INTRODUCTION
Loss to follow-up is a persistent obstacle to comprehensive orthopaedic trauma care. Postoperative outpatient follow-up provides the opportunity to identify surgical complications, such as wound dehiscence, infection, venous thrombosis, and fracture nonunions or malunions (Casp et al. 2017; Zelle et al. 2015). Furthermore, loss to follow-up hinders the ability to address the individual needs of a patient’s postoperative recovery, such as adjusting weightbearing status or physical therapy regimen (Zelle et al. 2015). These implications become a public health concern when considering that up to one-third of orthopaedic trauma patients fail to attend their first scheduled outpatient appointment (Whiting et al. 2015). Failure to address these issues in a timely manner is a major obstacle to maximizing optimal surgical outcomes, and preventing a catastrophic postoperative complication.
The orthopaedic trauma surgery literature is also impacted by loss to follow-up due to the effect it has on clinical research. Loss to follow-up can introduce bias into a clinical study, thus threatening the validity of the results (Somerson et al. 2016; Zelle et al. 2013). In a simulated series using data on orthopaedic polytrauma patients, Zelle et al (Zelle et al. 2013). demonstrated that a 20% loss to follow-up alters the statistical significance of functional outcomes in nearly one-third of simulations. Somerson et al (Somerson et al. 2016). recently reported that the mean loss to follow-up rate in orthopaedic randomized clinical trials (RCTs) published between 2008-2011 was 10.4%. However, a major finding was that loss to follow-up was not reported in 20% of the studies reviewed (Somerson et al. 2016). Without a complete understanding of which patients are being lost to follow-up, researchers often turn to “worst-case scenario” analyses to incorporate missing data, which many researchers argue does not provide a valid representation of orthopaedic populations (Nouta et al. 2013; Rowden et al. 2012).
Considering this, it is prudent to ask who is being lost to follow-up? More critically, it must be determined if vulnerable populations are disproportionately being lost to follow-up and thus receiving less care and less representation within the orthopaedic trauma literature. There is concern among researchers regarding the large proportion of disenfranchised populations, particularly racial and ethnic minorities, that are lost to follow-up (Somerson et al. 2016; Psaty et al. 1994; Janson, Alioto, and Boushey 2001). Within orthopaedic surgery, this issue is poorly understood. However, recent research denotes that both African American and Hispanic patients are significantly underrepresented within orthopaedic clinical trials in a manner that is disproportionate to the size of these groups within the greater population of the United States (Somerson et al. 2014). Knowledge is limited regarding whether compliance with follow-up is a contributing factor to this finding. Therefore, it is imperative to elucidate whether vulnerable populations, such as racial and ethnic minorities and patients of low socioeconomic status, are disproportionately lost to follow-up within orthopaedic trauma surgery.
The issue of loss to follow-up in orthopaedic trauma surgery persists despite a growing body of literature detailing its risk to both patients and clinical data. Furthermore, there is concern that these risks weigh more heavily on vulnerable populations given previous research identifying a high rate of loss to follow-up in such groups. In order to better understand loss to follow-up in orthopaedic trauma surgery, the present research aims to systematically review the literature to better define four questions: 1) Are racial and ethnic minorities at risk for loss to follow-up? 2) Are socioeconomic status and other demographic factors associated with loss to follow-up? 3) What are the patient-reported reasons for loss to follow-up? and 4) Does loss to follow-up affect functional outcomes?
METHODS
A systematic query of the literature on the Medline and Cochrane databases was conducted to identify articles containing the Medical Subject Headings (MeSH) terms “orthopedics” or “orthopedic procedures,” each of which was combined with the MeSH term “lost to follow-up” or the keywords “compliance” or “attrition.” Therefore, there were 6 total pairs of search terms. The query was performed on 24 September 2019. All studies published prior to that date were considered. In addition to the primary literature query, a secondary screening was completed by reviewing the works cited by each study retained from the primary search.
Studies were retained for review if they 1) were published in the English language; 2) described patients who underwent surgical treatment for a traumatic orthopaedic injury; 3) recorded patient compliance for at least the first scheduled outpatient follow-up appointment; 4) reported characteristics associated with patients who failed to comply with outpatient follow-up or reported patient-cited reasons for failure to comply with outpatient follow-up.
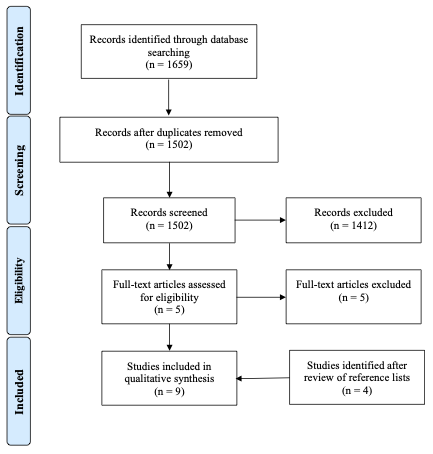
The initial query yielded 1,502 unique studies (Figure 1). Each title was reviewed and those that were evidently irrelevant to the review topic were eliminated (1,412). The abstracts of the remaining 90 articles were then reviewed for relevance regarding the inclusion criteria listed above; 80 articles were eliminated because the abstract contained information deemed discordant with the inclusion criteria. All of the remaining 10 articles were reviewed in their entirety, and 5 articles were eliminated due to failure to meet the inclusion criteria. After each of these phases, 5 articles remained for review.

All of the articles that were retained after the initial query were then entered into a secondary screening phase, which began with a screening of article titles in the works cited by each retained article. The secondary screening phase proceeded in the same manner as the primary screening, insofar as the abstracts were next analyzed, followed by the full-text articles, and ultimately 4 articles that met the inclusion criteria were retained. At the end of the primary and secondary queries, 9 articles remained for review.
RESULTS
Nine studies met the inclusion criteria (Casp et al. 2017; Zelle et al. 2015; Whiting et al. 2015; Badenhorst et al. 2018; Hoffmann, Sietsema, and Jones 2016; Madden et al. 2017; Murnaghan and Buckley 2002; Rafael Arceo et al. 2018; Tejwani et al. 2010). Together, these studies included 7,188 orthopaedic trauma patients (Table 1). A total of 1,728 (24.0%) patients were considered lost to follow-up over a range of 2 weeks to 2 years postoperatively. Four studies defined loss to follow-up as failure to attend the first scheduled outpatient visit or failure to attend any scheduled appointments thereafter (Casp et al. 2017; Whiting et al. 2015; Badenhorst et al. 2018; Tejwani et al. 2010), whereas 4 studies defined loss to follow-up as failure to comply over a period up to 6 to 24 months (Zelle et al. 2015; Hoffmann, Sietsema, and Jones 2016; Madden et al. 2017). One study utilized a compliance fraction (number of attended follow-up visits/(number of attended follow-up visits + number of missed follow-up visits)), and defined high compliance as a ratio of 0.75 or higher (Rafael Arceo et al. 2018). Among those studies only concerned with immediate postoperative follow-up, 868 (27.1%) of 3,206 patients were lost to follow-up. Meanwhile, those studies with longer follow-up cumulatively lost 503 (14.9%) of 3,369 patients to follow-up. In the single study that utilized a compliance fraction, 357 (58.3%) of 612 patients had a compliance fraction less than 0.75 over a maximum of two years (Rafael Arceo et al. 2018). Due to inconsistency regarding the definition of loss to follow-up and outcomes measured in each study, the data were not homogenous enough to perform quantitative comparative analyses.
Are racial and ethnic minorities at risk for loss to follow-up?
Among the 9 studies that met the inclusion criteria, only 3 reported data regarding patient race or ethnicity (Murnaghan and Buckley 2002; Rafael Arceo et al. 2018; Tejwani et al. 2010). Utilizing the compliance fraction to compare white and African American patients, Arceo et al (Rafael Arceo et al. 2018). found that white race was not associated with higher likelihood of high compliance (OR 1.31, 95% CI 0.90-1.90). In an analysis of demographic characteristics associated with loss to follow-up, Tejwani et al (Tejwani et al. 2010). did not determine any differences in the proportion of white, black, Asian or Hispanic patients who were lost to follow-up. Using a similar method of characterizing the demographics of orthopaedic trauma patients lost to follow-up within a Canadian database, Murnaghan et al (Murnaghan and Buckley 2002). found that indigenous peoples were significantly more likely to be non-compliant with follow-up (6/8, 80%) compared to non-indigenous patients (32/228, 14%; p<0.001).
Are socioeconomic status and other demographic factors associated with loss to follow-up?
Among the various measures for socioeconomic status, several of the studies examined the role of income (Tejwani et al. 2010), tobacco use (Zelle et al. 2015; Whiting et al. 2015; Badenhorst et al. 2018; Madden et al. 2017; Murnaghan and Buckley 2002), education level (Tejwani et al. 2010), and occupation (Zelle et al. 2015; Madden et al. 2017; Murnaghan and Buckley 2002; Tejwani et al. 2010) as risk factors for loss to follow-up. With regard to income, patients with higher annual income levels are more likely to return for follow-up than lower income patients. Of 54 patients lost to follow-up, thirty-seven (68.5%) reported having annual income levels less than $25,000 (Tejwani et al. 2010). Smoking status is also a significant predictor for loss to follow-up, with a relative risk of 1.20 and an odds ratio of 1.82 (95% confidence interval 1.28-2.58) (Whiting et al. 2015; Madden et al. 2017). One study noted that twenty-nine (76.3%) of its patients lost to follow-up were active tobacco users (Murnaghan and Buckley 2002). As a risk factor, tobacco use is correlated with lower socioeconomic status and is negatively correlated with education (Whiting et al. 2015). With regard to education, patients with postsecondary education degrees are more likely to return for follow-up, as forty (74.0%) patients lost to follow-up attained at most a high school diploma (Tejwani et al. 2010). Though some studies found no significant correlation between patient occupation and follow-up status (Zelle et al. 2015; Tejwani et al. 2010), one study reported that differences in occupational categories for patients who fail to follow-up can be used as an indicator for discrepancies in socioeconomic status and education level, as twenty-four (63.2%) of patients lost to follow-up were employed in unskilled positions such as clerks, sales, service, or labor (Murnaghan and Buckley 2002).
With regard to additional demographics, four studies determined male sex (Zelle et al. 2015; Hoffmann, Sietsema, and Jones 2016; Madden et al. 2017; Rafael Arceo et al. 2018) as an independent risk factor for loss to follow-up. Three studies each found that patients with no insurance or government insurance (Casp et al. 2017; Zelle et al. 2015; Whiting et al. 2015) and younger patients (Hoffmann, Sietsema, and Jones 2016; Madden et al. 2017; Murnaghan and Buckley 2002) were at increased risk of loss to follow-up. Significant travelling distance to follow-up was found to be an independent risk factor for loss to follow-up in two studies (Whiting et al. 2015; Badenhorst et al. 2018). Furthermore, one investigation of an international RCT determined that the most significant predictor of loss to follow-up was receiving care in the United States compared to Canada, Europe, or Australia (odds ratio 3.56, 95% confidence interval 2.46-5.17) (Madden et al. 2017).
What are the patient-reported reasons for loss to follow-up?
Only three studies assessed patient-reported reasons for not attending follow-up, which included 166 total patients questioned (Casp et al. 2017; Hoffmann, Sietsema, and Jones 2016; Tejwani et al. 2010). Thirty-one (18.7%) cited distance or inconvenience as the primary reason for not attending follow-up. Meanwhile, 19 (11.4%) patients stated that they did not attend follow-up because they were feeling well (Casp et al. 2017). Nine (5.42%) patients stated insufficient insurance as the primary reason for failure to follow-up (Hoffmann, Sietsema, and Jones 2016), while dissatisfaction or unawareness of the appointments was cited by 4 (2.41%) patients each (Casp et al. 2017; Hoffmann, Sietsema, and Jones 2016).
Does loss to follow-up affect functional outcomes?
Two studies assessed functional outcomes between patients lost to follow-up and those who were not (Hoffmann, Sietsema, and Jones 2016; Tejwani et al. 2010). One study examined loss to follow-up in tibial plateau fractures and recorded results for all patients using the Short Musculoskeletal Function Assessment (SMFA), visual analog scale (VAS) and range of motion (ROM) measurements (Hoffmann, Sietsema, and Jones 2016). Notably, the last recorded values prior to non-compliance with follow-up were used to compare patients lost to follow-up to those who were compliant over a 24-month period. Overall, no differences in the SMFA, VAS, or ROM were found; however, sub-analysis of ROM by patient sex revealed that males who were lost to follow-up after 12 months had an average of 8° greater flexion than those who completed 24-month follow-up (Hoffmann, Sietsema, and Jones 2016). Another study of patients lost to follow-up after either operative or non-operative treatment of distal radius fractures used the Short Form 36 (SF-36) health survey and the Disabilities of the Arm, Shoulder, and Hand (DASH) score to assess functional differences between patients with a two-week follow-up or less and those with a minimum follow-up of 6 months (Tejwani et al. 2010). While operatively managed patients were more likely to be compliant with follow-up compared to those treated non-operatively, lower physical and mental health components on SF-36 were independently associated with loss to follow-up regardless of management group (p=0.0049 and p=0.0261, respectively) (Tejwani et al. 2010).
DISCUSSION
Among all orthopaedic trauma patients included in this study, nearly one-quarter were lost to follow-up between 2 weeks and 2 years postoperatively. This finding is consistent with the suggestion that orthopaedic trauma patients are particularly at risk for loss to follow-up (Zelle et al. 2013; Sprague et al. 2003). However, in a recent investigation of loss to follow-up in orthopaedic RCTs, Somerson et al (Somerson et al. 2016). found that the rate of loss to follow-up in orthopaedic trauma trials (10.5%) was similar to the overall rate among all orthopaedic subspecialties (10.4%). Notably, RCTs are designed to minimize loss to follow-up. Among the nine studies included in the present review, only two utilized data available from RCTs while the remaining studies were all retrospective cohort designs. With the exception of one cohort study (Casp et al. 2017), the two studies of RCT data demonstrated the lowest rates of follow-up attrition (Madden et al. 2017; Murnaghan and Buckley 2002). For patients who are participating in RCTs, there may be increased emphasis for follow-up or selection bias in choosing patients who are more likely to follow-up.
The high rate of non-compliance with follow-up found in this study has concerning implications regarding the validity of data used within the orthopaedic trauma literature. Utilizing a simulation of orthopaedic trauma patient data, Zelle et al (Zelle et al. 2013). demonstrated that a 20% loss to follow-up changes the statistical significance of functional outcomes in approximately one-third of simulations. While it appears that RCTs in orthopaedic trauma retain on average enough patients to maintain validity, other study designs might be easily compromised due to lack of follow-up. This is particularly relevant when considering that RCTs represent only a small minority of primary investigations in orthopaedic surgery (Baldwin et al. 2012). While the present study was limited to investigations focusing on patients lost to follow-up after orthopaedic trauma surgery, the rate of attrition found here warrants further examination of follow-up compliance as it pertains to the validity of data within the orthopaedic trauma literature.
Furthermore, the paucity of data regarding loss to follow-up among minority populations is alarming. While the issue of loss of follow-up among disenfranchised populations is poorly understood in general, it is even more poorly defined within the field of orthopaedic surgery (Psaty et al. 1994; Janson, Alioto, and Boushey 2001; Somerson et al. 2014). Our systematic review of the literature determined that there is no evidence of greater loss to follow-up between white and African American patients, but that there is evidence of higher attrition rates among indigenous populations. This finding is particularly concerning because of the implications that it has regarding the care of not only those patients lost to follow-up, but also the resultant knowledge divide regarding the orthopaedic care of disparate populations. Given the limited evidence that disenfranchised populations are at risk for loss to follow-up, this particular conundrum merits further investigation.
Additionally, the lack of data considering the role of socioeconomic status in patients lost to follow-up is another reason for concern. Although income and education levels are considered two major proxies for socioeconomic status, their effect on patient follow-up in the field of orthopaedics is not well-documented. Evidence shows that individuals with higher income and education levels are less likely to be lost to follow-up; however, additional research is needed to validate these findings (Tejwani et al. 2010). This review also found that no correlation exists between employment and follow-up status (Zelle et al. 2015; Tejwani et al. 2010); however, the category of occupation was shown to be a significant factor, with individuals in unskilled positions being more likely to be lost to follow-up than those in skilled positions (Murnaghan and Buckley 2002). Ensuring information regarding these socioeconomic factors is documented during patient encounters or on intake forms can serve not only as a predictive clinical tool for future follow-up status, but could also fuel further investigations into this topic.
Notably, tobacco use emerged as a strong risk factor for loss to follow-up after orthopaedic trauma surgery in our review. Compared to the general population, tobacco use is over twice as prevalent in orthopaedic trauma patients (Neptune et al. 2014). The evidence that tobacco use is an independent risk factor for loss to follow-up is particularly concerning considering the increased risk of complications associated with tobacco use, including postoperative infection (Sørensen 2012; Nåsell et al. 2011), wound necrosis (Sørensen 2012), and nonunion or delayed union (Patel et al. 2013). While tobacco use itself is unlikely to be directly responsible for loss to follow-up, instead it represents a well-defined, yet multifactorial characterization of patients at risk for loss to follow-up. For example, the prevalence of tobacco use in the United States has a strong association with other risk factors of loss to follow-up identified in this study, which includes males and younger individuals (King, Dube, and Tynan 2012). However, tobacco use can also be used as a proxy for disadvantaged socioeconomic status, which is often challenging to define within clinical investigations (Whiting et al. 2015). In general, tobacco use is associated with less education and less wealth (King, Dube, and Tynan 2012). Understanding the evidence-based associations between tobacco use and sociodemographic characteristics can help clinical workers identify patients who are at risk of being lost to follow-up. These patients might benefit from a consultation with social workers pre-operatively in order to develop an individualized follow-up instruction plan.
There appears to be agreement in the literature regarding the relationship between patient demographics and loss to follow-up after orthopaedic trauma surgery. In particular, male patients are commonly lost to follow-up. This finding is unsurprising considering well-documented evidence that male patients are less likely than females to utilize health care services (Bertakis et al. 2000; Verbrugge, Wingard, and Features Submission 1987; Green and Pope 1999), report acute health conditions (Bertakis et al. 2000), disregard preventive health care (Juel and Christensen 2008), and delay seeking treatment for illness (Galdas, Cheater, and Marshall 2005). Researchers have suggested that Western perceptions of traditional masculine behaviors, such as toughness and self-resilience, contribute to these observed differences (Galdas, Cheater, and Marshall 2005). Therefore, exploring methods to address this belief system within discharge protocols is an appropriate initial step towards ameliorating the high rate of males lost to follow-up.
Younger patient age was also determined to be associated with greater risk of loss to follow-up. There are several reasons that might explain this finding. One reason is that older patients who sustain an acute orthopaedic injury are more likely than younger patients to have co-morbidities and are also at increased risk of a complicated hospital admission. Therefore, older orthopaedic trauma patients are more likely to be discharged to skilled nursing or rehabilitation facilities (Sacks, Hill, and Rogers 2011), which would either obviate the need for early follow-up or increase the likelihood of follow-up compliance due to collaboration between health care facilities (Stone et al. 2014). Going further, the finding that younger age is associated with loss to follow-up likely factors with the finding that uninsured or government insured patients are more commonly lost to follow-up. For example, in 2017 it was estimated that 86% of the uninsured population in the United States were nonelderly adults (“Kaiser Family Foundation Analysis of 2017 American Community Survey (ACS), 1-Year Estimates” 2018). Uninsured patients who are injured are less likely than patients with insurance coverage to adhere to all recommended care services (Hadley 2007). For younger patients, particularly those who are uninsured, a traumatic injury requiring orthopaedic surgical treatment might represent their first experience with surgical or inpatient care. Recognizing this possibility, members of the care team can assist the patient in navigating their postoperative care by emphasizing the importance of following up while minimizing the associated time, travel, and financial commitments for the patient.
The present review identified only three investigations of patient-reported reasons for failure to attend follow-up. Nevertheless, the finding most cited as the primary reason for follow-up non-compliance—travel distance or inconvenience—is consistent with prior publications. Namely, uninsured or under-insured patients and patients of lower socioeconomic status are known to disproportionately encounter transportation barriers to accessing health care (Syed, Gerber, and Sharp 2013). Using these characteristics to identify patients that might be at risk of missing follow-up appointments due to transportation or scheduling difficulty represents an opportunity to counsel patients on the timing, location, and necessity of postoperative follow-up. In addition, this subset of patients might benefit from alternative follow-up modalities, such as videoconferencing (Sathiyakumar et al. 2015; Buvik et al. 2018), to replace or limit the number of in-person follow-up visits.
Another commonly cited reason for failure to follow-up in this study was patients stating that they felt well. This finding suggests that loss to follow-up might be attributable to voluntary decisions made by the patient (Casp et al. 2017). Stated differently, loss to follow-up might be an individual-level issue instead of a shortcoming at the system level such as failures regarding collecting patient contact information, patient education, appointment scheduling, and predicting and managing logistical barriers. However, the general trend that RCTs are associated with less follow-up attrition than retrospective cohort analyses suggests that loss to follow-up in orthopaedic trauma could be more of a system-level issue rather than a patient-level problem. Evidence to support this theory is provided by data extracted from multi-national RCTs. For example, Somerson et al (Somerson et al. 2016). found that RCTs performed within the United States had significantly greater loss to follow-up compared to those performed outside of the United States. Likewise, a study included in the present review performed by Madden et al (Madden et al. 2017). analyzed loss to follow-up within a multi-national RCT and found that the strongest predictor of loss to follow-up was patients having received care in the United States compared to Canada, Europe and Australia. Despite these observations, the reasons for these findings on both individual and system levels is undoubtedly multifactorial and requires investigation.
The high rate of non-compliance with follow-up found in this study has concerning implications regarding the validity of data used within the orthopaedic trauma literature. Utilizing a simulation of orthopaedic trauma patient data, Zelle et al (Zelle et al. 2013). demonstrated that 20% loss to follow-up changes the statistical significance of functional outcomes in approximately one-third of simulations. While it appears that RCTs in orthopaedic trauma retain on average enough patients to maintain validity, other study designs might be easily compromised due to lack of follow-up. This is particularly relevant when considering that RCTs represent only a small minority of primary investigations in orthopaedic surgery (Baldwin et al. 2012). While the present study was limited to only investigations focusing on patients lost to follow-up after orthopaedic trauma surgery, the rate of attrition found here warrants further examination of follow-up compliance as it pertains to the validity of data within the orthopaedic trauma literature.
The present review has both strengths and limitations. Primarily, this is the first review of loss to follow-up within orthopaedic trauma surgery. Through a systematic review of the current literature, numerous characteristics and reasons why orthopaedic trauma patients are lost to follow-up were distinguished. More importantly, numerous areas for additional investigation and quality improvement initiatives were identified. However, all systematic reviews are limited by the quality of the included studies. In particular, this review was limited by significant heterogeneity among the included studies, which reported variable patient characteristics, follow-up lengths, definitions of follow-up compliance, attempts at contacting lost patients, and patient-reported outcomes. Similarly, there was considerable variability regarding the orthopaedic injuries studied, which ranged from low-energy injuries such as distal radius fractures to high-energy injuries such as tibial plateau fractures and polytrauma. Furthermore, there was inconsistent reporting of variables such as patient age, which limited the ability to synthesize data for analysis.
CONCLUSION
Our review confirms that there is a high rate of follow-up non-compliance after orthopaedic trauma. Furthermore, this study found that the orthopaedic trauma patient lost to follow-up is likely to be male, young, a current tobacco user, and uninsured or on a government health insurance plan. Notably, there is a critical need for further research to better describe loss to follow-up among minority populations and the subsequent effect this has on their care. While some research suggests that loss to follow-up in orthopaedic trauma surgery might be a voluntary decision made by patients, this research identified risk factors for failure to follow-up that can be directly addressed by system-level changes, such as patient education and discharge protocols designed to predict and address barriers to follow-up compliance. Additional research is needed to determine the extent to which clinical outcomes differ between patients lost to follow-up and those who are compliant.