






INTRODUCTION
Distal tibial fractures are very notorious for healing. Very little soft tissue cover especially skin and some subcutaneous fat not only increases the risk of open tibial diaphyseal fractures but also lead to delay in fracture healing and many other hardware related complications.
Of all the open fractures, 63% are seen in the tibia alone (Gustilo, Mendoza, and Williams 1984). Historicaly though distal tibial fractures were managed conservatively and with good results but it was only true for closed and simple distal tibial fractures. Open distal tibial fractures had many complications. Management of tibial diaphyseal fractures has always held a particular interest for orthopaedic surgeons. Many factors are considered for particular modality taking into account the fracture geometry, personality, status of overlying soft tissues, general condition and the surgical fitness. However surgery is well accepted modality to treat these fractures (Haines et al. 1984). In case of open tibial fractures stress is laid on the early surgery and thorough irrigation and debridement. After irrigation and debridement many techniques are described for management of open distal extra articular tibial fractures. Gustilo and Anderson classification (Kim and Leopold 2012) has helped a lot in classifying these injuries so that a definitive protocol can be established for deciding the type of fixation according to fracture classification.
External fixators are popular because of their ease of application in a shorter time duration, easy availability and the limited effect on the blood supply of the tibia, but these advantages have been outweighed by the high incidences of pin tract infections, the difficulties which relate to the soft tissue management .There is also more potential for malunions/nonunions and importantly very large apparatus which is inconvenient for the patient.
Use of reamed/unreamed intermedullary interlocking locking nails has been done by many authors especially in grade 1 and grade 2 open tibial fractures (Rand, Mosheiff, and Liebergall 1994) but the problem of infection leading to subsequent surgeries in mentioned in literature (Rand, Mosheiff, and Liebergall 1994).
The numerous methods which are used for treating open fractures of the tibia are an evidence of the ongoing efforts which are being made to improve the outcomes of the treatment of these fractures and of the continuing pursuit of more efficient and advanced methods for treating these fractures.
There has been a constant thinking and evaluation to fix these fractures more biologically(Mosheiff, Safran, and Liebergall 1997) with indirect close reduction and applying stable fixation to achieve early union and maximal function (Giannoudis, Papakostidis, and Roberts 2006a). Locking compression plate (LCP) applied as an external fixator fulfils this criteria and is called as supracutaneous plating (Giovannini et al. 2016). This can be an important tool in armamentarium of an orthopaedic surgeon especially in metadiaphyseal fractures with open injury (Giovannini et al. 2016) or closed injuries with precarious soft tissue Tscherne (Kerkhoffs et al. 2003) Grade 2 or 3.
We in our study will compare IMLN vs SCP in open grade 1 and 2 distal tibial fractures. None of the studies in international literature is available on comparison between these two modalities of fixation.
Material and Methods
The present study was carried out in the Department of Orthopaedics from 1.01.2019 to 1.06.2021. 40 patients in age >18 yrs who had Gustilo and Anderson type 1 and type Ⅱ fracture of distal tibia of both sexes were enrolled in this prospective study.
They were randomized into 2 groups of 20 each according to the day of admission. Consultant looking after Tuesday Thursday and Saturday performed IMLN on these patients. Author looking after Monday Wednesday and Friday performed supracutaneous plating.
The patients were allocated a sequential study number and there were no exclusions after randomization. Patients with pathological fractures, non-osteoporotic osteopathies such as endocrine disorders, rheumatologic disorders, diabetes mellitus, renal disease, immunodeficiency states, mental impairment or difficulty in communication were excluded. Those with open fractures according to Gustilo and Anderson type type III or fractures with a displaced intraarticular fragment were also excluded.
Approval for the study was given by the Ethics Committee of our hospital and informed consent was obtained from all patients before operation The patients were selected based on those satisfying the inclusion criteria and were followed up in postoperative period immediately and for one year.
The general data of patients are illustrated in Table 1.
After Initial Irrigation and debridement all patients were immobilized to relieve swelling. Intravenous antibiotics were started on admission and continued till 4th post operative day. Pneumatic tourniquets were used in both groups. However no evidence of intra opertaive bone necrosis due to use of tourniquet in IMLN group was seen.
Surgical steps For Supracutaneous Plating
Fracture reduction is done prior to application of plate. LCP metaphyseal plate of appropriate length is chosen. The plate is initially fixed to the proximal and distal fragments with a k-wire after certaining fracture reduction under fluoroscopy guidance (Figure 1). LCP is placed as close to the bone as possible, yet still allowing some space for swelling and regular wound care, to increase the mechanical stability of fixation (Figure 2). It is separated from the skin surface by a spacer of uniform thickness. For the distal tibia, at least four screws proximally and three to four screws distally are recommended (Figure 3). Successive holes are drilled over locking drill-guides through stab incisions made over the intact soft tissue envelope and screws are placed first distally and later in proximal fragment after ensuing good reduction. Screw tract and wound dressing is done.



Steps for IMLN technique
4 cm long incision was made from the inferior pole of patella to the anteromedial aspect of the tibial tuberosity. A patellar tendon splitting approach was used and entry point was visualized. The entry point was made with a diamond awl. Keeping the knee flexed to 90°, with the help of a curved awl, the window was tunneled to the medullary canal. Curved artery forceps was passed over the window created. The guide wire was inserted up to fracture site. Reduction was achieved by traction and closed manipulation of the limb and guide wire passed to the distal fragment. In all the cases sequential reaming was done with flexible reamers passed over the guide wire and minimum 9 mm diameter nail was used. In 2 cases of small diameter canal of the patients 8 mm nail was used. The nail was introduced over guide wire. Further fine reduction under Image Intensifier was achieved and the nail was negotiated into the distal fragment with the gentle taps of the hammer over the nail head. Use of blocking screws was done in 4 cases. Locking was done in static or dynamic mode depending on the fracture pattern. Free hand technique was used for distal locking of the nail under image guidance. Impaction was done, by padded gentle strokes over the heel (Figures 4 and 5).


In few cases compounding site was around fractures site, so using minimal invasive technique partial threaded cannulated screws were passed to achieve the reduction and then supracutanoeus plate was applied.
The duration of surgery was recorded from the incision to wound closure (Table 2). Postoperatively, IV 2nd generation cephalosporins and aminoglycoside antibiotics were continued for 4 days followed by oral antibiotics for 5 days along with limb elevation, analgesics, antacids and trypsin chymotrypsin. Dressing was changed every alternate day till stitch removal at 14 days. Post operatively below knee posterior slab was given which was removed on second postoperative day and passive ankle range of motion exercises were initiated. Full weight-bearing was restricted for 6 weeks. However partial weight bearing was initiated in both groups on 4th post operative day.
Average stay in the hospital was recorded. Delayed wound healing and superficial infection were defined (Table 3) as persistent drainage from the wound for at least two days, or separation of wound edges to a width > 1 cm and a length > 1 cm (Guo et al. 2010).
Since implant removal in supracutaneous group was on outdoor basis no second surgery/hospital stay was needed. Stay for the subsequent implant removal in IMLN group was added to total duration (Table 4). Follow-up was done at 2 weeks, 6 weeks, 3 months and 6 months after discharge till the fracture united. In each determined follow up at and after 6 weeks, clinical assessment of range of motion, radiological evaluation for progression of fracture healing and complications were documented. The functional outcome of the ankle was assessed with the help of AOFAS (American Orthopedic Foot and Ankle Society Ankle Score) and Knee Society Score (KSS) at 12 months (Table 2). Lower extremity functional score (LEFS) (Table 2) and Functional Results as per Ketenjian and Shelton Criteria (Ketanjian and Shelton 1972) modified by Yokoyama et al. (Yokoyama et al. 1994) were charted (Table 5). Complications like surgical site infection, deep infection, delayed union, non union and ankle stiffness were documented. The radiological outcome was assessed using the Teeny-Wiss scoring system and fracture union (Teeny and Wiss 1993) (Table 6). Fracture union was subject to radiographic evidence of union and pain-free weight bearing.
Results
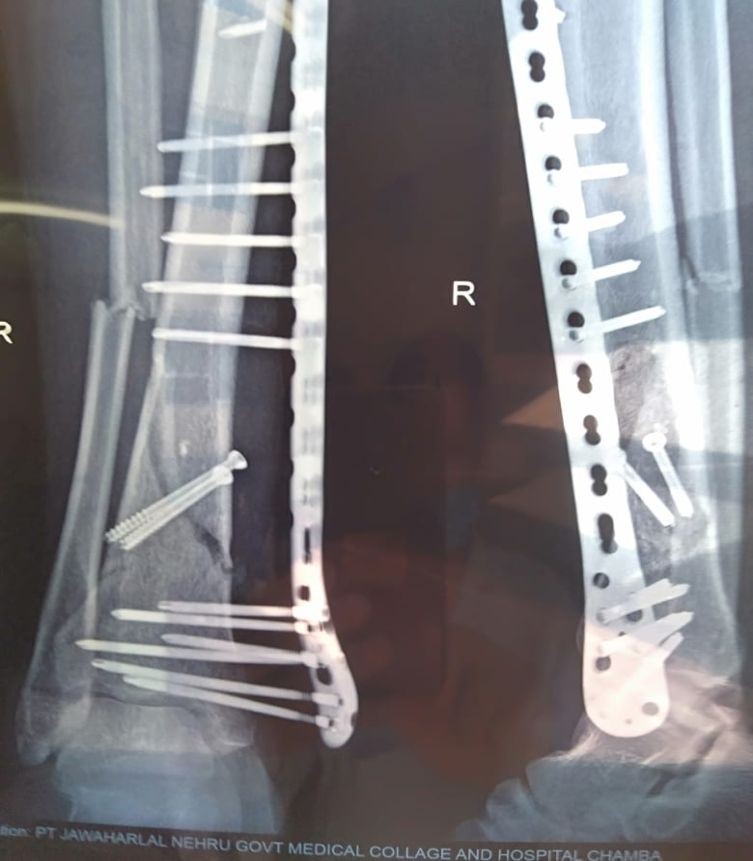
100% fracture union was seen in both cases (Figures 6 and 7). Only one case of deep infection was seen in IMLN group where implant removal and lavage was needed as a secondary procedure. One delayed union in SCP group was managed with removal of 2 screws across fracture site under local anesthesia. Mean time for union was 22 weeks in SCP groups and 19 weeks in IMLN group.


A total of 25 males and 15 females were enrolled in the study. 21 of them had Gustilo and Anderson type 1 open tibia fractures and 19 of them had type Ⅱ tibia fractures. In 25 patients right limb was involved. Overall duration of surgery was 90 ± 5 min in all cases and it was comparable in IMLN and SCP groups.
Intra operative blood loss was 165 ml and was more in IMLN group than SCP group (100) ml.
LEFS at 1 year was 90 in SCP group whereas it was 80 in IMLN group. p value was 0.001.
AOFAS score was similar in both groups showing good functional outcome around ankle joint.
Knee society score was statistically better in SCP group (82) whereas in IMLN group it was 70.
Duration of hospital stay (including implant removal) was 10 days in SCP group while it was 12 days for primary surgery in IMLN group but came out to be 19 days after adding the admission days for implant removal.
Superficial infection occurred in 3 cases of SCP group and 4 cases of IMLN group. Incidence of malunion was 5% in both groups.
Overall general well being and functional outcome was statistically better in SCP group. (Table 5).
DISCUSSION
Controversy is still present about the surgical merits of the different lines for treating distal tibia fractures; decision making is difficult, and no best treatment has been determined.
Soft tissue management along with accurate reduction and alignment are two challenging problems for any orthopaedic surgeon especially while dealing with fractures of tibia. No doubts external fixator has given good results in soft tissue healing but they are very cumbersome and interfere with activities of daily living.
Reamed or unreamed IMLN has been done regularly for Grade -1 and Grade -Ⅱ open fractures of tibia either in a single stage or in staged surgeries. Literature (Wang et al. 2019; Giannoudis, Papakostidis, and Roberts 2006b) have shown good results with these methods, but also with various complications (Xu et al. 2014).
Srinivas et al.(Srinivas and Nazeer 2017) in their study on 44 open tibia fracture patients has shown Intramedullary nailing for open fractures of the tibial shaft is an excellent mode of therapy. They recommend that wound debridement with or without closure along with primary interlocking nailing should be done for open fractures of the tibial shaft (from group I up to group IIIA of Gustilo classification). At a later date, SSG or flap or delayed primary closure, etc should be done.
NONE of the study is available in the literature as per search in major databases shows any comparison between IMLN tibia and Supracutaneous plating of the tibia. Comparisons have been made between Mininal invasive plating osteosynthesis and IMLN tibia (Wang et al. 2019).
Indivuidual Studies are done on Using LCP as external fixator in supracutaneous mode and have shown promising results.
This technique was first described by Marti et al. (Marti and van der Werken 1991) in 1991 was developed independently in 1987 by d by Ramotowski and Granowski (Marti and van der Werken 1991) and was named as ZESPOL-osteosynthesis.Their experience using AO-plates as external fixators was unequivocally positive.
In 10 patients the fixation done by Marti et al. (Marti and van der Werken 1991) provided enough stability to allow uneventful bone healing and/or to eliminate infection. Stability was high due to the short distance between the plate and the soft tissues. Patients were easily adapted to this new method and implant removal was easy.
Ziran et al. (Ziran et al. 2007) also delineated some theoretical advantages of supracutaneous fixation using LCP. First, small amounts of axial micro motion may reduce stress-shielding of the fracture site. Load-sharing during weight bearing may stimulate the developing callus until bony union. Second, “controlled destiffening” or dynamization by removing screws closest to the fracture site is possible, allowing some measure of control to the load-sharing process.
In our study mean age of distribution, gender of the patient and mean duration between admission and surgery were same in both IMLN and SCP groups. So the results obtained are comparable in both groups.
No non union was seen in both the groups. All 40 patients managed for open tibia fractures went into union.
However one case of delayed union was seen in SCP group which was dynamised in local anesthesia and 2 screws nearer to fracture site were removed and aggressive weight bearing was initiated it went into union.
Anterior knee pain was one of the major complaints in patients operated with IMLN group. Nearly 25 % of the patients had this pain which eventually lead to implant removal and second surgery. Incidence of anterior knee pain has been noted between 31% to 86% in various studies (Cartwright-Terry, Snow, and Nalwad 2007). The protrusion of nail tip (anterior and superior prominence) has been reported as one of the contributing factors for knee pain (Keating, Orfaly, and O’Brien 1997).
Due to this knee pain which led to implant removal in 25% of patients the average hospital stay in IMLN group was 19 days which is statistically significant as compared to 10 days in SCP group. This additional stay puts additional psychological and financial stress to an already traumatized patient. In remote areas like the place where institute is situated and in developing and low income countires like India this is a major concern. Easy and day care removal of implant in SCP cases is of better acceptance in situation prevalent in developing nation.
Mean time for union was more in SCP group (22 weeks) as compared to IMLN group (19 weeks). This might be because IMLN is a load sharing device while SCP is load bearing device. However this was found not to be statistically significant.
Mean AOFAS was similar in both IMLN and SCP groups showing good functional outcome around ankle joint.
However lower extremity functional scoring which include all joints of leg including knee joint was statistically better in SCP group than IMLN group.
We have used Ketenjian and Shelton Criteria modified by Yokohama et al for a better overall assessment of gross functional outcome of the patient as a whole.
In 90 % of the case outcome was excellent in SCP group while only in 60% of the cases in IMLN group it was good.
12 percent of patients in IMLN group had pain on ordinary activity and occasional swelling. One patient had poor score as per yokohama criteria. This patient had deep infection with pouring pus from knee insertion site. Luckily fracture was united and implant removal followed by good lavage settled the infection. This was the only case of deep infection in our study of 40 patients.
Superficial infection occurred in 15% and 20% of patients in SCP and Imln group but they were managed with antibiotics and good dressings. Though pin track infections are seen in patients managed with external fixator, but due to better stability provided by locking screws to the plate such pin track infections are far lesser in patients managed with supracutaneous group.
Radiological outcome using teeny and wiss criteria was anatomical in 80% cases of IMLN group as compared to 75% of cases of SCP group. This showed a good overall radiological acceptability in our study.
However in one case screw breakage was reported (Figure 8).We observed that during screw insertion it is very important to get a bicortical purchase. If alignment of plate to the anterior and posterior border of the tibia is not parallel then there are high chances that in last screws we are unable to get bicortical purchase. Inserting screws with torque can result in screw breakage.

Incidence of malunion was similar in both groups.
We have shown good functional outcome in SCP groups owing to non involvement of knee joint for entry site (not needed in SCP) and also due to easy implant removal as an outdoor procedure.
Except for this all other modalities are similar or slightly (statistically not significant) better in IMLN group.
Our results have shown that both a closed IMLN and LCP in Supracutaneous mode can be used safely to treat grade -1 and grade -Ⅱ dista metaphyseal fractures of the tibia.
Conclusion
Though major complications were not seen in any of the group except for a solitary deep infection in IMLN group, patients in SCP Group had lesser incidence of persistent pain or other chronic symptoms and were happier (better LEFS score, better Yokahama scoring) than their counterparts with interlocking nail. Using locking plate in a supracutaneous mode is a very simple, easy, rapid, reliable and effective method for management of open tibial fractures in adults, especially in terms of patient satisfaction and can be considered as an effective alternative to nailing in selected patients.
Conflict of Interest
The authors declare that they have no relevant financial or non-financial interests to report.
Funding
This research did not receive any specific funding.
Ethical Approval
Ethical approval was not required.
Informed Consent
Written informed consent was obtained from all patients and/or families.