


1. Introduction
Humeral fractures account for 1-5% of all fractures each year (Ekholm, Adami, et al. 2006; Ekholm, Tidermark, et al. 2006; Wolf, Athwal, Shin, et al. 2009; McKee and Larsson 2010). Closed treatment of humeral shaft fractures remains the standard of care in many instances, with good results (Sarmiento et al. 1977; Balfour, Mooney, and Ashby 1982; Zagorski et al. 1988; Foulk and Szabo 1995; Hunter 1982; Gregory and Sanders 1997; Gosler et al. 2012; Shields et al. 2016; Updegrove, Mourad, and Abboud 2018; Ali et al. 2015). Operative stabilization can be indicated due to a variety of factors including obesity, concomitant injuries, bilateral injuries, and associated vascular or neurological injuries (Ali et al. 2015; Carroll et al. 2012; Decomas and Kaye 2010; Bell et al. 1985; Bleeker, Nijsten, and Duis 1991; Brumback et al. 1986; Vander Griend, Tomasin, and Ward 1986; Foster et al. 1985, 1993; Gainor and Metzler 1986; Denard et al. 2010), and recent studies have shown improved outcomes in surgical versus non-surgically treated humeral fracture in trauma patients (Denard et al. 2010; Matuszewski et al. 2015). In cases of polytrauma, humeral stabilization can facilitate earlier patient mobilization by allowing immediate crutch ambulation.
The traditional recommendation for humeral shaft fixation is the use of a 4.5 mm narrow or broad dynamic compression plate (DCP). A previous study on weight bearing after humeral shaft fractures treated with plate fixation compared groups treated with immediate weight bearing versus a rest period of six weeks (Tingstad et al. 2000). The authors concluded that early weight bearing was acceptable; however, this study was completed prior to the widespread use of locked plates and mainly used broad 4.5 mm fragment plates. Advances in plate technology, such as locked and hybrid designs, have been shown to demonstrate greater strength and stiffness than traditional compression plates (Gardner et al. 2006, 2005; Ahmad, Nanda, Bajwa, et al. 2007; Bellini, Raimondi, Accetta, et al. 2007; Catanzarite, Alan, Baig, et al. 2009; Egol et al. 2004; Sanders et al. 2002; Snow, Thompson, and Turner 2008; Bottlang et al. 2009; Kubiak et al. 2006; Patel et al. 2011).
Successful fracture fixation requires matching the correct plate to fit the bone. Genetic and ethnic differences exist in patients which may limit traditional techniques of fixation. Smaller 3.5 mm plates are an alternative for humeral fracture fixation. The surgeon can control working length of the construct and stiffness by screw and plate selection. However, there are questions regarding plate type, plate length, and screw configuration that remain unanswered.
The answers to these biomechanical questions may provide useful data for clinical application. Our study examines the viability of utilizing a 3.5 mm locking dynamic compression combination plate (LCP) with a hybrid screw combination in place of the 4.5 mm non-locking DCP. We compared the two plates in a crutch ambulation model. We hypothesize that the small fragment plate applied using a hybrid construct technique will support at least 75% of the load of the larger plate and will fail at a higher load than that expected during immediate weight bearing.
2. Methods
2.1 Preparation of Samples
Twenty-four Sawbones synthetic humeri (Pacific Research Laboratories; Vashon, WA; United States of America) were potted in a lead-bismuth alloy on the distal end. The bones were angled at 15° in the frontal plane and -6° in the sagittal plane (Requejo et al. 2005; Opila, Nicol, and Paul 1987; Slavens et al. 2006). This approximates ambulation with the assistance of forearm crutches. A jig was fashioned to maintain this angle while the potting material hardened. Following potting, the samples were rigidly mounted in the MTS machine (MTS 858, MTS Systems; Eden Prairie, MN; United States of America) and subjected to stiffness testing (Figure 1). Each sample was loaded with force control to -333 N and a torsional load of 10 N-m applied (external rotation) and held for 5 seconds. This was repeated 5 times. Initial axial stiffness of the sample was then calculated from the results of these trials.

To determine the average stiffness of the unplated bone, the force data was imported to Microsoft Excel for analysis. The axial and torsional values for the loading portion of each cycle were isolated and graphed. An average of the five cycles was computed for all samples. These averages were divided into groups based on their subsequent plating with either the 3.5 mm or 4.5 mm plate, with an overall average also computed for each group. Samples 1 through 4 were utilized for preliminary testing and were not included in the analysis. Samples 11 and 12 were discarded prior to cyclic testing due to damage during preparation. Samples 22 and 24 were discarded, one from each subset, due to testing difficulties. As a result, there remained eight samples in each of two groups.
After completion of the stiffness testing, each bone was plated with either a 3.5 mm LCP or a 4.5 mm narrow DCP (Synthes USA; Paoli, PA; United States of America). The plates were 316L Stainless steel with nickel between 13%-15% by weight. An 8-hole 3.5 mm LCP utilized non-locking 3.5 mm screws placed in the holes at each end of the plate and immediately on each side of the fracture site, and locking screws inserted in the second hole from each end for a total of 6 cortices of fixation on each side of the fracture. This was to provide a longer working distance for the plate. An 8-hole 4.5 mm DCP with the same six screw configuration utilized all non-locking 4.5 mm screws in the construct.
2.2 Cyclic Testing
Following the application of plates, a 5 mm segment of bone was removed with a hand saw from the mid-position of the sample. The gap was verified for uniformity with a digital caliper and trimmed as needed. Each construct was rigidly mounted in the MTS machine and pre-loaded to -10 N of axial force and 0 N-m of torque (Figure 2). The samples were subjected to cyclic loading between -10 and -333 N axially and 0 and 1.0 N-m of torque at a rate of 0.5 Hz for 90,000 cycles. This simulates the use of forearm crutches during the approximate healing period by a patient of 150lbs for 3 months (Requejo et al. 2005; Opila, Nicol, and Paul 1987; Slavens et al. 2006; O’Toole et al. 2008). This was chosen as platform type crutches would be most likely used in a multiple trauma patient with upper extremity injuries. The samples were observed frequently during the trials to ensure no complications from the testing process. No premature failures were recorded.

Stiffness values were determined at three separate stages of cyclic loading for both axial force and torsional force: 20 seconds after the start of the procedure, 20 seconds before the end of the procedure, and at the halfway point of the procedure. The values for five loading cycles were again isolated and graphed, with the stiffness of the curves then averaged to provide a value for the construct (Table 1). An average stiffness for each subset was then computed by averaging these values across each group. These averages were then compared to the average initial axial stiffness of the unplated specimens to find a percentage of the repaired stiffness returned by the construct.
2.3 Failure Testing
All surviving samples were then subjected to a failure protocol. The samples were pre-loaded to -10 N of axial compression and 0 N-m of torque. The axial force was ramped to -2500 N, while torsional rotation was monitored but not controlled. Failure was defined as closure of the fracture gap at the medial cortex, fracture of the construct, or torsional angle exceeding 13°. Preliminary testing showed that closure of a 5 mm gap or torsional angle exceeding 13° each resulted in permanent deformation of the plates. The failure value for each specimen was determined by examining the loading data for the failure test. The final value before defined failure was used in each case. This value was then used to determine an average for both the 3.5 mm plate and 4.5 mm plate group. All implants exhibited some form of failure, with the most common being excess torsional angle. Samples were then visually examined for deformation and implant loosening.
2.4 Statistical Analysis
The comparison of independent measurements was by t-test with significance of P < 0.05.
3. Results
3.1 Cyclic Testing
For the 3.5 mm plates, the overall average axial stiffness was calculated to be 980.56 ± 143.10 N/mm (Table 1). The intact axial stiffness for this group was 1829.9 ± 628.97 N/m. This corresponds to a repaired stiffness of 53.6% of the intact bone. For the 4.5 mm plated group, the average axial stiffness was 1220.37 ± 276.02 N/mm, with an intact axial stiffness of 1938.51 ± 386.79 N/mm (Table 1). This results in a repaired stiffness of 62.9% of the intact bone. Our analysis revealed a statistical difference between the average axial stiffness of the 3.5 mm plate group and the 4.5 mm plate group (P < 0.05). For the torsional stiffness, the 3.5 mm plate group had an average of 1.53 ± 0.19 N-m/deg, with the intact torsional stiffness of 4.41 ± 0.232 N-m/deg (Table 1). The resulting repaired stiffness is 34.7% of the intact bone. For the 4.5 mm plate group, the average torsional stiffness was 2.04 ± 0.40 N-m/deg (Table 1), compared with an intact torsional stiffness of 4.5 ± 0.181 N-m/deg. This corresponds to a repaired percentage of 45.3% of the intact bone. Our analysis revealed a statistical difference between average torsional stiffness of the two groups (P < 0.01).
3.2 Failure Testing
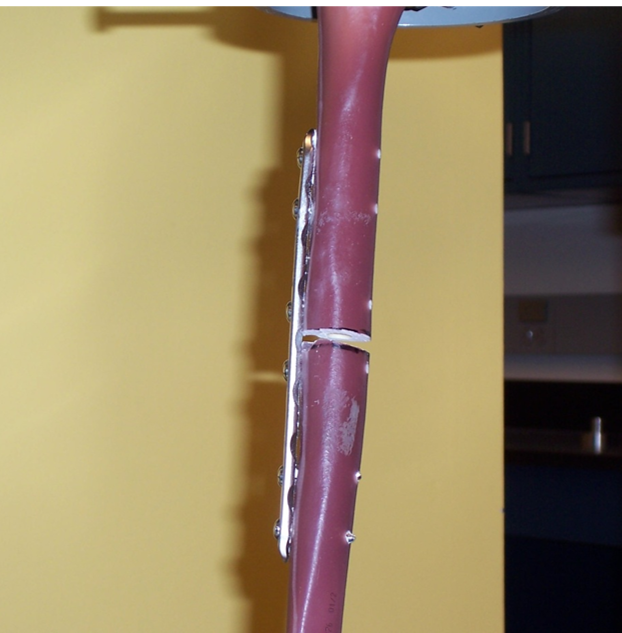
All bones failed by one of our failure definitions, with the 3.5 mm plate specimens failing via excessive rotation exceeding 13 degrees (Figure 3), while the 4.5 mm plate specimens failed with closure of the fracture gap (Figure 4). Average load at failure for the 3.5 mm plate group was 1870 N, while the 4.5 mm plate group failed at an average load of 2366 N (Table 1). Statistical analysis showed these to be statistically different (P < 0.01), as were the differences in failure mode. However, none of these failures were due to bone fracture or screw pullout.


4. Discussion
Standard of care for an isolated humeral shaft fracture is usually nonoperative; consisting of a coaptation splint acutely followed by management in a fracture brace. However, this algorithm does not apply to a polytrauma patient who also has injuries necessitating crutch ambulation. Traditionally, a 4.5 mm DCP has been used in these situations. We compared a 3.5 mm LCP in hybrid mode to a 4.5 mm non-locked DCP because we felt that the smaller plate in hybrid mode would compare favorably to the larger plate and offer the clinician options for operative treatment of humeral shaft fractures with a smaller plate. Our results support our hypothesis because mean failure loads for the 3.5 mm LCP were 79% of the mean failure load for the 4.5 mm DCP, and the mean failure load for the 3.5 mm LCP was 2.8 times the model physiologic load chosen for this study.
O’Toole et al. completed a biomechanical study to determine if locking screws offered any advantage over non-locking screws for plate fixation of humeral shaft fractures (O’Toole et al. 2008). The model was a comminuted midshaft humerus fracture and humeri were plated posterior with 10-hole 3.5 mm locking compression plates with the first group using only non-locking screws and the second group using locking screws. Stiffness and failure testing were performed on synthetic and cadaveric match pairs. Though they used 3.5 mm plates in this study, which is similar to our study, their method of testing used a fracture gap of 1 cm, while ours was 5 mm. This difference could theoretically place their model under additional stress as the larger gap closes. Their results demonstrated plate failure in the synthetic model above physiologic loads and there was no advantage to locking screws. In the cadaveric portion, there was no advantage of the locking screws in the 4 stiffness modes tested. Smaller 3.5 mm plates seem a logical option to choose for fixation of humeral shaft fractures depending fracture morphology and patient variables. These small fragment plates offer the advantage of more holes per unit length–thus more screws in a given segment of bone for plate length. In addition, the plate requires slightly less dissection and is easier to contour compared to the 4.5 mm counterparts. If a 3.5 mm plate is used, do locking plates and screw constructs offer any benefit? O’Toole’s study concluded there was no advantage to using all locking screws with 3.5 mm plates (O’Toole et al. 2008).
Hybrid fixation has been described to selectively affect the stiffness of constructs. These can go both ways: whether to purposefully increase or decrease the construct stiffness to affect fracture healing and meet the needs of the patient. Regarding a “hybrid” technique, Gardner et al. evaluated hybrid locked plating of osteoporotic fractures of the humerus (Gardner et al. 2006). The authors used 4.5 mm LCPs with 3 screws on each side of the fracture using locking, non-locking, or a hybrid model. To simulate osteoporotic bone, they over-drilled the screw holes. The authors completed cyclic torsion and torsional stiffness and compared the groups. The hybrid constructs in this model appeared to be mechanically similar to locked constructs and more stable than unlocked applications. A biomechanics study by Freeman et al. also used 4.5 mm LCPs with three screws on either side of the fracture using a combination of locked and nonlocked screws. They found that 12-hole hybrid plates require a minimum of 3 locked screws on each side of the fracture before an increase in torsional stiffness is seen, and that the configuration of where the locked screws were placed in the plate also impacted torsional stiffness (Freeman et al. 2010).
Tingstad et al. (2000) sought to answer the question of weight bearing following humeral plating using primarily 4.5 mm plates with 3.5 mm plates used in 6% of their cases. The weight bearing status of the humeri was based on the associated injuries and not the fracture patterns. In this study, 52% of the fractures had immediate full weight bearing. The authors concluded that immediate full weight bearing does not have an adverse effect on the outcome of operatively treated fractures of the humeral shaft (Tingstad et al. 2000). The authors could not suggest an ideal plate configuration but recommended at least six to eight cortices of fixation proximal and distal to the fracture site. Our study compared both plate types with at least six cortices proximal and distal to the fracture.
Our surgeons have used 3.5 mm plates as appropriate for patient and fracture for humeral shaft fractures over the past several years without significant adverse clinical issues. In multiple trauma patients, all humeri were fixed to be full weight bearing. Since no plate and screw combination had proved superior in the literature and clinical practice, we chose a hybrid model to reflect the clinical setting, as use of all locking screws in non-osteoporotic bone is not standard. In our Sawbone humeri, plates were applied anterolaterally. The previous biomechanical studies applied plates posteriorly (Gardner et al. 2006; Catanzarite, Alan, Baig, et al. 2009; O’Toole et al. 2008). In a multiple trauma patient, an anterolateral approach may be advantageous so other fractures can be addressed without changing patient position, or it may be necessitated due to their injuries. A recent paper by Idoine et al. performed internal fixation via an anterior approach to the humerus utilizing both 3.5 mm and 4.5 mm plates and found the majority of clinical and functional short- and long-term outcomes to be comparable to those of the posterior approach as reported in literature (Idoine et al. 2012). Anterolateral approaches with 3.5 mm LCPs have also been used with minimally invasive plate osteosynthesis with good results (Tetsworth, Hohmann, and Glatt 2018). Our biomechanical model simulated the position of weight bearing with crutches (Requejo et al. 2005; Opila, Nicol, and Paul 1987; Slavens et al. 2006). We chose hybrid fixation, as the previous study demonstrated this configuration to be more stable than unlocked plate application. Patel et al. concluded with an all-unlocked construct that a small fragment plate construct could not support weight bearing in a comminuted model (Patel et al. 2011). We chose a model to give an optimum balance of stiffness (not too stiff to affect fracture healing), while also being cost-conscious, so the model can be applied clinically.
Catanzarite et al. evaluated biomechanical testing of unstable humeral shaft fractures with 4.5 mm DCP and 3.5 mm LCP with a 5 mm fracture gap (Catanzarite, Alan, Baig, et al. 2009). This was most similar to our model. They completed stiffness tests in AP bending, medial-lateral bending, torsion, and axial compression. They also evaluated fatigue characteristics under cyclic AP bending and found no failures. The authors felt that the results indicate that the 4.5 mm plate is mechanically advantageous for stabilizing a comminuted fracture, but the 3.5 mm LCP could support physiologic loads applied during the postoperative rehabilitation (Catanzarite, Alan, Baig, et al. 2009). However, it is difficult to conclude that a 5 mm fracture gap correlates with a comminuted fracture. We use this model in studies, but in reality, there could be comminution spreading several centimeters of the diaphysis. Perhaps the technique employed for fixation of those highly comminuted fractures would be bridge plating, which was not evaluated in our study or other biomechanical studies of humeral shaft fixation.
Our biomechanical comparison by t-test reveals a significant difference between the average axial stiffness of 4.5 mm DCP vs. 3.5 mm LCP and a significant difference between the torsional stiffness of the 4.5 mm DCP vs. the 3.5 mm LCP. These results followed expectations due to differences in plate dimensions. However, 3.5 mm plates provided 80% of the axial stiffness and 75% of the torsional stiffness of 4.5 mm plates.
Failure loads and mode of failure were significantly different between plates. No construct failed by screw cutout, and cyclic loading was not a contributing factor. Our model includes a significant fracture gap, which required the plate to carry the entire load, and is the worst-case scenario for constructs in a clinical setting. The lack of plate failure or screw cutout in this situation suggests that the results from more typical clinical situations will also be acceptable. While the plates performed differently, both appear to support loads that are anticipated in the clinical setting.
This study contains several limitations. The use of Sawbones mimics healthy bone and may lead to conclusions that are not applicable to pathologic bone, especially osteoporotic bone. While we did apply several cycles of load, the loading regime is quasi static and does not fully mimic the dynamic application of load of crutch walking. Due to machine limitations, we were required to rigidly fix the ends of specimens, which may lead to unnatural stresses in the construct.
Our results followed expectations due to differences in plate dimensions. There were no apparent differences between constructs following cyclic loading. Our model includes a fracture gap, which requires the plate to carry the entire load, and it does not provide for healing that would occur following injury, each of which would tend to improve performance of both constructs in a clinical setting. In conclusion, while the constructs performed differently, both appear to support loads that are anticipated in the clinical setting.
Acknowledgements
The authors would like to acknowledge James Buchheit, MS and Sean Owens, MD for their contributions to this research project, which include initial project development by Dr. Owens as well as design and construction of experimental setups by Mr. Buchheit.
Disclosures
This research was supported in part by a research grant from Synthes, Paoli, PA. All authors were fully involved in the study and preparation of the manuscript. This manuscript is being submitted solely to Journal of Orthopaedic Experience & Innovation and is not to be submitted for publication elsewhere.