INTRODUCTION
Total hip arthroplasty (THA) and total knee arthroplasty (TKA) are immensely successful in relieving pain and restoring function in patients with arthritis. Though total joint arthroplasty (TJA) is generally safe, systemic complications secondary to the insult of surgery (unrelated to the prostheses) may occur (Parvizi et al. 2007; Eftekhar, Kiernan, and Stinchfield 1976). Postoperative gastrointestinal (GI) complications, in particular, are uncommon, but can be associated with substantial morbidity and mortality. Reported complications include ileus, acute colonic pseudo-obstruction (ACPO), GI bleeding, pancreatitis, diverticulitis, and intestinal ischemia (Yilmazlar et al. 2012; Petrisor et al. 2001; Clarke, Berry, and Larson 1997; elMaraghy et al. 1999; M. Nelson and McClelland 1992; Parvizi et al. 2008; Iorio, Healy, and Appleby 2000; Ficheur et al. 2016; Gehrke et al. 2018; Duchman et al. 2017; Kapadia et al. 2014; Eftekhar, Kiernan, and Stinchfield 1976). The incidence of each complication varies by series, with ileus and ACPO occurring in up to 4% of TJA patients (J. D. Nelson 2006; Eftekhar, Kiernan, and Stinchfield 1976; Iorio, Healy, and Appleby 2000; Yilmazlar et al. 2012; Clarke, Berry, and Larson 1997; Petrisor et al. 2001). These complications increase patient length of stay, risk of further complications, healthcare costs, as well as overall patient morbidity and mortality (Petrisor et al. 2001; Clarke, Berry, and Larson 1997; elMaraghy et al. 1999; Yilmazlar et al. 2012; Eftekhar, Kiernan, and Stinchfield 1976; Tengberg et al. 2017). For example, following emergent laparotomy for intestinal obstruction, a thirty-day mortality rate of up to 20% has been reported (Tengberg et al. 2017). Given that TJA complications and patient outcomes are used to assess hospital performance and affect value based payment models, a greater understanding of the incidence, risk factors and possible prevention of these complications is necessary (Sahota et al. 2018; Bozic et al. 2014; Gray et al. 2018).
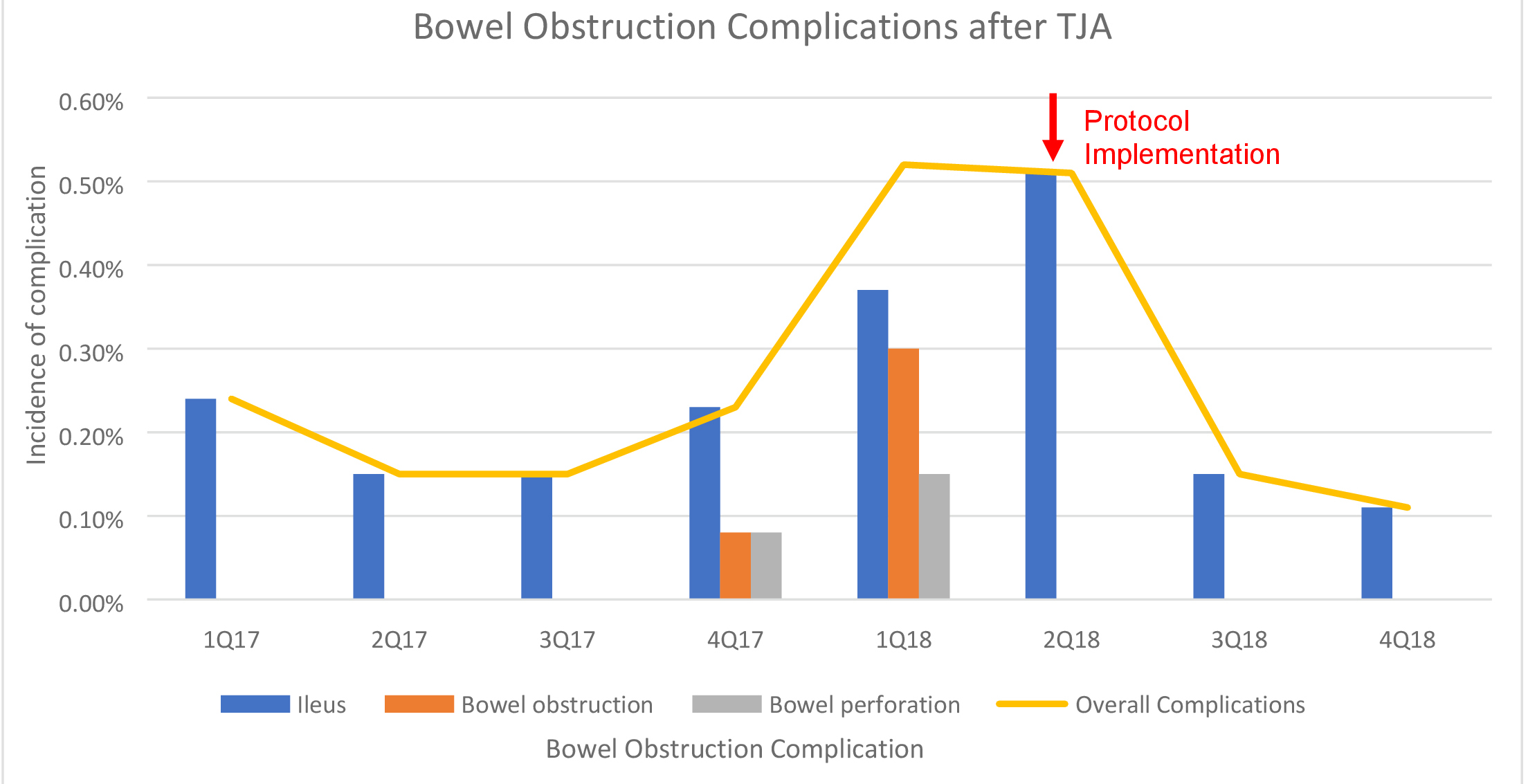
At our institution, an increasing trend of serious postoperative bowel obstruction complications after elective TJA was noted over a nine-month period from 2017 to 2018 (Figure 1). These cases were reviewed in depth and the observation led to an evaluation of current protocols in an effort to decrease the incidence of these events.
_from_2017-2018.jpg)
The Plan-Do-Study-Act (PDSA) method of quality improvement is commonly utilized to implement change in healthcare (Taylor et al. 2014; Coury et al. 2017; Münter et al. 2017; Baird et al. 2019). PDSA cycles involve creating a plan to address the problem (plan), carrying out the test and collecting data (do), analyzing the data (study), and make modifications as needed prior to carrying it out on a larger scale (act) (“QI Essentials Toolkit: PDSA Worksheet” 2007). The purposes of this study were to (1) create a protocol to prevent bowel obstruction complications in TJA patients using the PDSA quality improvement model as well as (2) assess the effect of the protocol on the incidence of such complications.
METHODS
Setting
This study is a prospective observational study including all patients undergoing total joint arthroplasty at a single specialty orthopedic hospital in 2018. This facility performs over 20,000 surgeries annually, of which approximately 6,000 are total joint arthroplasties. This study was IRB exempt.
Development of bowel complication prevention protocol
We created a multidisciplinary task force including orthopedic surgeons, orthopedic nurse practitioners, gastroenterologists, intensivists, hospitalists, and general surgeons with the goal of developing a standardized protocol to reduce postoperative gastrointestinal complications, with particular emphasis on bowel obstruction. The cases of severe bowel complications, as well as current practice in management of postoperative patients were reviewed. Opportunities for change in the current system were identified and potential solutions were created. For example, bowel function often was not formally assessed until the patient reported symptoms of constipation; therefore, treatment was reactive as opposed to proactive. Additionally, the initial postoperative bowel regimen did not account for persistence of constipation or progression to ileus or bowel obstruction. There was not a standard method by which bowel regimen medications were escalated, nor was it clear when other subspecialties should be involved. This likely played a role in the delay in diagnosis and appropriate management of the bowel obstruction complications that were observed. Solutions included creating a stepwise pathway designed to escalate the bowel regimen as needed daily, as well as incorporating daily assessments of bowel function and identifying key points at which other subspecialties should be consulted. Current literature in conjunction with expert opinion were taken together to develop a multi-step protocol that would be used by orthopedic surgery residents, nurse practitioners, and nurses, with appropriate escalation to specialists as needed.
Implementation of bowel complication prevention protocol
The protocol was presented to all orthopedic surgeons, orthopedic nurse practitioners, hospitalists, nurses and gastroenterologists involved in the care of patients at the orthopedic hospital. Orthopedic surgery residents and nurse practitioners were given lectures on the new protocol. In addition, an intensive educational program focused on enhancing gastrointestinal assessment skills and improving communication amongst members of the care team, was implemented for all orthopedic nursing staff. All staff, including orthopedic surgery attendings, were given the opportunity to voice concerns and suggest changes to the protocol prior to implementation. Physical copies of the protocol were available in each unit of the hospital, and digital copies were made available on the electronic learning platform at our institution.
Alterations were made to order sets and note templates within the electronic medical record system to assist with adherence to the protocol. For example, medications to stimulate bowel motility, which were previously given on an as needed basis, were changed to scheduled dosing. Providers were also prompted to obtain a gastrointestinal history and complete exam during documentation of daily progress notes. Additionally, the postoperative transition team assisted in continued monitoring of patients after discharge. Prior to the implementation of the protocol, all patients were contacted via telephone by a member of the postoperative transition team to assess patient recovery. This phone call now includes a standardized gastrointestinal assessment to monitor patient symptoms, with escalation to the attending physicians as indicated.
Evaluation of bowel complication prevention protocol
After implementation of the protocol, gastrointestinal complications were monitored. Problems regarding adherence to the protocol were also evaluated and modifications were made as necessary. For example, residents expressed concern regarding having adequate time during rounds to complete the full GI assessment that occurs on postoperative day one. There were also concerns about the patients’ ability to recall the information required to answer the questions as rounds are typically early in the morning and the patients are aroused from sleep. In response to those concerns, the nurse practitioners who care for the patients during the day would complete the majority of the postoperative day one assessment. To eliminate multiple people completing the assessment while making the responses available to all involved in the patient’s care, the assessment was made a part of the handoff tool in the electronic medical record that is accessible and can be edited by all members of the care team. Additionally, it was noted that there was no plan in place after discharge, as many patients are discharged on postoperative day one or two, prior to having a bowel movement. Rather than keep patients admitted until they had a bowel movement, which would unnecessarily prolong hospital stay, patients who fell into this category were prescribed a gentle laxative, given follow up with their primary care physician, and were contacted the first week after surgery to monitor symptoms as previously described.
RESULTS
Creation of Prevention Protocol
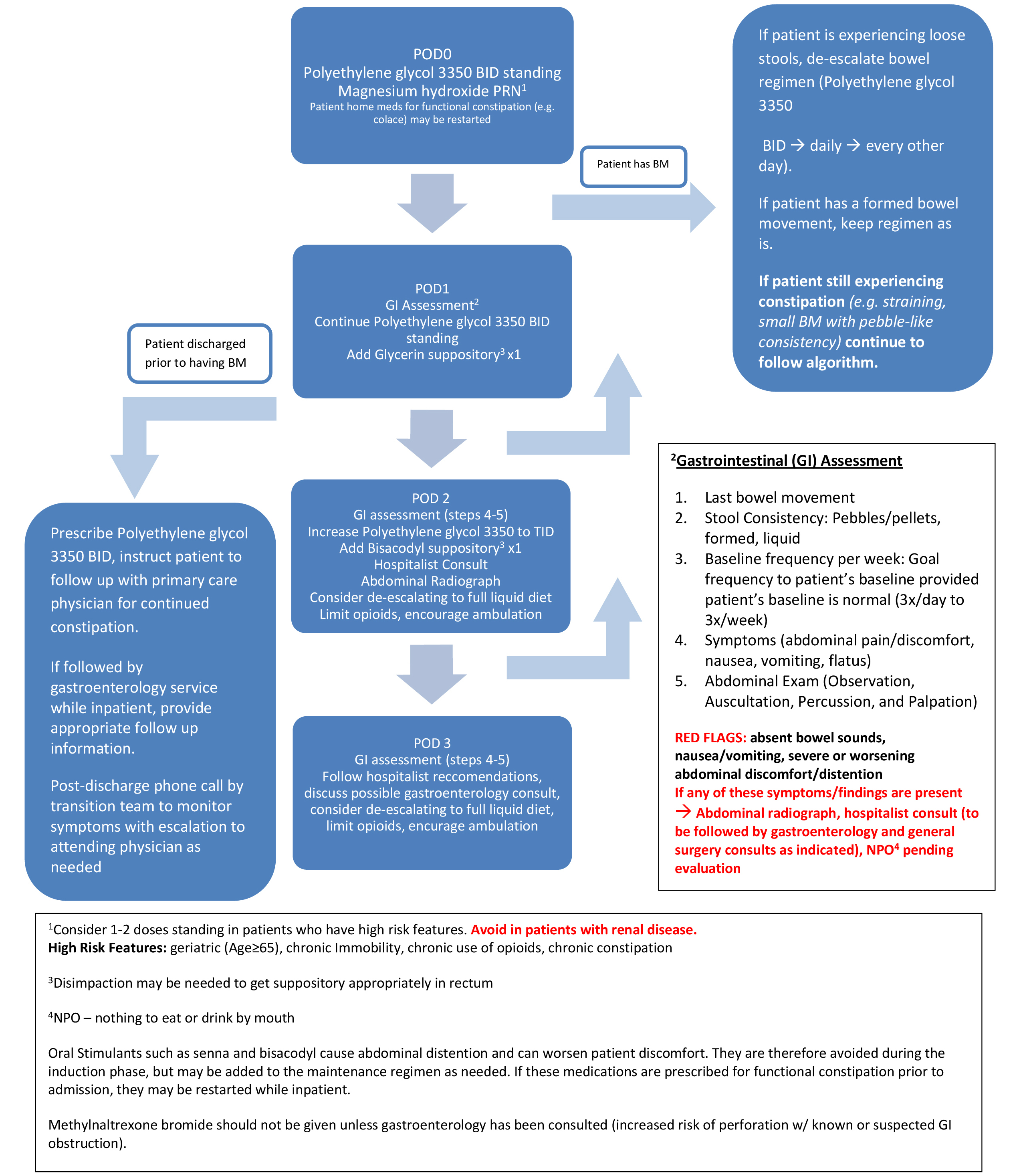
The protocol was created over two-month period, with multiple rounds of modifications made by the multidisciplinary task force. It is intended to be implemented on postoperative day zero and involves clinical evaluation with pertinent gastrointestinal history and exam, as well as medications, diet modification, imaging and appropriate escalation to specialists such as hospitalists, gastroenterologists, and general surgeons as needed (Figure 2).

Implementation of Protocol and Evaluation of Efficacy
The protocol was implemented in May 2018. From the time the protocol was implemented until the end of the year, 3,352 patients underwent TJA. During this time, there were no cases of bowel obstruction or perforation reported (Figure 1). Additionally, there was a 31.9% decrease in cases of ileus (Figure 1).
DISCUSSION
Though complications along the spectrum of bowel obstruction after total joint arthroplasty (TJA) are not uncommon, the reasons for the cluster of these complications noted at our institution in 2017-2018 were unclear. The increase in GI obstruction-related complications after TJA was noted from the 3rd quartile of 2017 to the 2nd quartile of 2018. The most severe complications were bowel obstruction with perforation and acute abdomen requiring exploratory laparotomy. Four patients underwent exploratory laparotomy with bowel resection and ostomies during this time. Three of the four patients had bilateral total knee arthroplasty, whereas the fourth patient underwent unilateral total knee arthroplasty.
There was one patient mortality. This patient underwent bilateral total knee arthroplasty without apparent complication and was discharged to an inpatient rehabilitation facility on postoperative day three. On postoperative day five, the patient reported abdominal pain, constipation, and one episode of emesis. Imaging demonstrated a partial small bowel obstruction. Due to clinical deterioration, the patient was transferred to the intensive care unit and general surgery was consulted. On exam later that day, the patient was noted to have findings of acute abdomen, and was emergently taken to the operating room for exploratory laparotomy, where no evidence of ischemia or necrosis was noted. The patient was found to be in septic shock and subsequently transferred from the orthopedic hospital to main hospital campus surgical intensive care unit that evening. The patient continued to deteriorate clinically and was taken back to the operating room on postoperative day six for an exploratory laparotomy. Substantial bowel ischemia was noted at that time and the patient consequently underwent a subtotal colectomy and partial small bowel resection. A do-not-resuscitate/do-not-intubate order was placed at the request of the family and the patient expired on postoperative day seven.
Postoperative bowel obstruction
Bowel obstruction after TJA is most commonly secondary to postoperative ileus or acute colonic pseudo-obstruction (ACPO) (Eftekhar, Kiernan, and Stinchfield 1976; Star, Colwell, and Johnson 1995; Iorio, Healy, and Appleby 2000; elMaraghy et al. 1999; Clarke, Berry, and Larson 1997; Petrisor et al. 2001; Yilmazlar et al. 2012). Signs and symptoms typically present 2-4 days after surgery (Parvizi et al. 2008; Petrisor et al. 2001; Clarke, Berry, and Larson 1997). The etiology remains unknown, however, several theories regarding the pathogenesis have been reported. The air fluid lock theory describes the potential role of prolonged immobilization. As a patient remains recumbent for an extended period of time, the dependent bowel loops collect air and fluid which can result in dilation and subsequently increase the risk of perforation and ischemic necrosis (J. D. Nelson 2006; elMaraghy et al. 1999; Petrisor et al. 2001). Other contributing factors include intraoperative anesthesia, as several anesthetic agents slow gastric emptying; as well as postoperative pain management with narcotics, which are also known to decrease gastric and colonic motility (Nguyen, Bono, and Bono 2019). Additionally, in the acute postoperative period, patients often have increased sympathetic stimulation and impaired parasympathetic function, which decrease gastric motility (Petrisor et al. 2001; Dorudi, Berry, and Kettlewell 1992). Risk factors include male gender, increased age, bilateral or revision surgery, history of abdominal surgery, arthroplasty done in the setting of trauma, and patient-controlled analgesia (Parvizi et al. 2008; elMaraghy et al. 1999; Clarke, Berry, and Larson 1997; Petrisor et al. 2001; Yilmazlar et al. 2012; Chambers, Silver, and Bucknell 1990; Nguyen, Bono, and Bono 2019).
Prevention protocols in current literature
There is a paucity of literature regarding postoperative protocols to prevent gastrointestinal complications along the spectrum of ileus and bowel obstruction in orthopedic surgery patients. Linari et al describe a protocol in which a Bisacodyl suppository is given on postoperative day one as opposed to as needed in the acute postoperative period (Linari, Schofield, and Horrom 2011). Much like this study, the protocol was created in response to an increased trend of ileus noted in TJA patients. Nurses played a significant role in the implementation of the protocol. In addition to administering the medication, nurses were responsible for completing a bowel function assessment in the electronic medical record if a patient had not had a bowel movement by postoperative day three. They noted a significant decrease in postoperative ileus and constipation in total hip arthroplasty patients (Linari, Schofield, and Horrom 2011). Prevention measures have also been reported in the general surgery literature. In a randomized controlled trial, Asao et al demonstrate that chewing gum on postoperative day one results in earlier flatus and bowel movements in patients undergoing elective colectomy for colorectal cancer (Asao et al. 2002). Similarly, Lobo et al found that restricting fluid and sodium intake also resulted in earlier flatus and bowel movements, as well as a shorter hospital stay in the same patient population (Lobo et al. 2002).
PDSA
The Plan-Do-Study-Act (PDSA) method is an effective tool for testing change that has been used across healthcare organizations to improve patient care. In surgical patients, studies have shown its success in creating preoperative scoring tools for common postoperative complications such as acute kidney injury, as well as enhance communication between the care team, thus facilitating patient transfer to and from the operating room (Baird et al. 2019; Münter et al. 2017). The hallmark of the PDSA method is that it requires continual evaluation with modifications made as needed. In the implementation of our protocol, ongoing communication between physicians, nurse practitioners, nurses, and patient care technicians was pivotal.
Limitations & future directions
Although we recognized a trend of bowel obstruction complications prior to the implementation of the protocol; the overall incidence of these complications is low. This limited our ability to adequately detect the effect of the protocol. Stronger evidence would be provided by a randomized controlled trial; however, this would also likely be limited by the low incidence of these complications. Although hospital staff were educated on the protocol, there are possibly cases where strict adherence to the protocol was not observed. For example, patients may refuse medications or further workup with imaging. Additionally, the learning curve may have also affected adherence to the protocol. To improve adherence moving forward, this protocol is taught to each new class of orthopedic surgery residents as well as nursing staff as part of the onboarding process.
The protocol was initially limited to total joint arthroplasty patients. It has since been expanded across other subspecialties within orthopedics, and possibly will be applied across other non-orthopedic surgical specialties. Future studies can evaluate the effect of the protocol in lowering the incidence of bowel obstruction complications in a larger patient population, and possibly offer improvements as further PDSA cycles occur. These efforts may prove beneficial in further standardization of postoperative care in hopes of improving patient outcomes as well as reducing associated healthcare costs.
CONCLUSION
Though infrequent, bowel obstruction complications after TJA can have detrimental effects resulting in further surgery, prolonged hospitalization, and patient mortality. This study describes a protocol that aims to prevent these complications in this patient population through early identification and intervention, with a demonstrated reduction in incidence of these complications after implementation.
ACKNOWLEDGEMENTS
We would like to acknowledge Drs. Ezra Dweck, Amy Wasterlain, and Stephanie Swensen, as well as the postoperative transition team for their assistance in creating and implementing the protocol.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this articles.