



The What
Slipped Capital Femoral Epiphysis (SCFE) is a well-known disorder of the adolescent hip that is typically caused by abnormal loading through the joint. This condition, often seen in patients with endocrinopathies, is typically treated with in situ pinning of the slipped hip. There remains, however, significant debate regarding the need and indications for prophylactic pinning of an unslipped hip, which is of increased importance given the typical unilateral presentation of this condition.

The Why
SCFE primarily affects obese males and has an incidence of 10-11 per 100,000 in the U.S., with this rate likely rising as a result of increasing obesity. The goal of prophylactic pinning is to prevent a future slip and subsequent sequelae such as avascular necrosis and chondrolysis of the femoral head. It is advocated for individuals at high risk for slip or individuals at risk for delayed presentation.
An important aspect of this decision making is the potential for anatomic changes to the proximal femur as a result of this prophylactic pinning, especially given that the individuals who undergo this procedure often have significant remaining osseous growth potential. Currently, there is little known regarding the implications of prophylactic pinning on proximal femur growth.
The How
The purpose of our study was to characterize the relationship between prophylactic pinning and proximal femur growth. Our hypothesis was that we would see an increased height of the greater trochanter relative to the center of the femoral head and a shortened femoral neck as a result of prophylactic pinning.
We reviewed data from patients at our institution from 2009-2015, including in our final analysis patients that had not previously undergone hip surgery, those who underwent pre-and postoperative AP radiographs, and those who had a unilateral slip at their initial presentation. Our team undertook a matched analysis based on prophylactic pinning status, which ultimately gave us two groups: one that underwent prophylactic pinning and one that did not. A variety of anatomic radiographic measurements on anteroposterior radiographs were then obtained to accurately characterize proximal femur growth in this cohort.

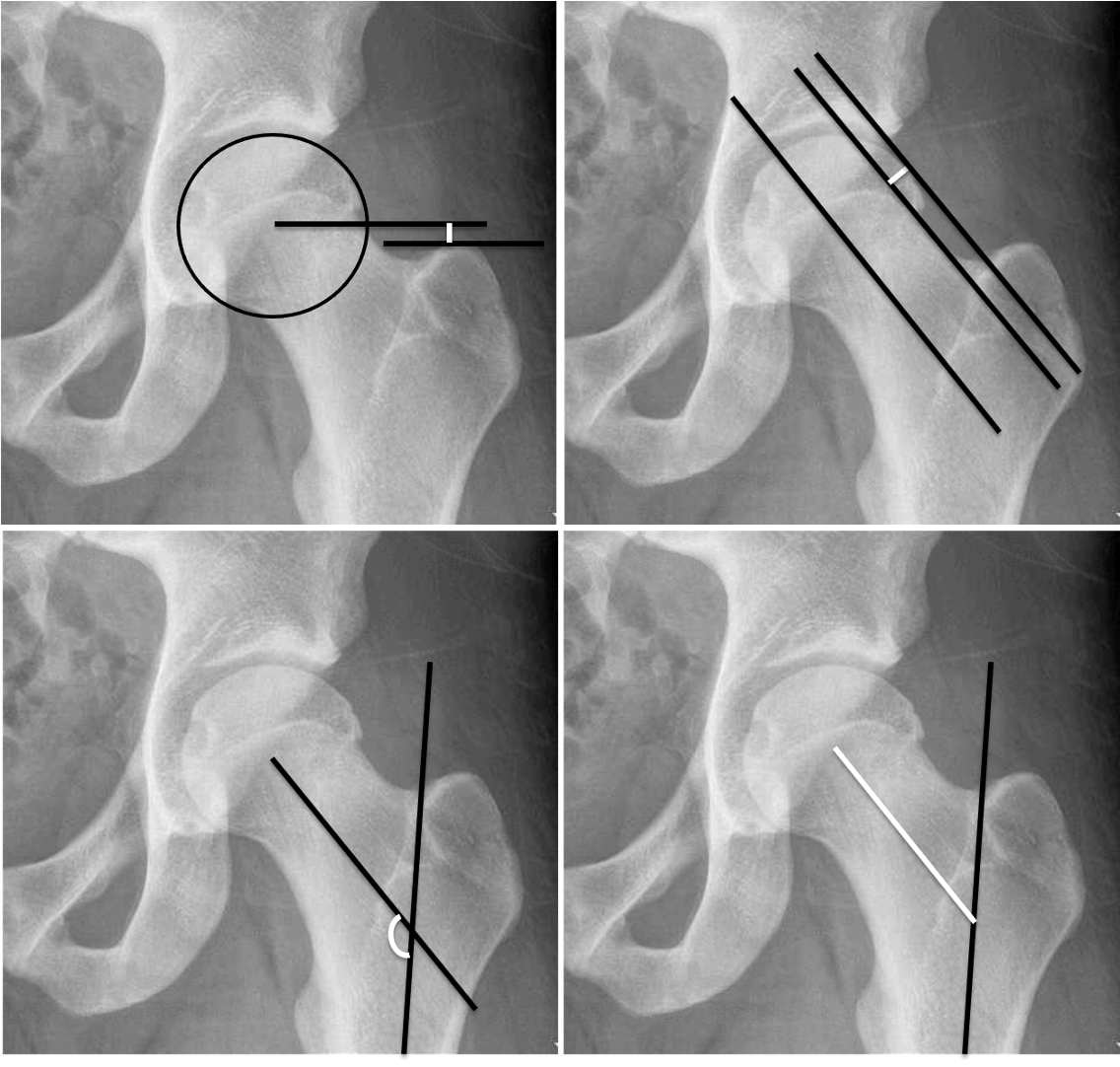
The white lines in each panel designate the actual measurement that was obtained. In the upper left there is an assessment of the height of the greater trochanter relative to the center of the femoral head; this was assessed by using a best-fit circle over the femoral head and extending a line parallel, with the distance measured between this line and a second parallel line at the apex of the greater trochanter. In the upper right we have the femoral head-neck offset, which was assessed by drawing three lines: one along the axis of the femoral neck, a parallel line on the lateral aspect of the femoral neck, and a third parallel line on the most superolateral aspect of the femoral head, with the distance calculated between the second and third lines to assess offset.
The bottom left panel demonstrates the femoral neck shaft angle, obtained by drawing intersecting lines along the axes of the femoral neck and femoral shaft and calculating the resultant angle. The bottom right panel demonstrates the measurement of femoral neck length; this measurement was obtained by drawing a straight line along the axis of the femoral neck from the center of the femoral head until it intersected with a line along the axis of the femoral shaft.
Our statistical analysis utilized the delta difference in these measurements from initial presentation to final follow up. We utilized a combination of independent samples t-tests and multivariable logistic regression to characterize the association of prophylactic pinning with proximal femur growth.
The Results
We demonstrated significant differences between our prophylactic pinning and no prophylactic pinning groups with our independent samples t-tests. We demonstrated a significantly increased greater trochanter height in the prophylactic pinning group, in addition to a significantly decreased femoral head-neck offset and femoral neck length.

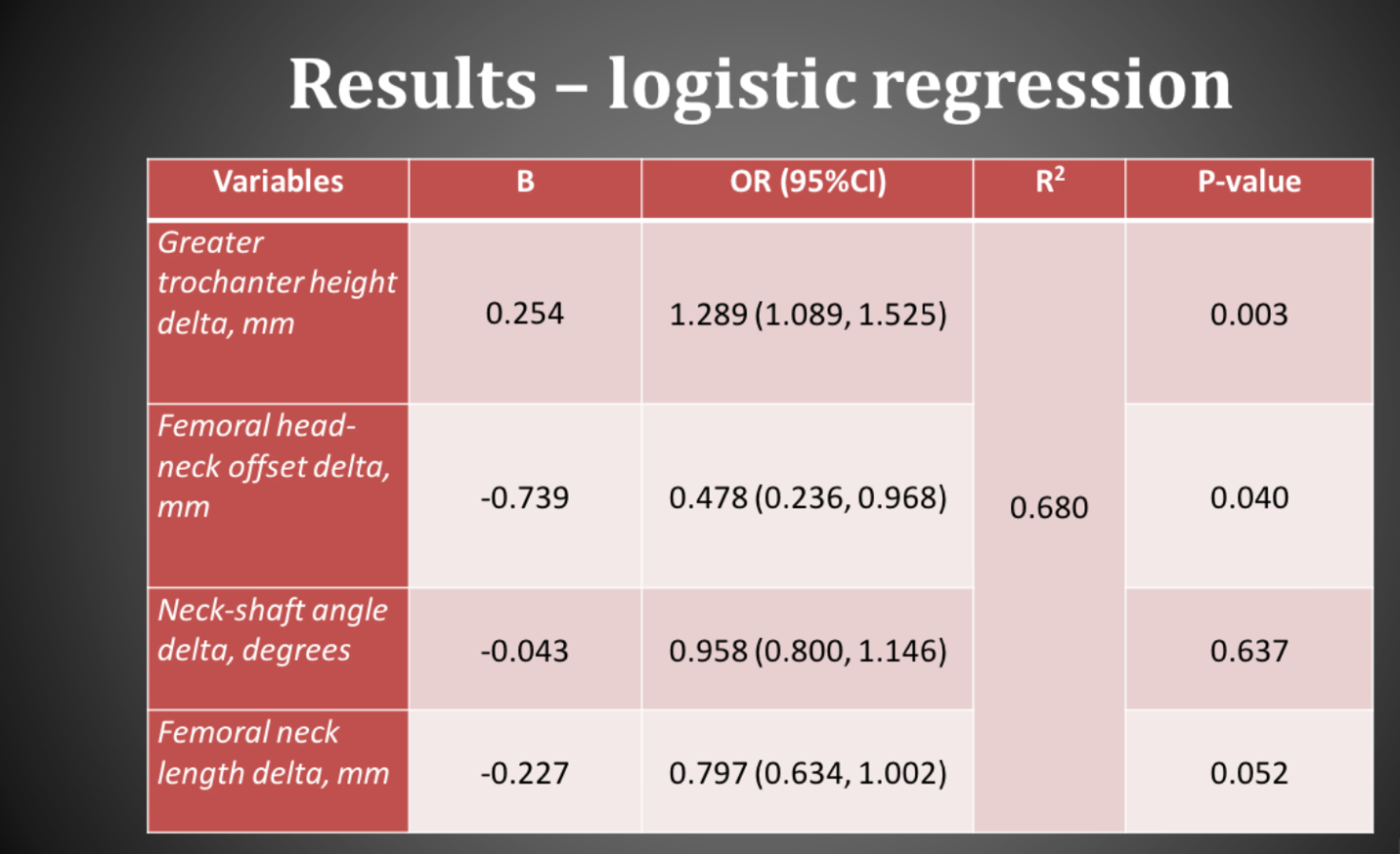
Here we have the results of our logistic regression, showing much of the same findings we observed with our comparison of the means. In the prophylactic pinning group, there is an association with an increased greater trochanter height, and also associations with loss of the femoral head-neck offset and borderline statistical significance with a reduced femoral neck length.

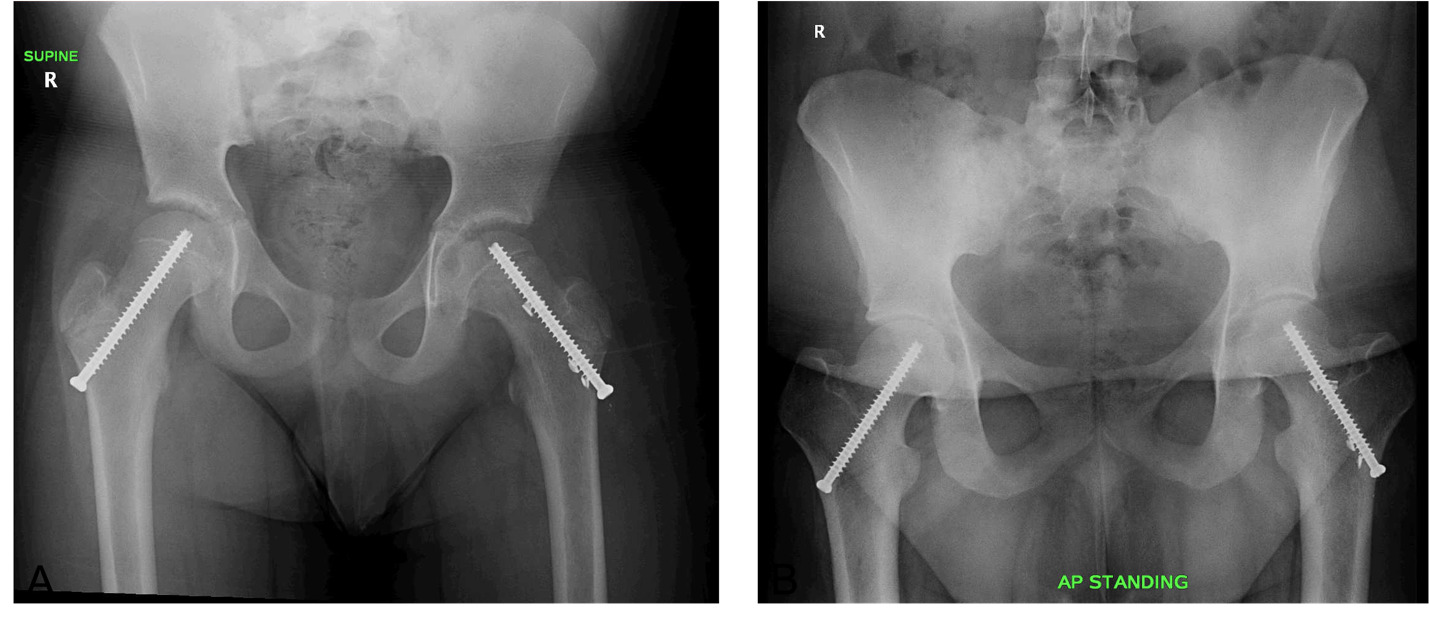
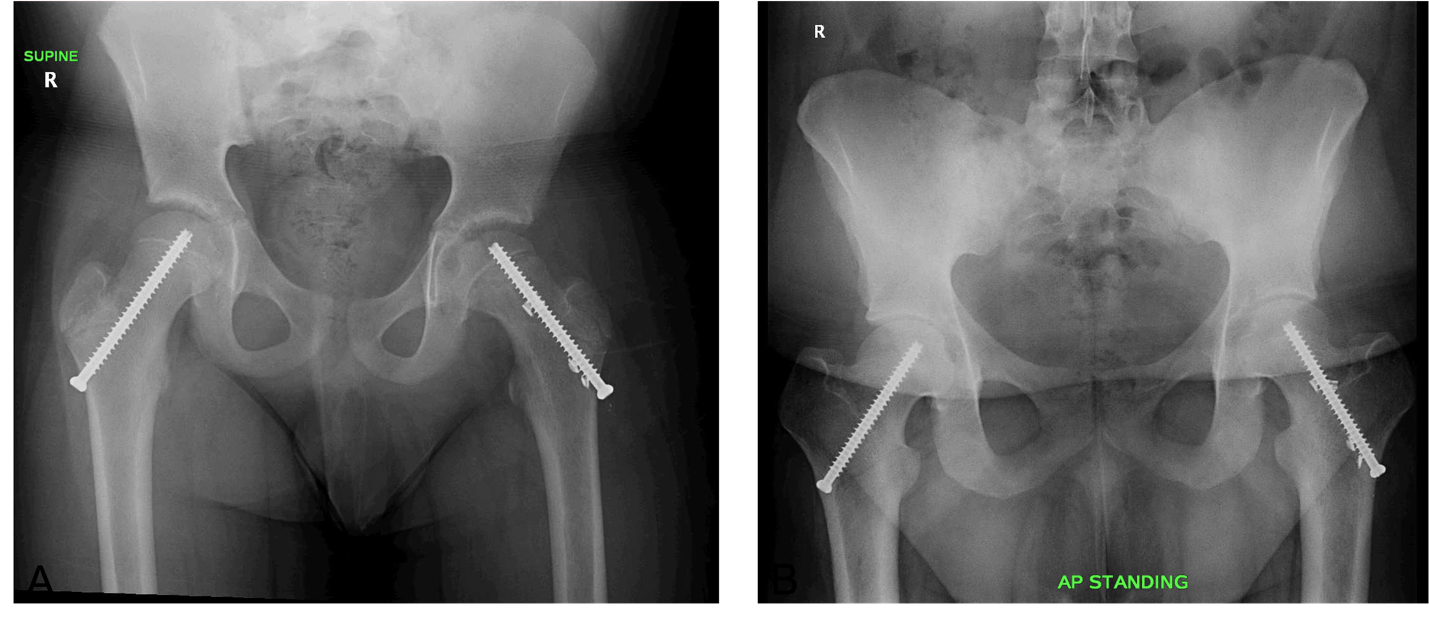
Here we have an individual who underwent prophylactic pinning, the left image showing the individual immediately following initial pinning with the final follow up on the right. This is a left-sided SCFE that underwent in situ pinning and was subsequently prophylactically pinned on the right side. When comparing the right proximal femur at these two timepoints, there is a relative loss of femoral neck length and femoral head-neck offset, in addition to an increase superiorly in the relative position of the greater trochanter to the center of the femoral head.

This individual demonstrates marked loss of femoral head-neck offset and extreme shortening of the femoral neck, in addition to significant superior displacement of the greater trochanter relative to the center of the femoral head.

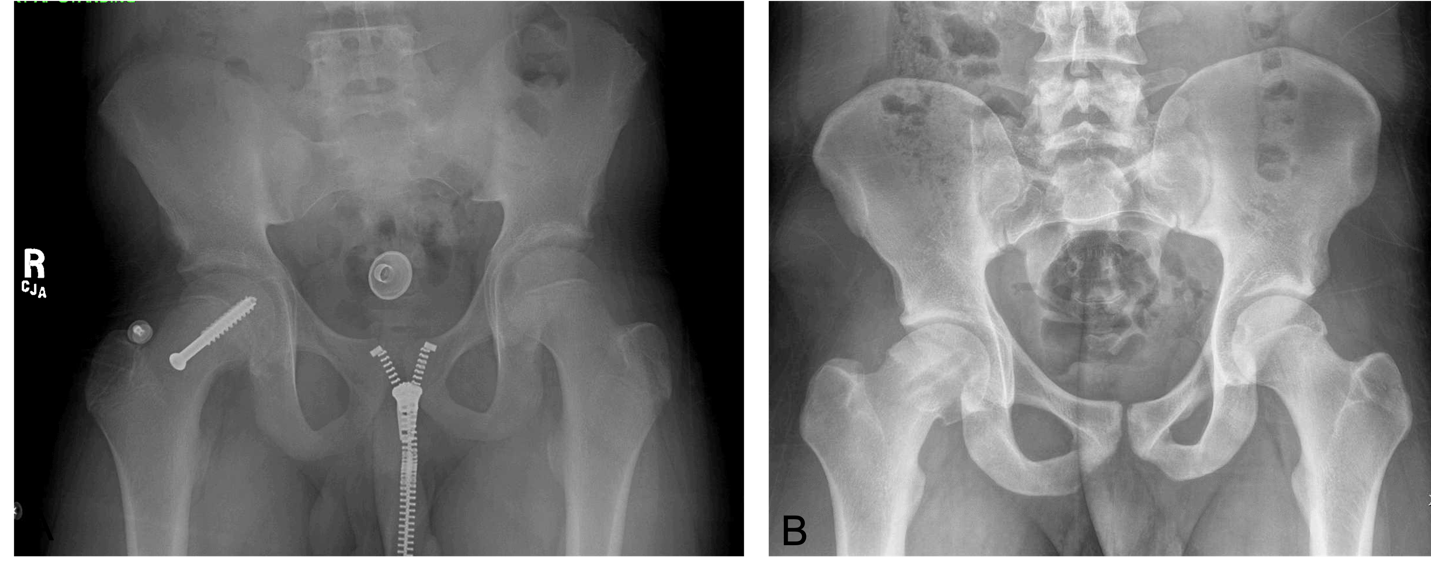
In this individual, who did not undergo prophylactic pinning, the left film shows the patient immediately following initial pinning, while the right film shows the final follow up. When comparing the left proximal femur at these two timepoints, it is evident that there is preserved proximal femoral anatomy between these two time points, with relative preservation of the femoral head-neck offset, femoral neck length, and positioning of the greater trochanter relative to the center of the femoral head.

In conclusion, our study demonstrates that significant proximal femoral morphologic changes are associated with prophylactic pinning in patients treated for a unilateral SCFE, which must be taken into account when considering prophylactic pinning in this population. Prophylactic pinning should be considered an independent risk factor for femoral morphologic changes when compared to the risk of subsequent slips. In addition, there are potential biomechanical implications due to anatomic disruption and its influence on hip functioning. There is also the potential need for revision surgery, especially from the perspective of cam lesion formations, which is shown here in the image of a left-sided prophylactically pinned patient who subsequently developed a fairly significant cam lesion that may need to be revised as a result of the pinning.