
1. INTRODUCTION
Total Knee arthroplasty (TKA) has been shown to be an effective procedure for improving function and pain in patients with osteoarthritis of the knee (Gibon, Goodman, and Goodman 2017; Hoffart, Langenstein, and Vasak 2012; Nakano et al. 2013; Blakeney, Khan, and Palmer 2014; Longo et al. 2018; Xie et al. 2012; Ensini et al. 2007). However, the current literature reports a patient satisfaction rate that does not exceed 80-85 (Gibon, Goodman, and Goodman 2017; Gunaratne et al. 2017; Van Onsem et al. 2016). Arthroplasty surgeons must strive to make further advancements in this procedure as there remains clear opportunity for improvement.
Use of computer navigation and robotics to optimize component alignment and soft tissue balance of the knee is a potential solution to improve patient reported outcomes (PROMs) and satisfaction (Song et al. 2013; Selvanayagam et al. 2019; Zhang et al. 2011; Kamat et al. 2009). Prior authors have theorized that perfecting these parameters will improve patient PROMs along with their satisfaction of the procedure (Choi and Ra 2016). Multiple systems have been developed to replace the conventional cutting jigs with navigation or robotic arms and guides with the goal of aiding in intraoperative decision making and cut precision. Early results of computer/robotic assisted total knee arthroplasty (CAS/RAS TKA) have been mixed, with excellent reproducible alignment, at times increased operative time, but overall little difference in patient reported outcomes (Barrett et al. 2011; Blakeney, Khan, and Palmer 2014; Cheng et al. 2012; Ek et al. 2008; Gothesen et al. 2014; Khlopas et al. 2018; Marchand et al. 2019; Lutzner, Dexel, and Kirschner 2013). The field of CAS/RAS TKA has continued to develop however, with new technologies and techniques being investigated.
Authors have continued to produce conflicting results comparing the results of CAS/RAS TKA when compared with conventional total knee arthroplasty (Conv. TKA). Some studies show distinct advantages of CAS/RAS surgery with improved PROMs and radiographic alignment (Blakeney, Khan, and Palmer 2014; Rebal et al. 2014; Pang et al. 2011; Lehnen et al. 2011; Petursson et al. 2018; Gothesen et al. 2014; Hoffart, Langenstein, and Vasak 2012). However, others show no significant change in PROMs or that any difference does not have a clinical correlation (Cho et al. 2019; Kim, Yoon, and Park 2020; Song et al. 2013; Park and Lee 2007; Song et al. 2011; Liow et al. 2014; Zhu et al. 2018; Yang et al. 2017; Roberts et al. 2015; Barrett et al. 2011; Lutzner, Gunther, and Kirschner 2010; Ek et al. 2008; Roberts et al. 2015). Systematic reviews are an effective means of identifying, evaluating and summarizing the findings of all relevant studies published on a given procedure. Systematic reviews and meta-analysis have been performed comparing Conv. to either CAS TKA or to robotic TKA for component positioning and clinical outcomes with varying conclusions (Cheng et al. 2012; Rebal et al. 2014; Agarwal et al. 2020; Ren et al. 2019).
As there remains controversy in this area, a systematic review and meta-analysis of the literature was undertaken to compare the clinical results between Conv. TKA and CAS/RAS TKA. This study sought to compare post-operative PROMs for patients undergoing CAS/RAS versus Conv. TKA. Secondary factors investigated included the number of months postoperatively the patients were followed as well as which CAS/RAS TKA systems were used.
2. MATERIALS AND METHODS
A systematic literature search was performed by following the PRISMA guidelines and using Pubmed to search the MEDLINE library to evaluate all studies comparing outcomes between Conv. TKA and RAS/CAS TKA. Multiple search strings were used, including “Robotic Knee Arthroplasty” (365 papers), “Computer Assisted Total Knee Replacement” (797 papers), “Conventional AND Robotic Total Knee Arthroplasty” (90 papers), “Conventional AND Robotic Total Knee Replacement” (75 papers). Once duplicates were accounted for, the above search generated 530 unique articles. Three authors, independently blinded to each other’s results, examined the abstracts of the above studies. 30 studies were found to be relevant to our criteria.
All non-randomized studies were further evaluated using the methodological index for non-randomized studies (MINORS) criteria (Table 1). All studies evaluated were comparative studies, thus a maximum score of 24 was possible. Any paper with a score of less than 12 was excluded from the study. Inclusion criteria were a study which compared RAS/CAS TKA and Conv TKA and studies that used post-operative PROMs as one of their outcome. Outcome measures included 2011 Knee Society Score (KSS), KSS, Hospital for Special Surgery (HSS) Knee Score, Western Ontario and McMaster Universities Arthritis Index (WOMAC), and Oxford Knee Score (OKS). Exclusion criteria were articles that did not directly compare RAS/CAS versus Conv TKA, articles not written in English, articles with Minors criteria <12, and articles that were a systematic review.
Of the 30 studies evaluated, many only reported the KSS or HSS score individually. Two papers also used the new KKS scores and were evaluated separately. The functional and clinical components of the KSS were combined in our analysis. After further applying our exclusion criteria, 22 papers were ultimately included in our final analysis (Figure 1).

Collected data included number of patients included in each study, the number of RAS/CAS and Conv. TKA in each study, post-operative follow up in months, 2011 KKS, KSS, HSS, WOMAC, OKS scores post operatively at any times points that were given in the different studies. We also collected standard deviations of these values to allow for analysis. All data was compiled in Microsoft Excel (2011 Version; Microsoft Corporation, Redmond, Washington, USA).
Between-study variance was summarized by the τ2 statistic, and the percentage of total variance due to between-study heterogeneity I2 (inconsistency) was reported along with the estimated summary effect and corresponding 95% confidence interval. As a rule-of-thumb, large levels of between-study heterogeneity may be assumed if the computed I2 is at least 75%. Between-study heterogeneity (relative to the total variance) of 0% is indicative of no study heterogeneity or large within-study variance relative to the differences in effect between studies. In this case, fixed effects and random effects estimates will be equivalent.
Forest plots were constructed in order to examine the standardized mean difference (SMD, the difference between the robotic and conventional group means divided by the within-group standard deviation) and corresponding 95% confidence interval (CI), using Hedges’ g as the effect measure, across all individual studies. The summary (pooled) estimate based on the random and fixed effects models is also included.
A result was considered statistically significant at the p<0.05 level of significance. All statistical analyses were conducted with the metaphor and meta packages available in R version 3.6.1 software (http://cran.us.r-project.org/).
3. RESULTS
There were 22 articles that were included in the study (Figure 1), which generated a final cohort of 2063 conventional knees and 1946 CAS/RAS knees for a total of 4009 knees. Cho et al. was used in both the KSS and HSS analysis as adequate data was available for both PROMs. Six studies were evaluated for HSS knee score and 17 studies for the KSS score. The mean follow-up for the studies was 52.9 months (Range 6 – 156). There were 13 level 1 studies, seven level 2 studies, two level 3 studies included (Table 2).
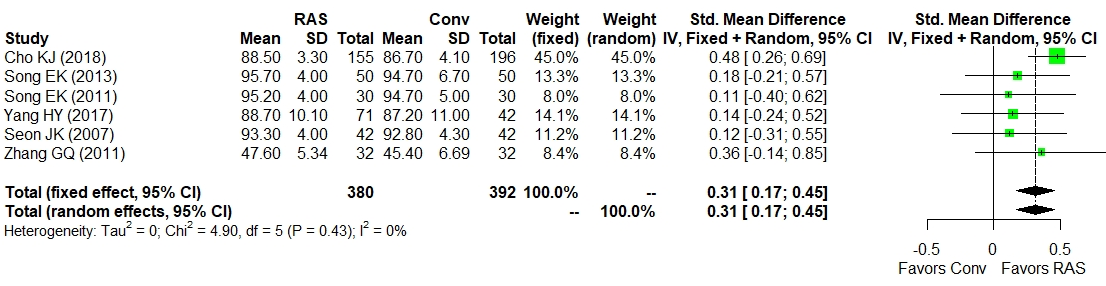
No statistical heterogeneity was detected (τ2 = 0; χ2 = 4.90, df=5, p=0.43, I2=0%) among the six studies that met inclusion criteria for the meta-analysis of HSS knee score (Figure 2). The diamond in the forest plot represents the overall statistic across the six studies and indicates that robotic-assisted total knee arthroplasty favored conventional with a higher HSS knee score (SMD = 0.31; 95% CI: 0.17-0.45).
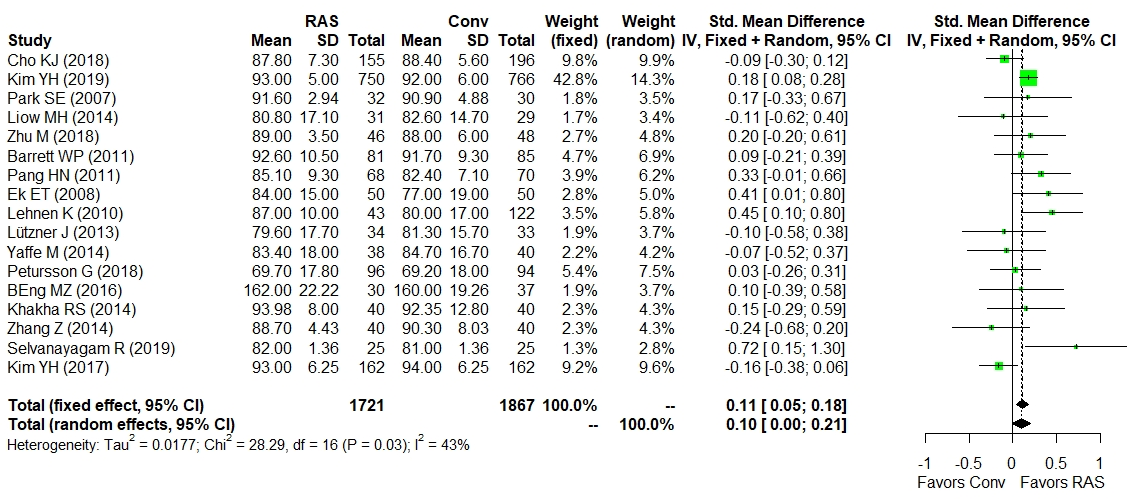
Moderate statistical heterogeneity was detected (τ2 = 0.018; χ2 = 28.29, df=16, p=0.03, I2=43%) among the 17 studies that met inclusion criteria for the meta-analysis of KSS (Figure 3). The diamond in the forest plot represents the overall statistic across the 17 studies and indicates that robotic-assisted total knee arthroplasty favored conventional with a higher KSS score (SMD = 0.10; 95% CI: 0.0-0.21). Random effects estimates are reported, as significant heterogeneity was detected among the studies.


4. DISCUSSION
There is still considerable room for improvement with regards to patient satisfaction and PROMs for TKA. As a result, CAS/RAS TKA was designed to decrease potential for human error in component alignment and ligamentous balance. While in theory this would translate to improved short- and long-term results, there continues to be conflicting reports on the difference in clinical outcome of CAS/RAS TKA. Our analysis was conducted to help determine if there is a clear benefit to CAS/RAS TKA over Conv. TKA.
This analysis demonstrated that the current literature favors CAS/RAS in terms of patient reported outcomes when compared to Conv. TKA. HSS and KSS were found to have superior SMDs in the CAS/RAS TKA groups. The analysis of the six studies reporting HSS found no heterogeneity and demonstrated a definitive trend towards superiority in the CAS/RAS groups. The studies that examined KSS were found to have moderate heterogeneity with a confidence interval at the line of no effect, as well as a smaller difference in SMDs than that found in the studies utilizing HSS. The KSS does trend towards superiority in the CAS/RAS groups, however not as definitively as with the HSS. The difference in heterogeneity may explain this result. These improvements also appear sustained at long term follow up, with an average of 52.9 months and a maximum of 156 months.
Though the numbers reported favor the use of navigation/computer technologies, the SMD found between the HSS score (0.31) and KSS (0.10) represent moderate and minimal differences between the two cohorts, respectively. Additionally, the differences between CAS/RAS and Conv TKA appear to be around the values of minimal important difference (MCID) for the different outcome measures (Lizaur-Utrilla et al. 2020; Singh et al. 2013). However, these values themselves are controversial, with minimal data available for what the MCID is for the HSS knee score. Therefore, it is unclear what the clinical implications are despite the apparent definitive improvement in the post-operative PROMs.
There are prior reports in the literature that also found superiority when comparing CAS/RAS and Conv TKA. However, many of these studies found more significant differences than in this meta-analysis. Hoffart et al looked at 195 patients split between CAS/RAS and Conv TKA and found a significant difference in KSS at 5 years favoring (Hoffart, Langenstein, and Vasak 2012). Blakeney et al split 107 patients between 3 groups of computer-assisted surgery for both the femur and the tibia, intramedullary guides for both the femur and the tibia, and an intramedullary guide for the femur and an extramedullary guide for the tibia. They found a significant difference with higher OKS in CAS/RAS TKAs at 46 months with worse scores associated with malalignment (Blakeney, Khan, and Palmer 2014). Ek et al retrospectively looked at 100 patients divided amongst CAS/RAS and Conv TKA finding better alignment, SF-12, and IKS scores in the computer assisted group (Ek et al. 2008). Pang et al randomized 140 patients into CAS/RAS and Conv TKA with the navigation group having superior alignment, function, and OKS at both 6 months and 2 years (Pang et al. 2011). While these studies demonstrate a significant improvement in PROMs, not all of the literature agrees.
Previous studies exploring CAS/RAS TKA outcomes found results that conflict with those presented above. Ensini et al completed a randomized prospective study between CAS/RAS and Conv TKA with 120 patients demonstrating improved component alignment in the navigation group with no significant clinical difference (Ensini et al. 2007). Song et al randomized 100 patients between CAS/RAS and Conv TKA and found more consistent alignment and better balancing in the navigation group, however with no significant difference in ROM, HSS, or WOMAC (Song et al. 2013). Selvanayagam et al randomized 50 patients into computer navigation and conventional groups and found better accuracy in CAS/RAS, but no difference at 4 years when looking at KSS and WOMAC scores (Selvanayagam et al. 2019). Kim et al took 162 patients and completed one knee with utilizing robotic assistance and the contralateral knee with conventional technique. At a mean follow up of 12.3 years they found no difference in KSS, WOMAC or ROM, but they did show an increased rate of anterior notching with CAS/RAS (Kim, Yoon, and Park 2020). Kamat et al looked at 637 knees and divided them into 2 cohorts of CAS/RAS and Conv TKA demonstrating no difference in OKS at 5 years, though they did show that in general misaligned knees had worse OKS (Kamat et al. 2009). While Kamat et al favored no difference in their analysis, their finding of inferior OKS in knees with poor alignment does support the theory behind CAS/RAS TKA. These studies are all heavily reliant on PROMs, and demonstrate the potential for this outcome measure to have limitations when determining clinical impact.
In addition to the above clinical studies, several meta-analyses have also been performed on this subject. Rebal et al completed a meta-analysis of 21 studies finding that RAS had more accurate alignment and improved KSS in CAS/RAS TKA at 3 months and again at 12 to 32 months (Rebal et al. 2014). Cheng et al also completed a meta-analysis of 21 studies with 2333 knees, however they found no statistical difference at early follow up (Cheng et al. 2012). A recent meta-analysis was performed by Agarwal et al. that evaluated Conv. vs RAS knee clinical and radiologic outcomes including 22 papers (Agarwal et al. 2020). They found a statistically significant difference in HSS scores favoring computer assisted surgery, which is consistent with the data presented in this study. They also demonstrated no significant difference in KSS scores. Agarwal et al only examined the effects of RAS TKA and did not examine the impact of computer navigation. This is why our meta-analysis included 6 studies when looking at HSS and 17 studies when looking at KSS scores, compared to 4 and 6 studies in the meta-analysis performed by Agarwal et al, respectively (Agarwal et al. 2020). Our study additionally expands on the results found by Agarwal et al by additionally completing a MINORs criteria assessment for the included studies (Agarwal et al. 2020).
Extensive analysis has been done on how post-operative PROMs differ between CAS/RAS and Conv TKA. However, there remains no clear consensus. This may be partially attributable to the fact that PROMs do not always correlate with patient satisfaction (Halawi et al. 2020). Unfortunately, patient satisfaction was not isolated or specifically evaluated in any of the included studies in this analysis. It is clear from this analysis that patient satisfaction needs further attention in future studies. This is especially important as orthopedic surgeons attempt to identify if the quantitative outcome provided by KSS and HSS scores translate to a clinical difference and overall patient satisfaction.
There were several limitations to our study. The first is that this study is a retrospective meta-analysis, and this presents with all the inherent bias and challenges of such a study. There is also the potential that other studies exist in the literature that were not found by this review, although over 1000 abstracts were examined for this study. While there is also the risk of including poorly designed studies within the analysis, this should have been mitigated as the MINORS criteria was used for the non-randomized studies. Finally, it would have been advantageous to directly compare patient satisfaction values to these PROMs to more directly the impact on patient satisfaction. However, none of the included studies reported directly on patient satisfaction, preventing us from making that comparison in this review. Ultimately, the lack of level 1 data with regards to modern RAS/CAS techniques sufficiently explains most of this study’s limitations. Thus, we recommend further investigation comparing PROMs from patients undergoing Conv. TKA those undergoing RAS/CAS TKA.
5. CONCLUSIONS
TKA is a consistently successful operation for the treatment of advanced knee osteoarthritis. This review has shown that RAS/CAS TKA improves HSS and KSS scores. However, it is still unclear how much the improvements from RAS/CAS clinically impact patients. There is a large volume of conflicting evidence in this field, and continued analysis is warranted to further elucidate the impact of RAS/CAS. Further randomized control trials comparing the RAS/CAS and Conv. TKA would be beneficial in showing if there are any differences between the two approaches with regards to PROM and patient satisfaction after TKA.
Conflict of Interest
The authors declare the following conflicts of interes: One author receives royalties, personal fees and non-financial support from Corin USA, personal fees and non-financial support from Omni Life Science, now acquired by the Corin Group 2020. Additionally, one author is an employee of Corin USA, a manufacturer of robotic assisted total knee arthroplasty surgery systems and conventional total knee arthroplasty systems.
Funding
There is no funding source for this study.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.