
Introduction
With the increasing incidence of end stage knee arthritis, TKA procedures are on the rise (Kurtz et al. 2007). Concomitantly, the incidence of PJI TKA is also increasing as these procedures become more common. The PJI rate after primary TKA ranges from 0.5% to 2% (Kurtz et al. 2010; Matsen Ko et al. 2016) and is a serious problem despite advanced surgical techniques, and rigorous adherence to perioperative antibiotic prophylaxis. Infection additionally is the leading cause of failure following revision TKA (Suarez et al. 2008). However, even at the low end of infection rates, with the increasing number of patients undergoing primary TKA, prosthetic joint infection is still a significant concern. A variety of surgical techniques and antibiotic spacers have been developed to improve the treatment of the chronically or age-indeterminate infected TKA. Both static and mobile knee spacers have been used extensively in two-stage exchange to resolve PJI following TKA (Park et al. 2010; Silvestre et al. 2013). The gold standard treatment of chronic periprosthetic TKA infection with a 2-stage exchange yields infection eradication rates of 80-90% (Mahmud et al. 2012). In the 2-stage technique, the infected knee prostheses and associated cement are removed and a thorough debridement of all infected or necrotic tissue is performed with copious irrigation of the knee joint. A temporary antibiotic-impregnated prosthesis, i.e. spacer is additionally implanted after a rigorous debridement is performed. Postoperatively, intravenous antibiotics are administered, and reimplantation is subsequently performed once clinical and laboratory indicators demonstrate infection eradication. Two-stage exchange is the generally preferred treatment method for PJI in North America, for both difficult to treat pathogens as well as in patients who have already undergone previous revision procedures.
Static antibiotic knee spacers have several potential advantages including the release of local surgeon directed antibiotic therapy, enhanced stability, and the maintenance of soft-tissue tension within the knee. However, they may also lead to further problems particularly pronounced stiffness of the knee joint, difficulty with removal at the time of the reimplantation procedure, and the potential significant for bone loss of the distal femur and/or proximal tibia (Calton, Fehring, and Griffin 1997; Fehring et al. 2000).
Articulating antibiotic knee spacers, i.e. mobile spacers made of gentamycin impregnated polymethylmethacralate (PMMA) bone cement have evolved to overcome the difficulties encountered by static spacers and mimic the function and geometry of a knee arthroplasty prosthesis. Articulating knee spacers additionally elute high concentrations of antibiotics, allow early patient rehabilitation, and preserve range of motion of the knee, potentially resulting in improved mobilization. Articulation of the mobile spacer may potentially yield enhanced range of motion following the reimplantation surgery due to less scaring of the collateral ligaments and extensor mechanism. Several types of articulating spacers are available, either premade, i.e. commercially available, or surgeon molded in the operating room; however the articulation of these devices may be associated with a variety of spacer-related complications, primarily among them, dislocation which could threaten or cause extensor mechanism disruption. The choice of articulating knee spacers is generally directed by surgeon familiarity, historical preferences, cost, and hospital availability. We describe our experience of treating PJI following primary and revision TKA in patients with a pre-made knee commercially available articulating antibiotic spacer, (OsteoRemedies® Memphis, TN) in the first stage for the treatment of chronic periprosthetic TKA infection. The aim of the present study was to determine the range of motion of a novel knee spacer in the treatment of PJI following primary and revision TKA with the specific aim of determining postoperative range of motion, function, ease of revision, infection recurrence, spacer related complications, and need for revision following the treatment of PJI. We hypothesized that this commercially available knee spacer may be associated with an enhanced outcome and equivalent infection eradication coupled with both ease of insertion and removal at the time of the second stage reimplantation procedure. We report our experience with management of PJI in TKA patients with the OsteoRemedies® articulating knee spacer.
Materials and Methods
Following IRB approval, a retrospective review of 31 consecutive infected TKAs (26 primaries and 5 revisions) treated between 2014 and 2016 at our clinic was examined. The criteria for study inclusion were revision for infection following primary or revision TKA with one or more infection criteria. At Hinsdale Orthopaedics Associates (HOA), 31 consecutive TKAs (26 primaries and 5 revisions) complicated by infection were treated by one surgeon. The mean age was 62.5 years (range, 47-82). The mean length of follow-up was 3.52 ± 1.36 years (range, 1.29-6.03 years). There were 15 men and 16 women. Implants included 26 primary TKAs and 5 revision TKAs (including two already revised for infection with a previous two stage exchange). All primary TKA patients had a cemented condylar prosthesis with patellar resurfacing using a polyethylene button. Revision TKA patients had cemented stemmed CCK type prostheses with or without patellar resurfacing. Clinical assessments were performed before surgery and at latest follow-up.
All patients received similar supervised postoperative care with early mobilization (out of bed the day after surgery; fully weight bearing on affected extremity with assistive devices as needed). All patients received intravenous antibiotics for 6 weeks through a peripherally inserted central catheter (PICC) following the first stage procedure (resection arthroplasty, rigorous debridement of infected bone and soft tissue, and gentamycin impregnated spacer placement). Choice of postoperative antibiotics was directed by culture results under the guidance of infectious disease consultation and continued for 6 weeks. In addition, all patients received thromboembolic prophylaxis with aspirin, apixaban, or low molecular weight heparin starting postoperative day 1, or Coumadin (DuPont Pharmaceuticals, Wilmington, Del) starting the night of surgery and continued for 6 weeks. Patients were treated with aspirin (325 mg PO BID) unless they were previously on Coumadin or had a history of prior thromboembolic disease in which case they were treated with Eliquis or Lovenox.
For each patient, variables including range of motion were examined following spacer placement and postoperatively after the second stage procedure. Knee flexion and extension were measured by a single surgeon using a goniometer with the patient in a supine position, and the measurements were recorded in the medical record. Institutional research board approval was approved by Western IRB. After IRB approval, the patient’s clinical profile was obtained from the electronic medical record. Patient history, physical examination, serological markers, synovial fluid analysis, and microbiolgic studies were assessed for infection criteria including the Musculoskeletal Infection Society. The major and minor criteria which were examined and included the following: (1) sinus tract; (2) positive culture results from 2 or more tissue or fluid samples; and (3) 4 of the following 6 criteria are present: (I) elevated CRP/ESR; (II) elevated synovial WCC; (III) high synovial PMN leukocyte percentage; (IV) presence of purulence in the joint; (V) positive culture result from one sample from the affected joint; and (VI) PMN leukocyte count of more than 5 per high-powered field in 5 high-powered fields on histologic analysis at 400 × magnification (Parvizi et al. 2011). Additionally, symptoms such as pain, warmth, effusions, drainage, redness, and restriction of movement with or without discharging sinuses were noted. After general anesthesia during the first stage surgery, TKA or RTKA components were removed, cement and necrotic bone and soft tissue were curetted out and removed. The femoral and tibial canals were thoroughly cleaned and debrided of infected material. Inflammatory tissue and fluid obtained during this procedure were sent for aerobic and anaerobic bacterial culture and fungal culture.
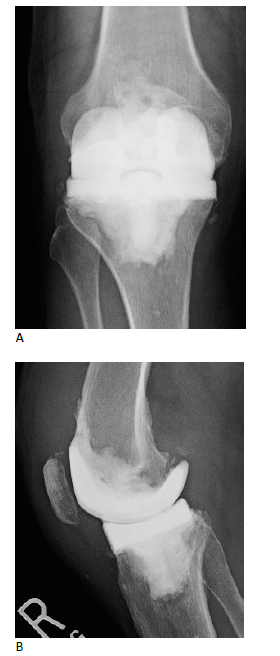
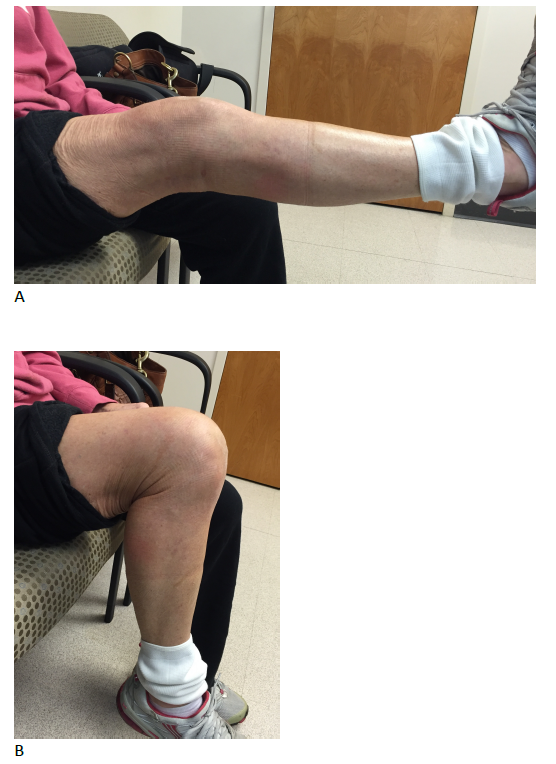
During the first stage procedure, the modular and customized knee spacer was implanted onto the clean bone surfaces using high viscosity gentamicin-loaded bone cement (see Figures 1 and 2). Trialing with flexion-extension matching was done prior to spacer placement to confirm the optimum spacer thickness and provide a smooth knee range of motion (see Figure 3) and reconstitute the flexion/extension gap. Cement in doughy form was layered on the undersides of the femoral and tibial components to make the spacer easier to remove during the second stage procedure. Inpatient physiotherapy was started immediately with knee range of motion and quadriceps strengthening exercises as soon as the pain permitted and full weight bearing ambulation with a walker was performed on the first post-operative day. Patients were discharged home or to a sub-acute nursing facility when medically stable with intravenous antibiotics monitored by an infectious disease specialist. The patients were followed up regularly. Post-first stage procedure intravenous antibiotics were started as per culture and sensitivity report of the fluid and tissue sent for culture preoperatively or intraoperatively. Antibiotics were continued for 6-8 weeks followed by a 4-week antibiotic free period.
_infected_total_knee_replacement_(ap_knee_x-ray)__(b)_femoral_exposure_and_component_re.png)
_ap_knee_x-ray_(b)_lateral_knee_x-ray.png)
_active_extension_and_(b)_active_flexion.png)
Normal skin condition and appropriate healing over the operative site without any redness or sinuses and normal serologic markers range of interleukin-6 (IL-6), ESR, CRP, and a negative knee aspirate after a minimum of a 4 week antibiotic holiday denote infection free and thereby made the patient eligible for the second stage of surgery (Goldman, Scuderi, and Insall 1996). The second stage surgery involved spacer removal, frozen section, and if negative, then definitive revision TKA. Since the intraoperative frozen section examination revealed less than five WBCs per high power field in all patients, the second stage procedure was performed as planned.
Results
Data extraction was completed via a standard form. Patient characteristics including demographics, range of motion, exposure for reimplantation, infection eradication, and complications were recorded. The primary cause for TKA in the 26 patients were for advanced osteoarthritis (25) and rheumatoid arthritis (1). Of the 5 revision TKA patients, 2 were previously revised for arthrofibrosis, 2 for previous infection, and 1 for aseptic loosening. Revisions for arthrofibrosis and aseptic loosening had been revised more than 2 years prior to presenting with infection. Similarly, the 2 previous infected revision TKA patients had been infection free for more than 2 years with a two-stage exchange before presenting with recurrence of infection. In the infection workup of 31 patients, preoperative aspiration was negative in 8 patients (25.8%). The organisms identified from preoperative and intraoperative cultures included the following in 23 patients (74.2%) : S. aureus (6), S. epidermidis (5), Staphylococcus sp not aureus (5), Eschericia coli (2), Morgangella morganii (1), Enteroccocus faecalis (1), Citrobacter diversus (1), Alpha streptococcus (1), E. coli, Corynebacterium, and Staphylococcus sp not aureus (1). There were no patients who presented methicillin resistant S. aureus.
A total of 31 patients (16 female/15 male) undergoing treatment for infection were identified (26 following TKA and 5 following RTKA) from years 2014 to 2016. The mean ± SD ages were 62.5±9.4 years (range, 47-82 years). The overall mean ± SD time of interim spacer placement for all patients was 25.7± 21.9 weeks (range, 8-109 weeks). One patient (spacer placement of 109 weeks) retained her spacer for 109 weeks due to medical reasons following her first stage procedure and did not wish to undergo the second stage procedure when offered to her. She continued to fully ambulate on her spacer without difficulty and underwent reimplantation surgery more than 2 years following the first stage procedure, when her medical issues largely stabilized. The median time for spacer retention was 15.71 weeks. 19 of 31 patients (61.2%) retained the knee spacer for less than 20 weeks. The mean ± SD postoperative follow-up (following second stage reimplantation surgery was 3.52 ± 1.36 years (range, 1.29-6.03 years). Range of motion (extension) with the spacer was 3.6°±7.2° (range 0° to 30°); spacer flexion was 95.5°±26.3.5° (range 40° to 130°). Postoperative range of motion (following second stage procedure) included extension of 1.6°±4.4° (range 0° to 20°); flexion was 105.2°±19.7° (range 45° to 140°). Five of the 31 patients (16.1%) required either a flap or soft tissue procedure by a plastic surgeon to allow for enhanced wound closure at the completion of the first or second stage procedure. No extensile approaches were used for the revision TKA reimplantation procedures. One patient required a reoperation due dislocation of the femoral component 3 weeks post resection arthroplasty and was revised with a second femoral spacer. One patient had a spacer fracture (fracture of the femoral component) which did not impair ambulation and was treated by definitive revision TKA reimplantation following the standard treatment protocol.
Infection Eradication
Two of the 31 spacer patients (6.45%) failed an initial two stage exchange and required a second two stage exchange for infection eradication. Those 2 patients are currently infection free at 2.8 and 2.9 years following a repeat 2-stage exchange. In addition, two of five revision TKA patients who had previously undergone a 2-stage exchange for infection by outside surgeons, presented with recurrence were treated with a repeat 2-stage exchange and are currently infection free at 2.8 and 3.5 years. At a mean follow-up of 3.52 ± 1.36 years (range, 1.29-6.03 years) post reimplantation surgery, all patients were infection free with no evidence of recurrence. Complications, such as medial collateral ligament tears and periprosthetic fractures, were not observed in any of the patients.
Discussion
Infection continues to be a vexing complication following primary and revision TKA and is a leading cause of revision TKA within 2 years of the index procedure (Kurtz et al. 2012). At present, two-stage exchange is the current preferred treatment algorithm for resolving infection in TKAs in the United States, and achieves a high rate of infection eradication (Cui et al. 2007). Multiple spacers are available including static and articulating spacers for the treatment of PJI which could be either premade (off the shelf) or surgeon molded (intra-articular cement spacers molded in the operating room). Antibiotic impregnated PMMA spacers have become an established mechanism to provide local delivery of antibiotics following the resection arthroplasty and before the reimplantation procedures. Knee spacers not only help in maintaining the joint space but also provide stability for the knee joint whether static or mobile. Nonarticulating cement block spacers can be easily made intraoperatively with surgeon selected antibiotic-impregnated PMMA and are fashioned to fit the existing bone defects. Although useful in infected knees with the substantial bone loss, static spacers present several disadvantages such as knee immobility and subsequent stiffness, spacer dislodgement, and bone erosion (Jacobs, Christensen, and Berend 2009). Scar formation, tissue adherence, and quadriceps scaring and subsequent shortening make the reimplantation surgery particularly difficult. Often extensile exposure is needed during the reimplantation surgery due to scar formation. Various types of mobile spacers are available to treat the problem of PJI, and purported benefits include improved function, knee mobility, and ease of reimplantation. At present, no specific surgical technique is considered to be superior to another, yet there are significant differences in terms of functional outcome, range of motion, ease of insertion, reliability, cost, and simplicity of removal.
Currently, articulating spacer use has become more widespread due to the multiple advantages including maintaining joint motion, preventing extensor mechanism shortening, facilitating reimplantation, and improving postoperative function. The presently described OsteoRemedies® premade antibiotic spacer provides multiple size options to improve host bone coverage, enhanced component fit, and maximizes knee joint stability thereby providing improved knee function, rehabilitation, and enhanced range of motion. The additional modularity of this spacer also enhances surgeon directed intraoperative flexibility and facilitates intraoperative gap balancing and joint line restoration, which traditionally has been difficult with presently available spacers. The described spacer technique obviates the time-consuming need for hand crafting cement-on-cement spacers, which can be technically challenging, labor intensive, and prone to dislocation. In addition, partial weight bearing is generally advised for commercially available cement spacers, but full weight bearing may be possible with the present spacer as demonstrated in the present series without adverse consequences. This additional benefit improves patient rehabilitation and functional recovery. Most importantly, patients can remain ambulatory without restriction until they are ready for the second stage procedure.
When analyzing infection eradication, there appears to be no significant difference between various static or articulating spacer devices or techniques. The lack of superiority between multiple spacer constructs also highlights the fact that achieving infection eradication is multifactorial including the quality of the surgical debridement, host comorbidities, patient optimization, the elution of antibiotics in the cement, the type of antibiotics, and the type of bone cement.
As mentioned above, articulating spacers are often used to facilitate implantation of the second stage of the 2-stage exchange for infection. The present series evaluated two stage procedures with an articulating spacer technique and found no requirement for extensile measures to perform the reimplantation surgery. We hypothesize that the interim range of motion provided by this articulating spacer leads to improved soft tissue compliance, decreased extensor mechanism scarring, and facilitates the second-stage implantation.
The present series had 2 (6.45%) recurrences of infection, 1 (3.22%) femoral spacer dislocation, 1 (3.22%) spacer fracture, and no tibiofemoral dislocations or subluxations. This prefabricated cement spacer may have improved mechanical properties compared with higher-dosed handmade pre-molded spacers. Spacer removal before second stage surgery was straightforward and no extensile approaches were required. The present spacer facilitates knee range of motion, thereby with knee flexion during the second stage procedure, the femoral component is removed first followed by tibial spacer removal. This novel design promotes knee stability, improved patient function, and overall outcomes. The articulating antibiotic knee spacer presently described for the management of PJI following TKA and revision TKA is modular, stable, provides intra-articular elution of antibiotics, and is relatively easy to insert during the first stage procedure. Removal during the second stage procedure can be performed safely and efficiently. It is, like any knee spacer, either static or mobile, however associated with spacer-related complications which may be inherent in this complex patient population.
Conclusion
Between 2014 and 2016, 31 consecutive patients with deep PJI following primary TKA (26) or revision TKA (RTKA) (5) were managed with the OsteoRemedies® knee spacer. An acceptable level of spacer-related complications are reported and a stable knee joint with range of motion up to 100° were observed in these patients. This customized and modular articulating knee spacer has the potential to reduce spacer-related complications, provides significant infection eradication, and offers improved knee function for the treatment of PJI in both TKA and revision TKA.
Author’s contribution
KJA is the only author and performed the research, data gathering, analysis of the results, and writing of the manuscript.