INTRODUCTION
Opioid prescribing after total knee arthroplasty (TKA) presents significant risks for patients and burden to the healthcare system and society. Prolonged opioid use after TKA is common is associated with higher rates of infection, stiffness, and aseptic revision (Cancienne et al. 2018). In a study of 23,726 patients who underwent TKA at an integrated healthcare system during 2008-2011, 92.7% of patients had a prescription for opioids dispensed during the first 90 days after surgery, 42% during postoperative days 91-180, 32.2% during postoperative days 181-270, and 30.4% during postoperative days 271-360 (Namba et al. 2018). A national database study of 113,337 TKA patients treated from 2007-2015 found that 32% patients were prescribed opioids for more than 3 months postoperatively with prolonged opioid use (Cancienne et al. 2018).
Excessive prescribing of opioids after TKA, identified in multiple studies (Hernandez, Parry, and Taunton 2017; Atwood et al. 2021; Runner et al. 2020; Huang and Copp 2019), increases the risks for misuse, abuse, dependence, diversion, and overdose, and contributes to the national opioid crisis that exacts significant health and economic burdens for patients, their families, the healthcare system, and society (Heins 2019; SAMSHA 2010, 2012; Centers for Disease Control and Prevention 2018; Hagemeier 2018).
Multimodal analgesia, which targets numerous pain pathways, is now standard of care to reduce opioid consumption while controlling pain after TKA (Wainwright et al. 2020; Li, Ma, and Xiao 2019; Elmallah et al. 2018). Analgesia modalities recommended for use in patients undergoing TKA include neuraxial anesthesia, local infiltration analgesia, nerve blocks, and oral analgesics of different classes and with different modes of action (Wainwright et al. 2020). In addition, cryoneurolysis administered approximately 5 days before TKA has been shown to significantly reduce post-operative opioid use (Dasa et al. 2016; Mihalko et al. 2021).
The purpose of this pilot case series is to examine whether a multimodal analgesia regimen can eliminate the need for opioid use after hospital discharge in 40 consecutively treated TKA patients while adequately controlling pain during the first 3 months after surgery. We hypothesize that the majority of patients will not require opioids after discharge and that patients using opioids before surgery will be least likely to achieve an opioid-free TKA, as preoperative opioid use is the strongest predictor of opioid requirements after surgery (Hernandez et al. 2018).
METHODS
This is a retrospective case series of 40 consecutive patients who underwent primary unilateral TKA by a single fellowship-trained orthopedic surgeon practicing at an academic community hospital between May and October 2020. Patients who had undergone TKA for the contralateral joint were excluded. Surgery for all patients consisted of navigated TKA using Zimmer Biomet Persona or Zimmer Biomet Nex Gen implants. The study was approved by the site’s institutional review board.
The multimodal analgesia regimen utilized was part of an enhanced recovery after surgery protocol and was developed over time based on evidence and the surgeon’s clinical experience. Approximately five days prior to surgery, patients underwent percutaneous cryoneurolysis following local anesthesia with lidocaine. The operating surgeon (VD) or his designee performed cryoneurolysis in all cases. Cryoneurolysis is the nonpermanent treatment of peripheral nerves with temperatures below-20°C (Pacira CryoTech Inc. 2019), which causes Wallerian degeneration of the nerve axons (Zhou et al. 1995), resulting in a long-acting nerve block (Barnard 1980). Cryoneurolysis was administered using the handheld iovera° device (Pacira Cryotech, Fremont, CA, USA). Nitrous oxide flows from a disposable cartridge through the handpiece to an assembly of three 27-gauge closed-end needles. As the nitrous oxide enters the needles, a highly localized cold zone is formed via the Joule-Thompson effect. Nothing is injected in the body and the nitrous oxide gas is vented safely out of the handpiece.
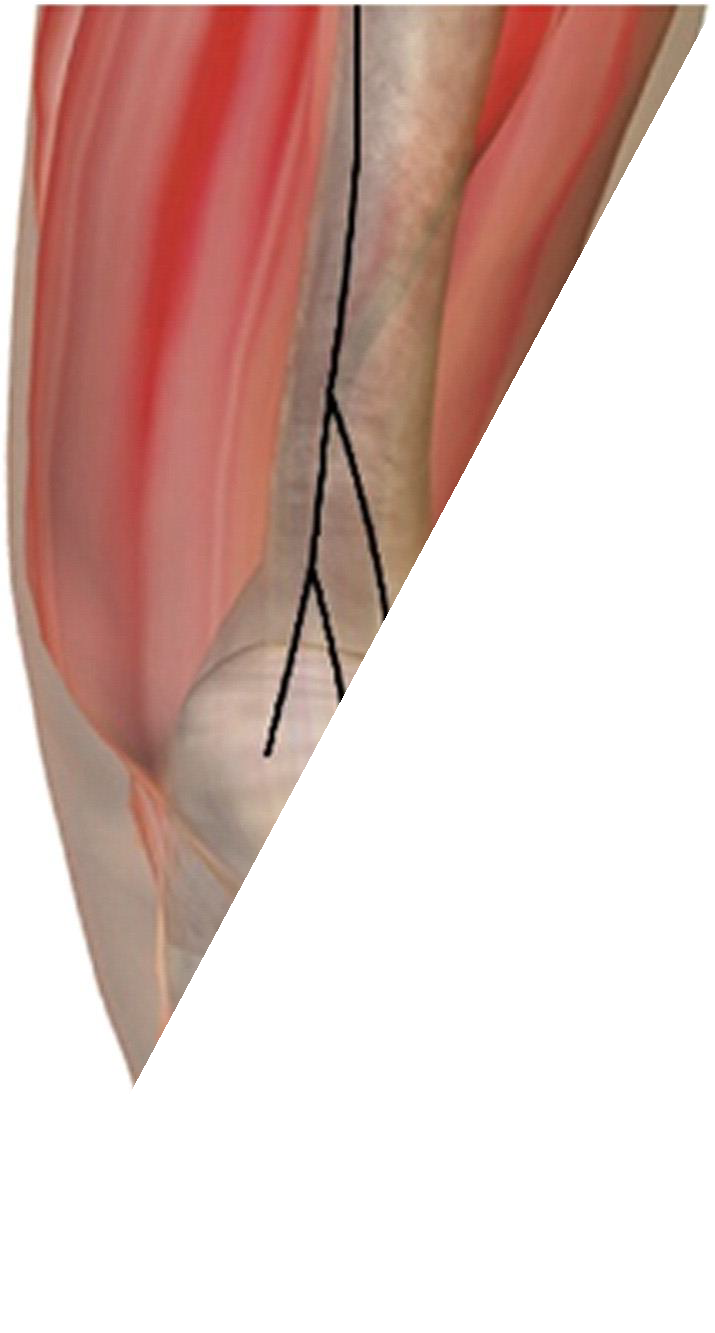
Cryoneurolysis targeted the superficial geniculate nerves, the anterior femoral cutaneous nerve (AFCN) and infrapatellar branch of the saphenous nerve (ISN), which lie in a predictable and superficial location as they approach the knee and provide sensory innervation around the anterior knee with no motor involvement (Horner and Dellon 1994). The AFCN was targeted approximately 70 mm above the superior pole of the patella along a horizontal line the width of the patella (Figure 1A). The ISN was targeted approximately 50 mm medial to the patella tendon (Figure 1B) along a longitudinal line from the inferior pole of the patella and tibial tubercle.
_treatment_line_(a)_and_infrapatellar_branches_of_t.png)
Using these anatomical landmarks, treatment lines were drawn on the patient’s knee. A treatment cycle consists of a period of cooling then warming of the needles, lasting approximately 50 seconds. Once a treatment cycle was complete, the needles were introduced along the next section of the treatment line. Each line required approximately six treatment cycles to cover the length of the treatment line.
At the hospital immediately before surgery, patients received a single dose of 150 milligram (mg) pregabalin, 200 mg celecoxib, and 1000 mg intravenous (IV) acetaminophen. In addition, an anesthesiologist performed a neuraxial (spinal) with 1.6 mg of 0.75% bupivacaine (and occasional IV fentanyl depending on the anesthesia provider), a regional adductor canal block (ACB) and interspace between the popliteal artery and capsule of the posterior knee (IPACK) block with liposomal bupivacaine (Exparel; Pacira Pharmaceuticals, Inc, San Diego, CA, USA). Intraoperatively, patients received a periarticular infiltration of 0.25% bupivacaine hydrochloride (Marcaine). Following surgery, patients who remained overnight in the hospital were given 75 mg pregabalin twice a day, 200 mg celecoxib twice a day, and 650 mg of acetaminophen every 6 hours. If additional pain relief was needed prior to discharge, patients would typically receive hydromorphone 1 mg as needed. Upon discharge home, patients were instructed to take 325 mg acetaminophen every four hours for two weeks and 75 mg diclofenac twice a day for 6 weeks. Patients were not prescribed opioids at discharge but could receive a prescription if they contacted the surgeon and reported uncontrolled pain. If requested by the patient, the initial opioid prescription─ oxycodone 5 mg every 12 hours for 2 weeks — was intended to provide breakthrough pain relief while ensuring that narcotics were used sparingly. Residents were not permitted to prescribe narcotics during call hours and all inquiries for pain during business hours were routed to the attending surgeon.
Data derived from patient medical records included demographics (age, sex, race, surgery date, and type of insurance) and clinical information (body mass index [BMI], length of stay [LOS]). All opioid use during the 3 months before and after TKA was determined by examining the Louisiana Prescription Monitoring Program (PMP) database. Opioid-naïve patients were defined as those who had no opioid prescription filled in the 3 months prior to TKA and opioid- experienced patients as those who had at least one opioid prescription filled during the three months before TKA.
Pain control was assessed using the Pain Intensity item from the PROMIS-29® (Patient- Reported Outcomes Measurement Information System®), which is assessed on a 0-10 numerical rating scale, and the Knee Osteoarthritis and Outcomes Score (KOOS) Pain subscale score, which has a range of 0 (no problems) to 100 (extreme problems); both questionnaires were administered immediately prior to surgery and two weeks and three months after surgery. Data were managed using REDCap and analyzed using SAS version 9.4 (SAS Institute Inc, Cary, NC, USA). Analyses were predominately descriptive in nature.
RESULTS
Patients
The sample was predominately female (72.5%) and white (55%) with an average age of 65 years (Table 1). Among the 40 patients, 32 (80%) had not filled an opioid prescription during the three months prior to TKA (opioid naïve) and 8 (20%) had filled at least one opioid prescription within three months prior to TKA (opioid experienced). Seven of the eight patients with preoperative opioid use had received their prescription from a physician other than the operating surgeon.
Thirteen patients (five opioid naïve and eight opioid experienced) did not receive preoperative cryoneurolysis because the procedure was not approved by their insurer. The majority of patients (62.5%; n=25) were discharged from the hospital on the same day as their surgery; 35% (n=14) spent one night and 2.5% (n=1) two nights in the hospital after TKA.
Opioid Use Following TKA
Two thirds of patients (67.5%; n=27) were able to recover from TKA without using oral opioids. Whereas all 8 (100%) of the experienced opioid users required opioids after TKA, only 5 of 32 (15.6%) opioid-naïve patients required postoperative opioids (Table 2). Opioid-experienced patients had a higher mean number of post-TKA opioid prescriptions (3.1 vs. 1.6) and mean total morphine milligram equivalent (985 vs. 265) than opioid-naïve patients. Among the 32 opioid- naïve patients, 3 of the 9 (33%) who did not receive cryoneurolysis required opioids after TKA compared with only 2 of the 23 (8.7%) who received cryoneurolysis.
Pain After TKA
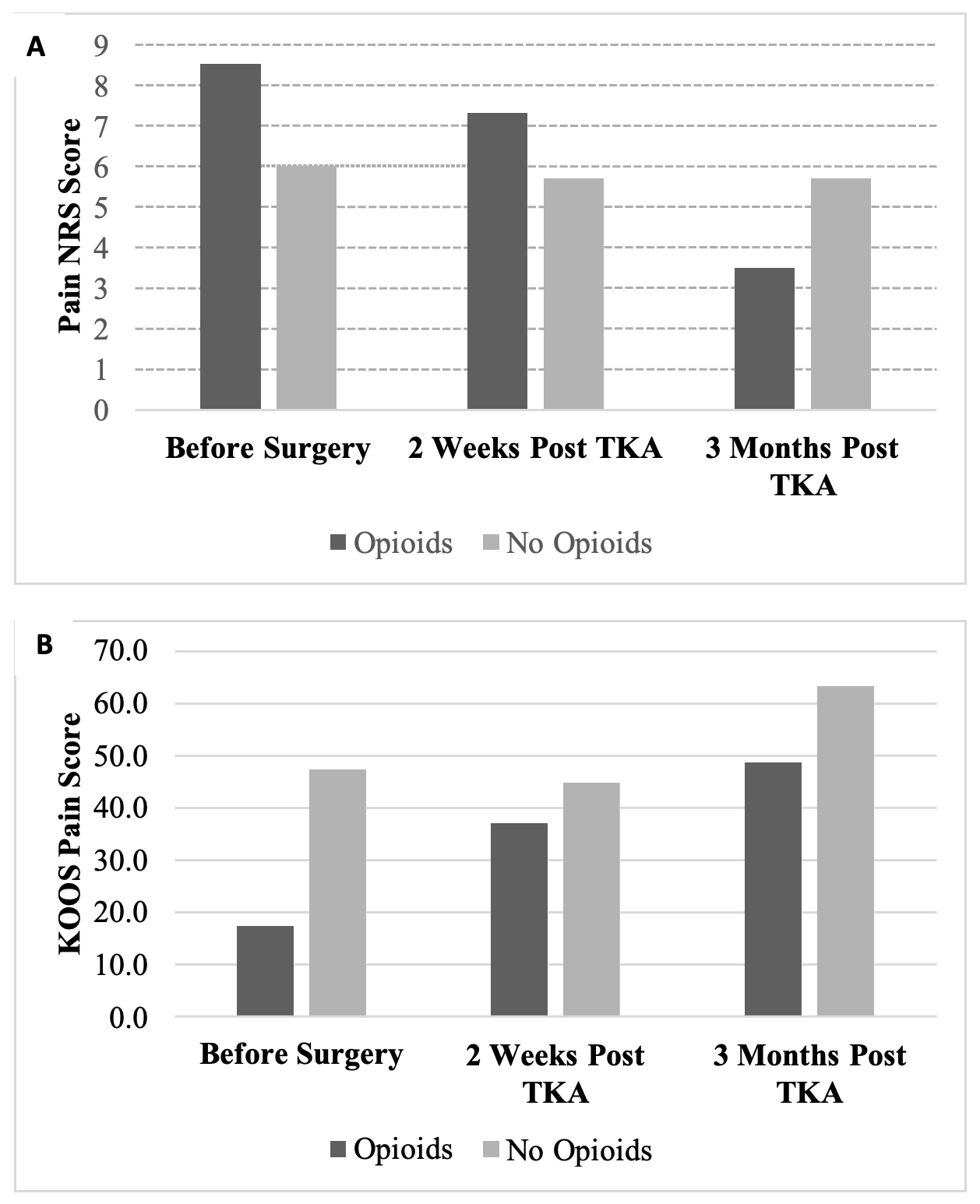
Pain improved from before surgery to three months post-surgery (Figure 2A and 2B). Although pain scores improved over time for all patients, patients who used opioids after TKA reported higher levels of pain at each time point compared with those who had an opioid-free TKA.
_score_(a)_and_koos_pain_subscale_score_(b)_over_time_by_.png)
DISCUSSION
In this pilot study, we describe outcomes of an opioid-free multimodal pain regimen applied to a series of 40 consecutively treated TKA patients. Utilization of a comprehensive regional and multimodal analgesia regimen targeting distinct pain pathways resulted in opioid-free TKA for two thirds of all patients and 80% of opioid-naïve patients. Further, patients who achieved an opioid-free TKA reported lower levels of pain at all time points than patients who required opioids after TKA. Consistent with other studies that have found preoperative opioid use to be predictive of higher opioid use following TKA (Goesling et al. 2016; Rozell et al. 2017), in this cohort, patients’ recent history of opioid use was prognostic of whether they were able to tolerate post-surgical pain without opioids: 100% of opioid-experienced patients required opioids after TKA compared with only 16% of opioid-naïve patients.
The results of this study provide additional support for the effectiveness of multimodal analgesia that addresses different pain pathways. In the present study, 13 of 40 patients did not receive preoperative cryoneurolysis because their insurer did not approve the procedure, allowing for comparison with patients who received this intervention. Within the opioid-naïve group, 33% who did not receive cryoneurolysis required opioids after surgery compared with only 9% of patients treated with preoperative cryoneurolysis. Similarly, in a retrospective cohort study, Dasa et al. reported that preoperative cryoneurolysis was associated with a shorter hospital length of stay and 45% reduction in opioid consumption during the first 12 weeks after TKA (Dasa et al. 2016). Together, these findings suggest that preoperative cryoneurolysis is an important component of pain relief during the first 3 months after TKA.
All patients received a protocol consisted of neuraxial analgesia, an ACB, and local infiltration of liposomal bupivacaine as well as an intraoperative periarticular injection of bupivacaine hydrochloride. Consensus guidelines recommend neuraxial analgesia over general anesthesia for routine TKA patients to reduce the risk of complications (Memtsoudis et al. 2019). Additionally, randomized controlled trials have shown that the combination of ACB and local infiltration of liposomal bupivacaine as well as the combination of ACB and periarticular injection synergistically promote better pain control and less opioid consumption after TKA (Zuo et al. 2019; Kim et al. 2019). Finally, multimodal oral analgesia, prescribed following hospital discharge in the present study, has been previously shown to reduce opioid consumption, minimize opioid-related side effects, and improve pain control (Golladay et al. 2017).
This pilot study was intended to demonstrate that opioid-free TKA was possible; however, results indicate that the majority of patients who used opioids during the 3 months prior to TKA required opioids to control pain following TKA. How to mitigate prolonged opioid use after TKA for this highest risk subgroup remains an area ripe for investigation. Several recent papers have described success in reducing opioid consumption during the first 6 postoperative weeks by utilizing patient-specific opioid- tapering protocols after total hip arthroplasty and spine surgery (Joo et al. 2020; Tamboli et al. 2020). However, it is unclear whether these reductions will be sustained and what proportion of patient may attain opioid-free status.
The main limitations of this case series are the small sample size and involvement of a single surgeon practicing at one institution. The small sample size resulted in insufficient power to make meaningful statistical comparisons between patient subgroups (e.g., opioid naïve vs experienced, cryoneurolysis vs no cryoneurolysis). Treatment of patients by a single orthopedic surgeon limits the generalizability of findings. Although retrospective studies may be prone to selective bias, patients selected for this case series were consecutively treated using the same pain protocol. Although the sample was racially diverse, only a small proportion of patients had
Medicaid insurance, suggesting that patients with lower income and other socioeconomic disadvantages may have been underrepresented. In a previous study, both black race and Medicaid insurance were risk factors for prolonged opioid use among opioid-naïve adult orthopedic patients (Lanzillotta-Rangeley et al. 2020). A strength of the study was the access to the statewide PMP database which captured all filled narcotic prescriptions. Thus, filled opioid prescriptions written by the treating surgeon as well as other providers were able to be captured. We note, however, that this study captured only prescribed and not consumed opioids. It may be possible that some proportion of patients had excess opioid pills from their initial discharge and/or refill opioid prescriptions.
CONCLUSIONS
In conclusion, although there is no consensus about the optimal multimodal pain protocol for use in TKA, a growing body of evidence indicates that modalities that target a variety of pain pathways can produce additive or synergistic benefits. Given the well-known costs of prescription opioids, orthopedic surgeons should seek to use the full range of available tools to reduce pain, promote recovery, and minimize opioid consumption after TKA. We are collecting data for publication of a larger case series with a longer follow-up to demonstrate that the multimodal pain protocol utilized in the current study yields robust results. Future research should seek to determine which elements of the protocol are most essential for effectively managing pain and minimizing opioid use after TKA and investigate novel approaches to achieving opioid-free status in TKA patients who receive preoperative opioids
Funding
No funding was received for this study.
Conflicts of Interest
Dr. Dasa is a paid speaker for Bioventus, Swiftpath, and Pacira; consultant for Bioventus and Pacira; owns stock or stock options in SIGHT Medical, My Medical Images, and Goldfinch Health; and has received research support from SKK, Cartiheal and OREF. The other authors have no competing interests to disclose.