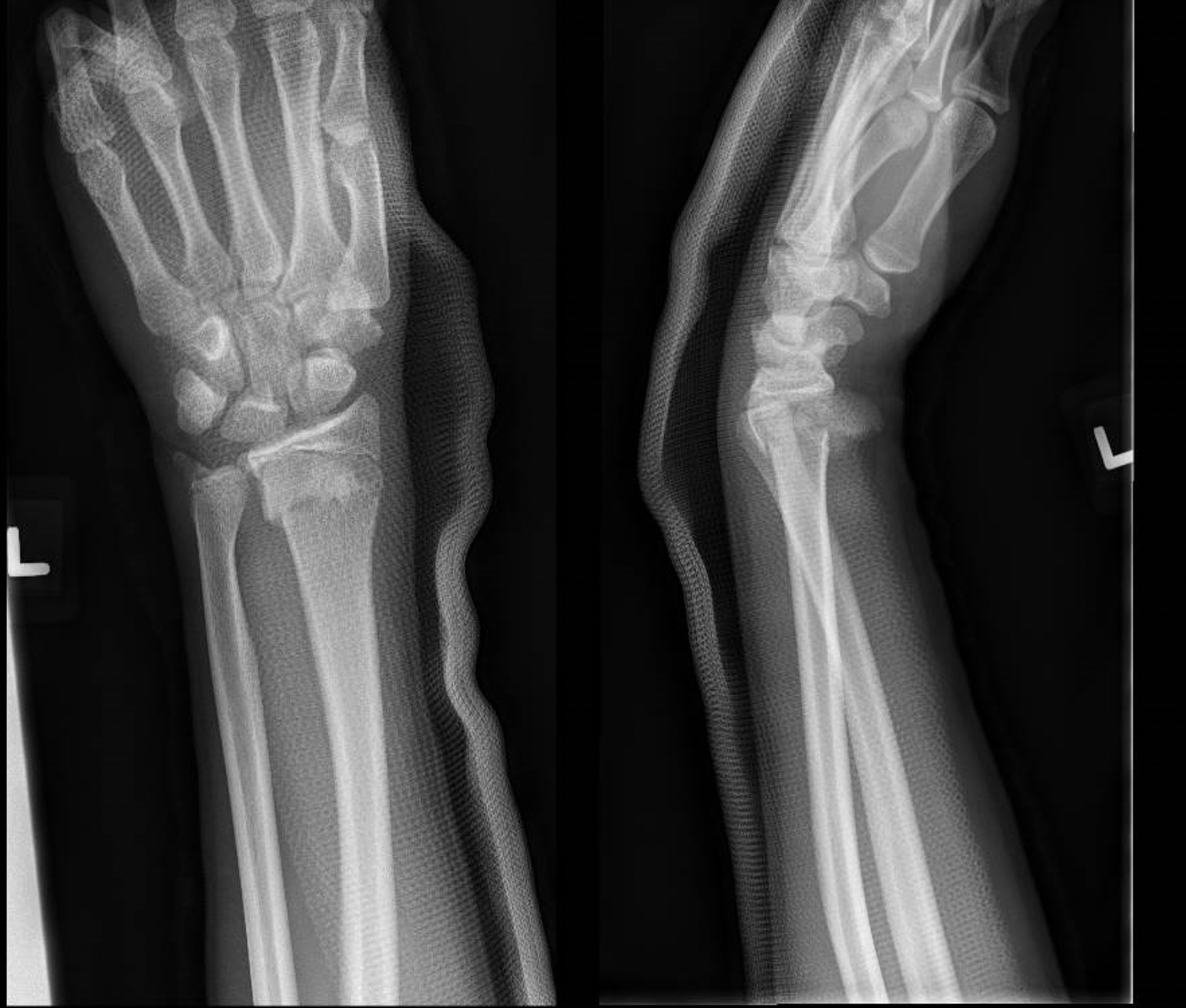
A right-hand-dominant 16-year-old boy presented to the accident and emergency department of an adult hospital with left wrist pain and deformity after falling on his outstretched hand. He had been holding onto a basketball hoop and broke his fall with his left upper extremity. He sustained no other injuries and was brought immediately to the hospital by an ambulance. Physical examination revealed a dinner fork deformity with a 2 x 2 mm abrasion over the ulnar styloid. There were no open injuries and his neurovascular status was intact with no signs of carpal tunnel syndrome. Initial radiographs showed a displaced, angulated, and comminuted Salter-Harris II fracture of the distal radius (Figure 3). Manipulation and reduction were attempted under Bier’s block and the fracture was subsequently immobilized in a plaster of Paris slab. Post-reduction radiographs showed reduction of the Thurston-Holland fragment, but displacement of the volar fracture fragment (Figure 4). The child was subsequently referred to the adult orthopaedic service, which then arranged for transfer to our pediatric tertiary institution. Upon arrival at our institution, the patient was noted to have skin tenting with the volar fracture fragment felt below the skin. There was no open injury, hematoma, bruising, or signs and symptoms of neurovascular compromise (Figure 5).



Investigations
Plain radiography is the preferred initial investigation for children with wrist pain after an injury and typically consists of a standard anteroposterior and lateral radiograph of the wrist. Other associated joints should also be imaged based on clinical presentation and may include the hand, forearm, elbow, and shoulder, as well as other injured areas. Radiographs define the presence of the fracture, degree of displacement, presence of comminution, size of fragments, intraarticular involvement, and joint alignment. Associated injuries to nearby structures such as the distal radio-ulnar joint, ulnar styloid, and scapholunate interval can also be assessed. Soft tissue swelling can also be approximated on plain radiographs.
Additionally, post-reduction films are important in determining the quality of the reduction and assessing any complications that might have occurred. In both cases, while the overall alignment of the distal radius fracture was improved, the displaced volar fracture fragment was well visualized on the lateral film. CT scans are rarely used in children given the concerns for radiation exposure and are better used to characterize intra-articular fractures. A Doppler ultrasound or vascular study can be useful if there is concern about arterial injury or vascular compromise.

Treatment
Case 1
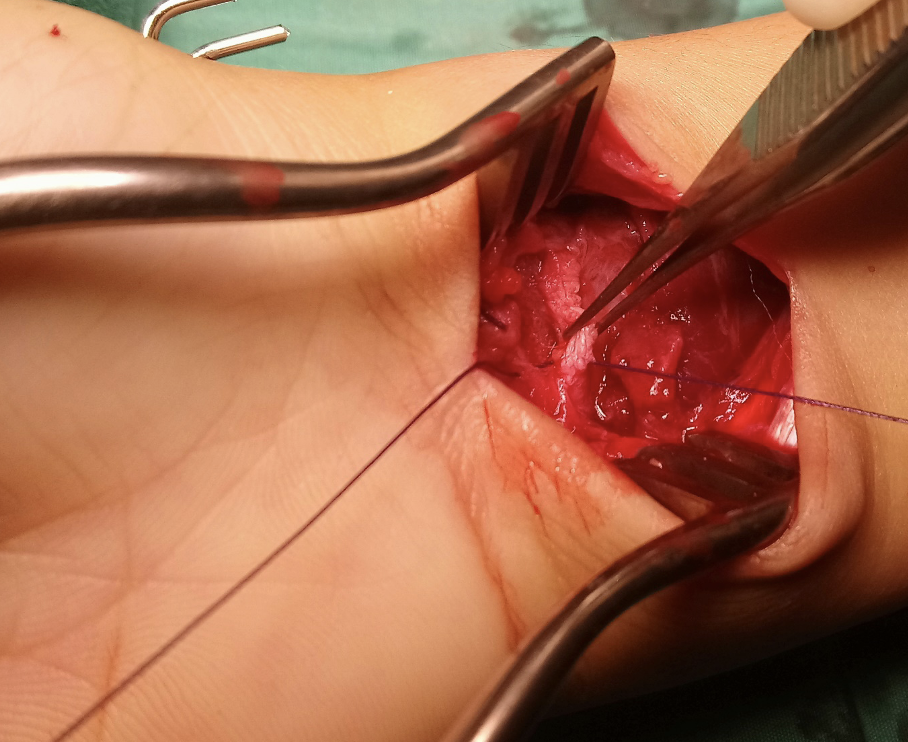
The child subsequently underwent open reduction and percutaneous pinning after unsuccessful attempted closed reduction under general anaesthesia. Intraoperatively, the volar fracture fragment was found to have punctured through the pronator quadratus and was severely tenting the median nerve and flexor tendons (Figure 6). The pronator quadratus was freed from the fragment to allow reduction. The volar periosteum and pronator quadratus were then repaired individually with vicryl 4-0 to stabilise the fragment (Figure 7). Two divergent 1.6mm Kirschner wires were inserted percutaneously and through the radial styloid to fix the Thurston-Holland fragment as the volar fracture fragment in the metaphyseal region had rendered the fracture unstable (Figure 8). Wires were not used to fix the volar fragment as it was adequately stabilized with the periosteum and pronator quadratus muscle repair. In addition, the wire tip of an anteroposterior Kirschner wire either from a volar or dorsal entry point would irritate the tendons or the median nerve.



Case 2
The child subsequently underwent open reduction and internal fixation of his left distal radius fracture. Intraoperatively, the distal radius fracture was noted to be severely comminuted with the volar fracture fragment found to have lacerated the pronator quadratus. The median nerve and flexor tendons were found to be intact and protected throughout the surgery. The distal radius fracture was fixed with a 3.5 mm locking plate and the pronator quadratus repaired over the plate with vicryl 4-0.
Outcomes
Case 1
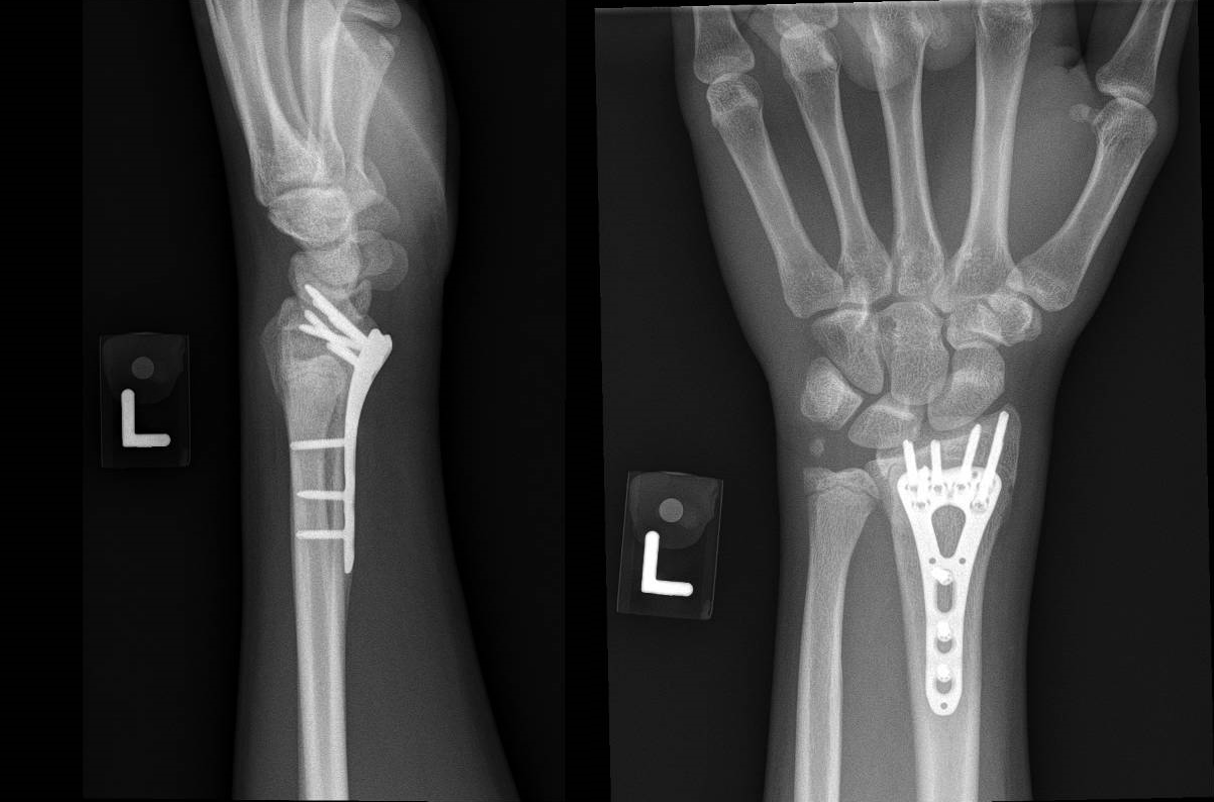
The child recovered well without any further complications. The percutaneous pins were removed in the outpatient clinic at four weeks. The fracture united within two months (Figure 9). The child regained normal function of the right wrist and was allowed to resume full activities.

Case 2
The child was noted to have superficial skin necrosis one week postoperatively (Figure 10). The area of necrosis corresponded with the area of skin tenting seen preoperatively. He had no fever or symptoms of infection thus the skin necrosis was managed conservatively with wound care. The skin necrosis subsequently resolved and the child was cleared for regular activities (Figure 11). The fracture united within two months (Figure 12). The patient opted to remove the plate at a later date.




Discussion
To our knowledge, displacement of a volar fracture fragment caused by manipulation and reduction of distal radius fractures in the pediatric population has not been reported in the literature. A review of the literature shows that repeated and aggressive reduction attempts may lead to increased fracture comminution, loss of reduction in the cast, and even long-term physeal arrest, thus it is not recommended in children (Roth et al. 2014). Furthermore, we believe that in these cases, the reduction technique was incorrectly applied. It was likely that longitudinal traction was applied immediately. This tightened the periosteum and, in an attempt to reduce the fracture, an anteriorly directed force over the distal fragment might have further displaced the volar fracture fragments in both instances.
The ideal technique would have been to first exaggerate the deformity (Bae 2008). In both cases, the distal fragment was displaced dorsally. The volar aspect, being the tension side, would have caused the periosteum on that side to be torn off, while the dorsal periosteum would likely remain intact. Further angulating the distal fragment dorsally accentuates the deformity and relaxes the dorsal lying periosteum, which is almost always stripped but still intact. With the distal fragment still angulated, distal traction is then applied to match the dorsal cortices. The distal fragment is then palmar flexed to restore alignment. As the dorsal periosteum is intact, a below-elbow slab placed in the acute setting is sufficient for a stable immobilisation. This is subsequently changed to a full below-elbow cast in mild palmar flexion, immobilizing the fracture with three-point fixation (Bae 2008).
In summary, we describe two cases of manipulation and reduction of pediatric distal radius fracture resulting in displacement of the volar fracture fragments. Key learning points from the cases are as follows:
-
When performing manipulation and reduction of fractures, we need to be mindful of the periosteum, which is especially thicker in children and almost always intact.
-
The principles of closed fracture reduction must be adhered to - exaggerating the deformity to relax the periosteum, matching the cortical ends and levering the fragments back into alignment.
-
Forceful and/or multiple attempts at reductions in pediatric distal radius fracture in children can increase the risk of iatrogenic complications, including fracture displacement, soft tissue injury, neurovascular compromise, and tearing of the periosteum, which is essential for stability.
-
Skin tenting following fractures must be relieved as soon as possible to avoid skin necrosis, neurovascular injury, and loss of function.
-
Distal radius fractures with displaced volar fracture fragments in children are an uncommon and unstable injury with risk of displacement with reduction attempts.