Introduction
Burnout is a syndrome characterized by emotional exhaustion, depersonalization, and reduced personal accomplishment in the work environment (Maslach et al. 1997; Maslach, Schaufeli, and Leiter 2001). In 2010, Shanafelt et al. conducted a survey of United States (US) physicians using the Maslach Burnout Inventory (MBI) and found that more physicians were burnt out (38%) when compared with the general US population (28%) (Shanafelt et al. 2010). Arora et al. conducted a systematic review of orthopaedic residents and faculty in 2013 and reported a burnout rate of 50–60% (Arora, Diwan, and Harris 2013). Burnout has been associated with decreased productivity, impedance of personal fulfillment, decreases in patient safety, and increases in medical errors (Shanafelt et al. 2010; Firth-Cozens and Greenhalgh 1997; West, Dyrbye, and Shanafelt 2018).
In December 2019, the first case of ‘severe acute respiratory syndrome coronavirus 2’ (SARS-CoV-2) was reported (Yang, Zhang, and Chen 2020). On January 30, 2020, the World Health Organization labelled the disease outbreak caused by coronavirus 2019 (COVID-19) an international public health emergency, and in March 2020 it was declared a pandemic (Stawicki et al. 2020). Healthcare workers battling this virus were faced with personal protective equipment shortages and morbidity and mortality of their colleagues, resulting in increased reports of emotional trauma, social isolation, depression, anxiety, and insomnia (Huang et al. 2020; West, Dyrbye, and Shanafelt 2018). In July 2020, Coleman et al. conducted a survey of American College of Surgeons (ACS) residents, fellows, and early career surgeons and found that 55% reported emotional exhaustion, 45% reported a decrease in sense of personal achievement, and 39% reported depersonalization related to the COVID-19 pandemic (Coleman, Abdelsattar, and Glocker 2021).
Women physicians and healthcare workers were disproportionately affected by the pandemic. The reduction in childcare services and school closures heightened the professional disadvantage that women face because they are more likely to carry a larger burden of household labor and caregiving (Allen et al. 2020; Higgins et al. 2021; Wenham, Smith, and Morgan 2020). Limited data are available to assess how orthopaedic surgeons have been affected by the COVID-19 pandemic, especially in regard to burnout symptoms.
The purpose of this study was to understand how the COVID-19 pandemic contributed to burnout syndrome as well as changing family and practice dynamics for practicing academic orthopaedic surgeons. We hypothesized that most practicing orthopaedic surgeons, especially female orthopaedic surgeons, would experience burnout syndrome due to changing practice dynamics and family dynamics caused by the COVID-19 pandemic.
Materials and Methods
Study Design and Setting
After obtaining approval from the Institutional Review Board at our institution, an anonymous 28-question online cross-sectional survey was distributed using convenience sampling to 2,002 academic orthopaedic surgeons listed by the American Academy of Orthopaedic Surgeons (AAOS) between February and April of 2021. Academic surgeon email information is private and can only be accessed by members of the AAOS. The survey was created and distributed using Qualtrics Software (Provo, Utah). Follow-up emails were sent 2 and 4 weeks after initial communication to encourage participation. The survey was open for three months, so as to minimize the risk of survey fatigue in our sample.
Variables Studied and Their Definitions
The first half of the survey consisted of questions from Kale et al. (2020), which asked about the effect of COVID-19 on orthopaedic surgeons’ practices and their personal well-being. Eight questions evaluated family dynamics during the pandemic such as time spent with family and household chores. Ten questions were related to respondent demographics. The outcome measure of this study, burnout syndrome, was measured using the MBI: Human Services Survey (MBI-HSS) scale (Maslach, Schaufeli, and Leiter 2001; Abu-Hilal and Salameh 1992), which is currently the most widely used validated measurement for evaluating burnout syndrome. License and permission from the authors of the questionnaire were obtained. The MBI-HSS has a high reliability and validity (Maslach, Schaufeli, and Leiter 2001; Wang et al. 2020b). The 22 MBI-HSS questions measure emotional exhaustion, depersonalization, and the feeling of reduced personal accomplishment (Table 1). Persons with high exhaustion and high depersonalization scores were defined as having burnout: the higher the score, the greater the degree of burnout (Maslach, Schaufeli, and Leiter 2001; Sahraian et al. 2008; Luan et al. 2017; Wang et al. 2020a).
Statistical Analysis
The anonymous survey data was downloaded from Qualtrics into SPSS Statistics 21 (IMB, Armonk, New York) for analysis. Mean and standard deviation (SD) were calculated for continuous variables, while percentages were analyzed for categorical thresholds. Analysis of variance (ANOVA) F-test comparison of score means and Fischer’s Least Significant Difference (LSD) post-hoc analysis were used to compare MBI-HSS scores using demographic variables and family dynamic questions to determine if there were any significant differences. Univariate analyses of categorical variables were assessed with Chi-square test. Dichotomous variables were assessed using Fischer’s exact test. A p value < 0.05 was considered statistically significant.
Results
Patient Demographics
A total of 2,025 emails were distributed and 23 could not be delivered. Blank or incomplete questionnaires (N=18) were excluded from data analysis. A total of 227 valid questionnaires (response rate: 11.3%) were analyzed with a respondent completion rate of 98%. The majority of surgeons were between ages 40–59 years (148 of 218, 68%), practiced academic medicine (191 of 217, 88%), and identified as male (164 of 227, 72%) and white (185 of 218, 85%). Most surgeons in the sample worked between 50–59 hours/week (60 of 217, 28%) and 60–69 hours/week (81 of 217, 37%), and were married (193 of 218, 89%) with children (209 of 227, 92%). A significant majority of single (12 of 13, 92%, p < 0.001) and childless (17 of 18, 94%, p < 0.001) respondents were female. Respondents practiced in all geographic locations across the United States, and all orthopaedic specialties were represented (Table 2).
Demographic Differences in Burnout Syndrome
Within our sample, a majority of participants (155 of 227, 68%) showed burnout based on the MBI-HSS (i.e., high scores on the emotional exhaustion and/or depersonalization scales). Burnout prevalence was significantly higher in surgeons between the ages of 40–59 compared to older surgeons (73% vs. 13%, p = 0.002) and surgeons early in practice compared to those practicing for 31+ years (32% vs. 7%, p = 0.002) (Table 3).
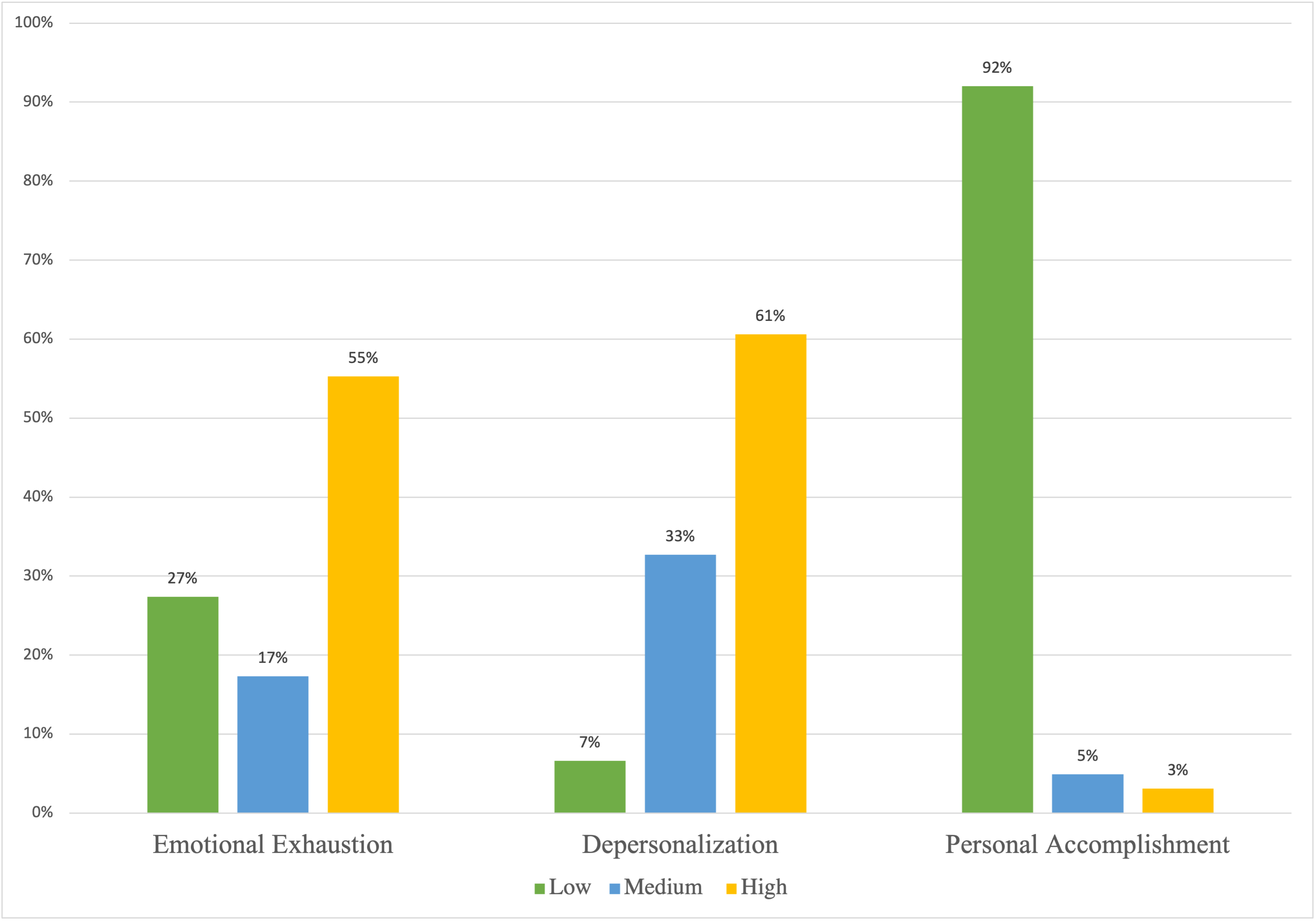
The mean scores of each MBI-HSS for all surgeons showed high levels of emotional exhaustion (30.0 ± 13.7), depersonalization (12.1 ± 6.4), and personal accomplishment (49.0 ± 6.3). When stratified into low, medium, and high scores, most surgeons in the sample had high levels of emotional exhaustion (55%), depersonalization (61%), and personal accomplishment (92%) (Figure 1, Table 4).
_for_orthopaedic_surgeons.png)
Emotional Exhaustion
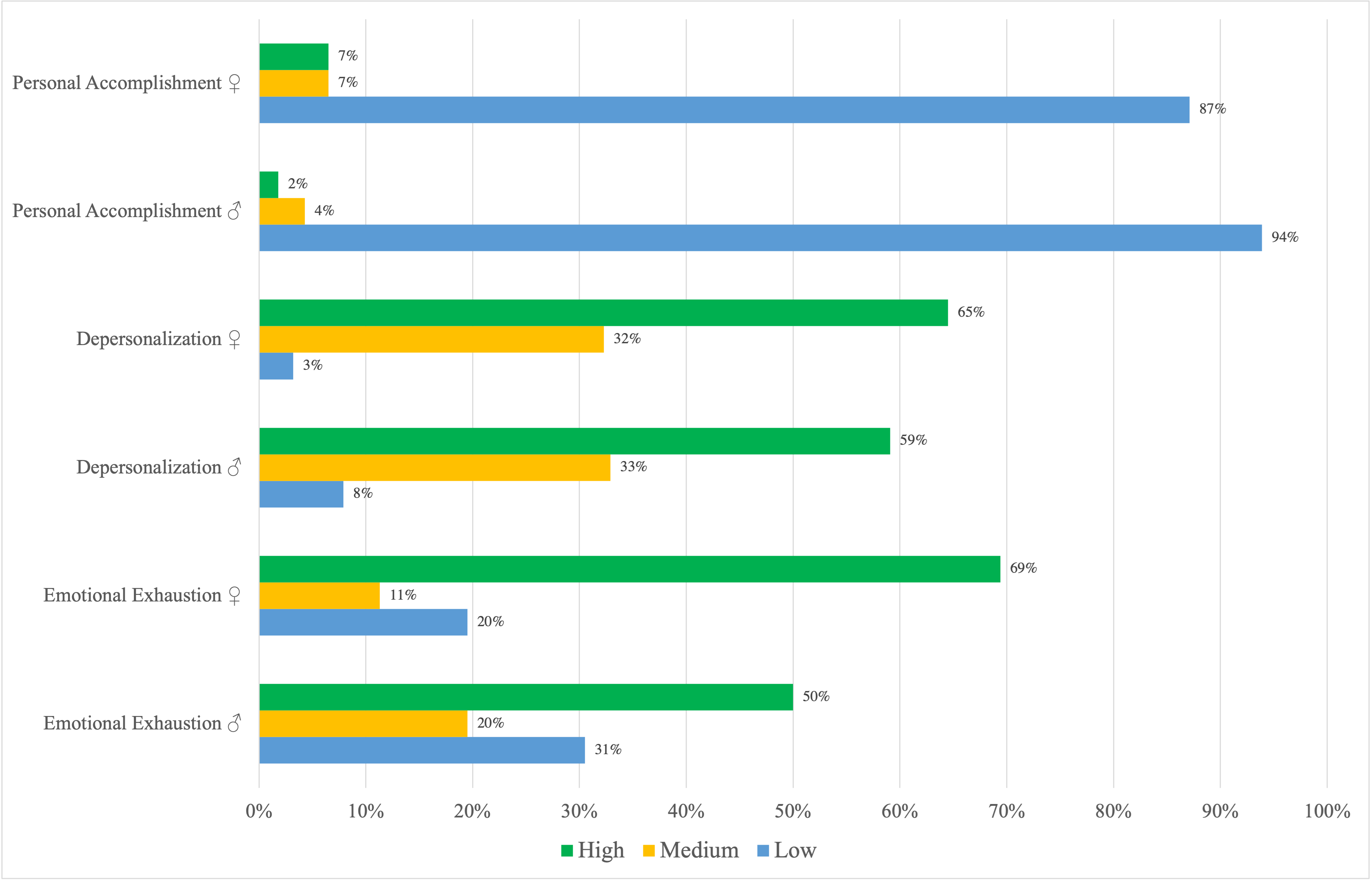
Emotional exhaustion measured by the MBI-HSS differed significantly in age, gender, years of practice, geographic location, marital status, and whether participants had children. Surgeons between 20–29 and 40–59 years old (31.5 ± 14.4, p = 0.004 and 32.5 ± 13.4, p < 0.001, respectively) had higher scores compared to those > 60 years old (22.3 ± 11.0). Those in practice for 5–10 years (32.6 ± 14.4) and 11–20 years (33.2 ± 13.1) had higher scores compared to those in practice for 31+ years (20.4 ± 9.6, all p < 0.001). Surgeons from the West had higher scores compared to those from the Southwest (p = 0.011). Single surgeons (92% female) had higher scores (40.6 ± 13.5) than married surgeons (29.5 ± 13.4, p = 0.024 [1.1, 21.1])). Surgeons who did not have children (94% female) (38.4 ± 16.0) had significantly higher scores than those who did (29.2 ± 13.3, p = 0.006). Female surgeons (34.4 ± 14.4) had higher mean emotional exhaustion scores than male surgeons (28.2 ± 13.1, p = 0.002). When stratified into low, medium, and high scores, a greater proportion of female surgeons had significantly higher emotional exhaustion and depersonalization scores compared to male surgeons (Figure 2).
_for_female_and_male_orthopa.png)
Depersonalization
Depersonalization scores differed significantly based on age, years of practice, geographic location, and whether participants had children. Younger surgeons (20–29 and 40–59 years old) (14.0 ± 7.1, p = 0.004 and 12.7 ± 6.5, p = 0.003, respectively) had higher scores compared to those greater than 60 years old (9.4 ± 4.6). Those who were in practice for 5–10 and 11–20 years (14.1 ± 7.5, p = 0.001 and 13.6 ± 6.7, p = 0.003, respectively) had higher scores compared to those in practice for 31+ years (8.6 ± 3.5). Surgeons from the West (35.0 ± 12.3) had higher scores compared to those from the Southwest (20.7 ± 8.7, p = 0.003). Surgeons without children (16.1 ± 7.6) had significantly higher depersonalization scores than surgeons with children (11.7 ± 6.1, p = 0.005).
Personal Accomplishment
Feelings of personal accomplishment differed significantly based on age and years of practice. Surgeons > 60 years of age (50.4 ± 5.3, p = 0.008) had significantly more feelings of personal accomplishment than surgeons between the ages of 20–39 (46.4 ± 7.3). Surgeons who were in practice for longer (>31 years) (50.8 ± 5.0) had significantly more feelings of personal accomplishment compared to surgeons in practice for 5–10 years (46.7 ± 7.1, p = 0.004) (Table 5).
Impact of COVID-19 Pandemic on Burnout Syndrome
The majority of the sample reported that COVID-19 impacted their practice by stopping or delaying elective surgery (N=216, 95%). A greater proportion of surgeons who reported delay in advancement in tenure/partnership showed burnout based on the MBI-HSS (14 of 15, p = 0.014). The prevalence of burnout was significantly higher among surgeons who reported that the COVID-19 pandemic had an impact on their personal and mental well-being (123 of 154, p = < 0.001). Significantly more surgeons who indicated that, because of the COVID-19 pandemic, they were under financial distress (17 of 18, p = 0.015), mental/emotional distress (85 of 100, p < 0.001), had deteriorating home situations (37 of 39, p < 0.001), and had to change their practice dynamics (52 of 62, p = 0.002) had burnout based on the MBI-HSS (Table 6).
Impact of Changing Family Dynamics on Burnout Syndrome
A large proportion of the sample indicated that their spouse/partner performed childcare (N=88, 44%) and household care duties (N=112, 51%). Significantly more male surgeons (N=98, 62%) relied on their spouses for household chores than female surgeons (N=13, 22%, p < 0.001). Significantly more female surgeons (25 of 37, 68%) reported doing household chores themselves compared to male surgeons (12 of 37, 32%, p < 0.001). In addition, significantly more male surgeons relied on their spouses for childcare (N=76, 49%) than female surgeons (N=11, 16%, p < 0.001), who relied more on outside help (M vs. F outside help: 3.8% vs. 18.6%, p < 0.001). Across the sample, the time spent on household chores (51%) and caring for children (49%) since the onset of COVID-19 increased, with no significant differences between genders. Surgeons who completed household chores (35.4 ± 14.2) had higher emotional exhaustion scores than those who relied on their spouses (30 ± 12.2, p = 0.009). Surgeons who spent a decreased amount of time on household chores since the onset of the COVID-19 pandemic had higher emotional exhaustion scores than those who spent an increased or the same amount of time (p = 0.018 and p = 0.019, respectively). Surgeons whose employers did not change policies to allow more flexibility during the pandemic had higher emotional exhaustion scores (33.4 ± 13.9 vs. 28.1 ± 13.2, p = 0.005) and higher feelings of reduced personal accomplishment (47.7 ± 6.8 vs. 49.9 ± 5.5, p = 0.01) (Table 7).
Discussion
Physician burnout has been shown to cause increased medical errors (Shanafelt et al. 2010), decreased patient satisfaction and safety (Garcia et al. 2019), and deterioration of surgeon mental health and interpersonal relationships (Sargent et al. 2012). The COVID-19 pandemic has impacted healthcare in innumerable ways, including the re-allocation of resources (Meneghini 2020), cancelling of elective procedures (Congiusta et al. 2020), and negatively impacting physician’s mental and physical health (Huang et al. 2020). The present study investigated burnout among academic orthopaedic surgeons and the contributing role of the COVID-19 pandemic, and found that orthopaedic surgeons experienced high levels of burnout. Younger, more inexperienced, and female surgeons, especially childless and unmarried female surgeons, experienced more emotional exhaustion and depersonalization.
Previous studies have confirmed that orthopaedic surgeons are susceptible to emotional exhaustion and depersonalization (Ames et al. 2017; Daniels, DePasse, and Kamal 2016; van Wulfften Palthe et al. 2016; Travers 2020; Arora, Diwan, and Harris 2013). In 2009, Sargent et al. found that 28.4% of faculty members exhibited burnout as defined by high scores on emotional exhaustion and/or depersonalization scales (Sargent et al. 2009). Verret et al. surveyed orthopaedic surgeons at their institution and found that burnout was most strongly associated with increasing workload and decreasing job control in orthopaedic residents and attending surgeons and with a decreasing sense of fairness and poorer sense of community among fellows (Verret et al. 2021). Studies performed prior to the COVID-19 pandemic, such as Balch et al., have found that orthopaedic surgeons have lower burnout rates than other surgical subspecialties such as trauma or vascular surgery (Balch et al. 2011). This study, which was distributed during the COVID-19 pandemic, found relatively high rates of emotional exhaustion (55%) and depersonalization (61%) among orthopaedic surgeons. These higher rates could be due to the unique stressors of the COVID-19 pandemic, which has been associated with increased psychological stress, including anxiety and burnout (Coleman, Abdelsattar, and Glocker 2021).
This study found that being female, younger, and an early career surgeon was associated with higher rates of emotional exhaustion and depersonalization and reduced personal accomplishment. Younger orthopaedic surgeons or those in the early stages of their practice (< 5 years) likely feel more stress due to financial uncertainty, as they may still be responsible for school loan repayments and may not be financially independent. The suspension of elective surgical procedures and decreased patient volume during the pandemic could place additional emotional stress on younger practicing surgeons (Wong et al. 2020). Female orthopaedic surgeons’ higher rates of emotional exhaustion may reflect gender-related harassment, worry over exposing vulnerable family members to the virus, and gendered expectations to provide care for children or other family members on top of existing household responsibilities (Allen et al. 2020; Wenham, Smith, and Morgan 2020). Samora et al. found that female orthopaedic surgeons were significantly more likely to experience discrimination, bullying, and sexual harassment, all of which can contribute to burnout (Balch Samora et al. 2020).
COVID-19 has had a significant negative impact on the personal and mental well-being of the majority of orthopaedic surgeons in this sample (79%), contributing to burnout. Delay of advancement/tenure, increased financial distress, and changing practice dynamics were all significant determinants of burnout. Due to the pandemic, many orthopaedic practices have furloughed and reduced staff, decreased clinic hours, reduced pay, and shifted to telemedicine (Flynn 2020), which all disrupt a physician’s practice. Because elective procedures were cancelled in most locations due to the pandemic and continue to be cancelled due to re-emerging COVID-19 variants (“Release of Emergency Order/Notice: Medical and Surgical Procedures, Dental Visits, Procedures and Surgeries Other Healthcare Services” 2021) many orthopaedic surgeons have experienced a significant decrease in patient volume and revenue (Kale et al. 2020; Wong et al. 2020). The suspension of elective surgeries at academic centers represented a decline in invaluable training for residents and income for attending surgeons. At the cost of specialized teaching and training opportunities, many attending surgeons and residents either volunteered for or were redeployed to teams caring for COVID-19 patients (Rahman et al. 2020; Congiusta et al. 2020), further disrupting practices and contributing to increased burnout.
The COVID-19 pandemic has presented challenges for parents and caregivers attempting to work while caring for children, in large part due to school closures and implementation of distance learning (Kuehn 2020). Despite these obstacles, our study was in agreement with previous literature (Saleh et al. 2009) that being married and having children were protective factors against burnout compared to single, childless surgeons. This study also found that mental/emotional distress and deteriorating home situations were significant determinants of burnout. This finding is supported by previous literature that lack of support from spouses and poor marital relationships can increase emotional exhaustion among orthopaedic surgeons (Saleh et al. 2009).
Higgins et al. found that female orthopaedic surgeons perform substantially more unwaged household work than their male counterparts (Higgins et al. 2021). The pandemic has likely further exacerbated this divide: multiple studies have found that, as a result of the pandemic, women have spent more time on household tasks (Rhubart 2020), and shouldered the majority of childcaring duties (Miller 2020). Surgeons who worked for employers that did not change policies to allow for flexibility during the pandemic also suffered from high emotional exhaustion. All these factors contribute to a vicious cycle perpetuating burnout among female surgeons: lack of good childcare and workplace policies, especially in a field like orthopaedics, where women are minorities and more susceptible to discrimination (Balch Samora et al. 2020), make it even more difficult for women succeed within the field. Given that the COVID-19 pandemic continues to stress our healthcare system’s resources and personnel, reassessing policies that are in place is critical in order to support orthopaedic surgeons and prevent further burnout.
This study has several limitations. The response rate was relatively low (11.3%), and thus the results may not be generalizable to all practicing orthopaedic surgeons. The high nonresponse rate was likely related to the perceived time burden of completing the survey: however, among respondents, we had a very high survey completion rate (98%). Female orthopaedic surgeons were underrepresented in this sample, although the male to female ratio (about 3:1) reflects the gender distribution of current practicing orthopaedic surgeons (Rohde, Wolf, and Adams 2016). Survey questions about emotional state and family could also be considered subjective and have variable interpretations. Selection bias from our sample means our results may not be generalizable to all practicing orthopaedic surgeons: our sample consisted of mainly male academic orthopaedic surgeons, and very few hospital or private practice surgeons. Results may vary when considering how orthopaedic surgeons in different practice settings, such as private, hospital, or community settings, were impacted by the pandemic. Other factors that could potentially impact physicians’ resilience during the pandemic, such as monetary compensation, time spent driving children, or other lifestyle factors, were not studied. This study is a cross-sectional survey, and causal relationships cannot be inferred from the data
Conclusion
This study quantifies how burnout during the COVID-19 pandemic has impacted orthopaedic surgeons, their practices, and family dynamics. Overall, there were high rates of burnout. Younger orthopaedic surgeons or those in early stages of practice were more susceptible to burnout. Female orthopaedic surgeons, especially childless and unmarried surgeons, experienced more emotional exhaustion and depersonalization. Changing practice dynamics, financial distress, and lack of workplace flexibility were all contributing factors to burnout. Orthopaedic surgeons who are younger, beginning practice, and are women are vulnerable to being spread too thin by the pandemic, contributing to burnout and potentially worse outcomes for patients and surgeons. Leaders in the orthopaedic field should encourage better workplace flexibility and advancement for women who may be under increased stress, as well as financial safeguards to better protect orthopaedic surgeons from changes as a result of the continuing COVID-19 pandemic.