


1. Why did you choose to switch over?
For full disclosure, I was introduced to the ROSA® knee system (Zimmer Biomet, USA) as part of an early evaluation team. After this experience I requested a 30-case evaluation at my institution and subsequently the hospital decided to purchase the system. With the current movement to ambulatory surgical centers (ASC), my associated ASC has also purchased a robot.
Ultimately, our choice to switch to robotic total knee arthroplasty was driven by our desire to improve health care quality and outcomes and provide value to our practice. We believe robotic surgeries have the potential to improve both the patient and provider experience, just like how technology has improved the way we run our daily lives from cell phones in our pockets to smart cars on the road.
Joint replacement surgeries routinely lead to excellent outcomes (Kayani et al. 2019), and many technological advancements in joint replacement surgeries have been developed ranging from computer navigation systems to custom designed implants. Even so, with total knee replacements there remains a 20% patient dissatisfaction rate (Kayani et al. 2019). It is thought that implant malposition, gap balance mismatch, and poor alignment restoration are some of the underlying reasons why total knee replacements, in spite of the above mentioned technologies, continue to struggle, which could be a cause of dissatisfaction (Sharkey et al. 2014). My conventional TKA outcomes have been very good, but not perfect. Approximately 90% of my conventional TKA cases have reported good outcomes. Unfortunately, roughly 10% were dissatisfied. Though this is better than the commonly referenced 80/20 ratio, where 20% of TKA are dissatisfied, it still allows room for improvement. So despite having a high volume practice (250-300 TKA per year), I wasn’t happy with 10% of my TKA patients being dissatisfied. This is why I looked to technology as a way to improve my patient experience. Interestingly, we are seeing early evidence of improvements in our PROMs with this technology, but it is still too early to say if its statically significant. In order to determine this, research is actively being performed to verify or dispute these findings.
The issue with some of these prior technologies is that they still lack the capability to produce dynamic, objective data for gap analysis that allows the surgeon to appropriately restore symmetric, well-balanced, and rectangular extension and flexion gaps. There is also an issue with mid-flexion instability with knee replacements that has not yet been well addressed (Vajapey et al. 2020). Sensor-based technologies have attempted to address mid-flexion instability showing improvements in ligament balancing (Cho et al. 2018). However, the ability of these sensor-based instruments to improve outcomes remains controversial (Geller et al. 2018; Chow and Breslauer 2017; Song et al. 2019). Also, a recent report suggests that the use of ligament balancing tools associated with robotic TKA may provide accurate gap-tensioning throughout the range of knee flexion (Shalhoub et al. 2019). This is a promising component for robotics and may result in improved patient outcomes.
Robotic assisted TKAs have the potential to minimize the need for surgeon’s reliance on subjective decision making and to move towards a more scientific and standardized approach that utilizes real-time objective data. As previously noted, I’ve struggled with some dissatisfied patients when conventional instrumentation was used. As such, I have trialed multiple technologies, but with minimal changes in my practice outcomes. When choosing to move to robotics I considered several systems. Ultimately, I chose the system that allowed me to continue to use my current surgical technique but provided the real-time objective data to assist in accurate implant placement (Parratte et al. 2019; Seidenstein et al. 2020). However, it should be noted that the limitation of this system is the inability to guide the axial rotation of the tibial baseplate as it is currently out of the scope of the application.
In addition to our desire to improve health care quality, we continuously seek to add value to our practice. We see robotic assisted joint replacement as a way to increase physician alignment, engagement, and satisfaction. There is a growing number of surgeons who desire to work for practices that offer robotic service lines and therefore this can be a tool for recruitment and retention (Boylan et al. 2018; Naziri et al. 2019; Sousa et al. 2020).
Another way this technology adds value is by providing practice differentiation. Our market allows for patient self-referrals, and in this consumer driven healthcare world, many patients identify the latest state of the art technology as an indicator of quality and expertise and the presence or absence of robotics can influence the provider they choose.
2. Why did you choose the robotic system you use over the other systems?
Good question. I have been very happy with the rationale of design and biomaterials that Zimmer Biomet Persona TKA offers me and my patients. This includes Vitamin E polyethylene inserts, the J-Curve on the femur, 1 mm increments on the poly, and the fixed bearing locking mechanism, along with cemented and cementless technologies. In my hands coupling ROSA and Persona together and using the FuZion tensometer to confirm balanced rectangular flexion and extension gaps allowed a smooth transition to robotics from my preferred conventional method.
One of the reasons I prefer ROSA is the ergonomics in design, the software-surgeon interface, how it adopts to my work flow, and that I also have the same tactile feedback from the manual saw blade that I would have otherwise with a conventional TKA.
But, at the end of the day, I find that a primary reason I use this system is because of my comfort in the implant design rationale. Ultimately, each surgeon needs to look at their own philosophies of what they use and why they use it. Each surgeon should make decisions to adopt the corresponding technology based on what they feel will provide the best care for their patients.
Each system and company are exploring new technology as a way to improve outcomes. At this time, the implants and biomaterials are the best we have seen, but unfortunately, we still see dissatisfaction in our patients. As more reimbursement is tied to outcomes, maybe technology is the missing link. Thus, using technology, strategically, in our practices may help improve upon the already excellent outcomes that total joints have to offer.
3. What do you feel are the intraoperative benefits?
In my hands, the benefit of using a robotic assistant during surgery, is that I am still in control of every surgical decision being made. The difference though, is that with robotics every decision I make is based on real-time, objective data. This allows me to correct the limb alignment, gap balancing, and femoral rotation as needed during the procedure. These aspects are important to restore at the time of surgery to ensure good outcomes and the robotic assistant allows this to be done accurately and efficiently every time.
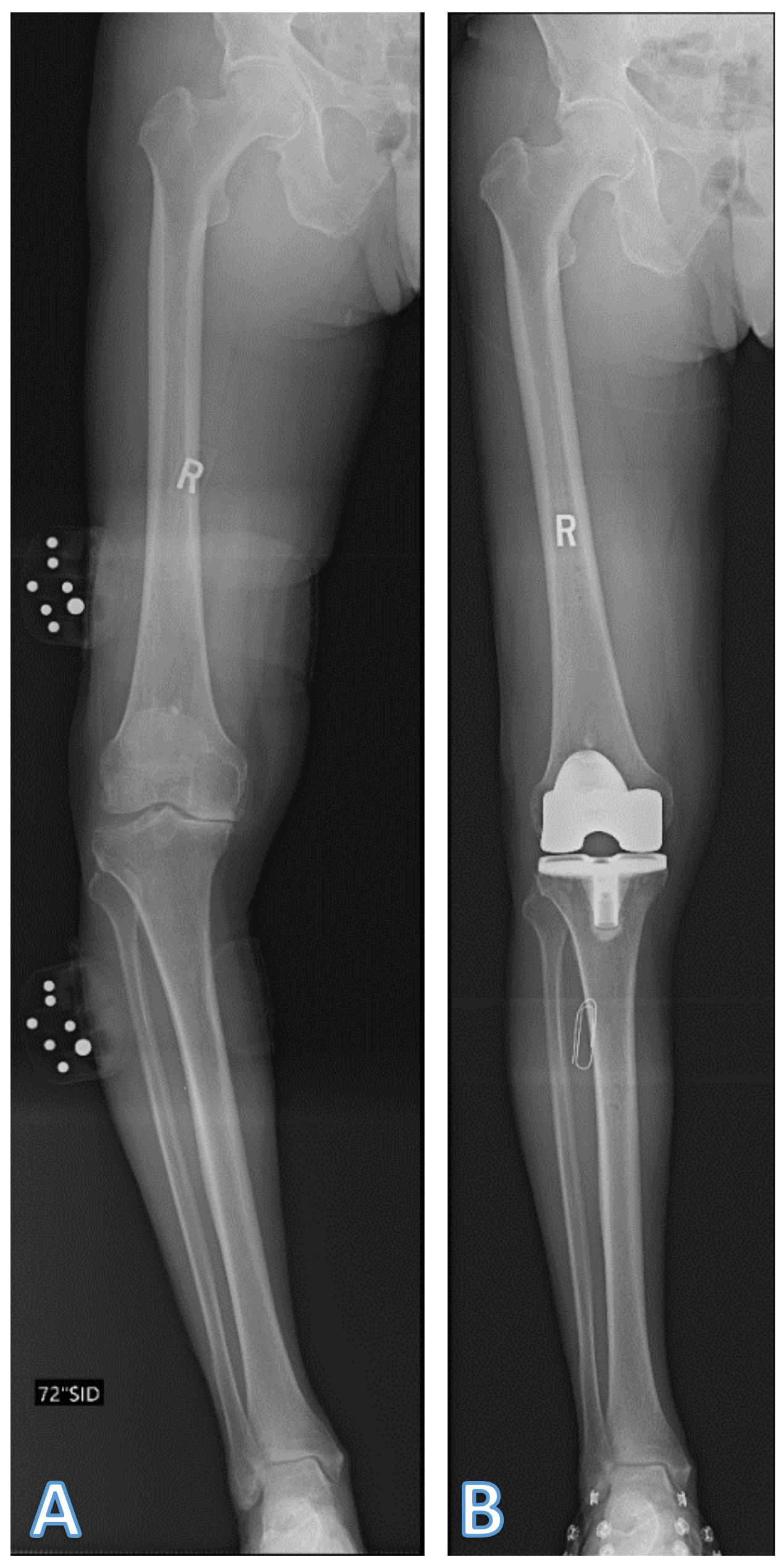
For example, a recent case I completed was a 77-year-old male with severe right knee pain, and a varus deformity. His preoperative x-rays (Figure 1) showed significant arthritic changes throughout the right knee and a preoperative 20-degree varus alignment. The patient had trialed multiple rounds of nonoperative interventions without any success and so therefore, we decided he was an appropriate candidate for robotic assisted right total knee replacement.
_preoperative_20-degree_varus_misalignment_and_sev.png)
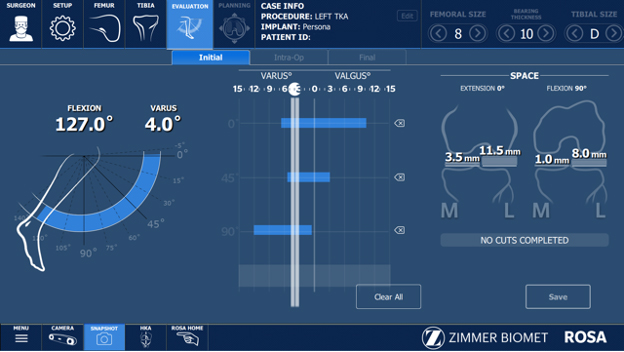
During this surgery, I performed a gap balanced posterior stabilized right total knee replacement utilizing Rosa assistance. During this surgery, I was able to restore his alignment, as appreciated by the postoperative x-rays (Figure 1). His postoperative alignment measures 2 degrees of varus, which is within my comfort zone of +/- 3 degrees from mechanically neutral, and his gaps are well-balanced, as seen in the intra-operative screen shots (Figure 2). His femoral rotation was also restored with a well tracking patella. This patient went on to do very well postoperatively and was very happy with his right knee replacement.


Total knee replacement surgery is functionally a soft tissue balancing procedure and the robotic assistant allows me to objectively balance the gaps to within 0.5 mm. Previously, adjustments were made with less precision and larger increments of adjustment were acceptable practice. However, with robotics more precise adjustments can be made. For example, a gap balance tool for the robotic system used at my practice allows the surgeon to visually appreciate the symmetry of the gaps with an associated tension on the medial and lateral side, illustrated by a computer graphic, and an objective number within 0.5 mm (Figure 3). I think having this new ability to make higher precision, 0.5 mm adjustments, and then adjust the poly thickness by 1 mm allows us to personalize a patient’s total knee replacement which I feel leads to better outcomes.


Further, unlike conventional and patient specific cutting jigs which are static at time of surgery, robotics allows the surgeon the ability to make adjustments based on the soft tissue envelope. The surgeon no longer has to rely on an artistic approach to the soft tissue feel of the knee, because the robotic approach gives you data previously unavailable. I find this to be most beneficial in evaluation of the flexion gap, and now I have the opportunity to adjust for the mid-flexion range. Something we have not had the ability to control for in the past.
Every knee replacement is functionally different. A robotic assistant provides objective, real-time physiological data which allows me to design and adapt, intraoperatively, patient-specific plans tailored to ensure that I can more precisely restore the patient’s knee biomechanics. In practice this ultimately decreases intraoperative variation in procedural technique and minimizes the need for subjective decision making by the surgeon. It also allows the robotic assistant to generate an objective and modifiable plan to meet the patient’s own biomechanical and anatomical needs.
4. What are the benefits to your patients?
The biggest benefit with robotic assisted knee replacements is the use of patient-specific, objective data that is generated and used for every knee replacement. Because of this, we feel we are starting to see anecdotal evidence of improved patient outcomes. Patients seem to be recovering faster, and their range of motion seems to be improving faster. Our rates and manipulations of the knee replacement seem to be less, and our patients seem to be very happy with their experience. At this point, more research needs to be performed to see if this is a scientific benefit or just a placebo effect. However, it should be noted that we are seeing very happy patients on a regular basis. I suspect this seems to be related to the nature of transitioning an artistic surgery to a scientific procedure.
5. What about OR time?
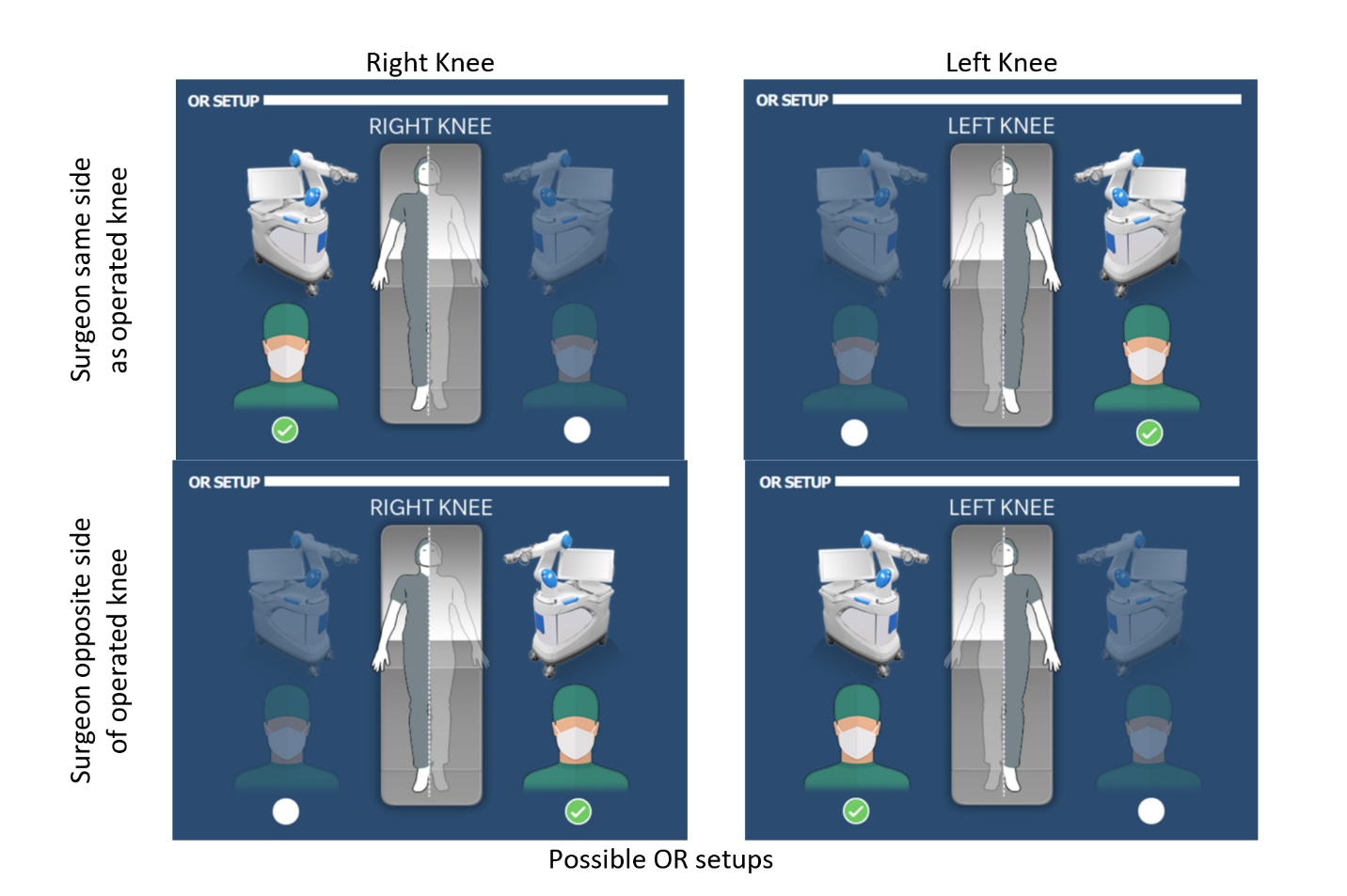
As with any transition to a new approach for surgery, there is a learning curve. This includes a reconfiguration of the operating theater as recommended by the manufacturer of each robotic system. For reference, with the ROSA® Knee system, the robotic arm/base is always positioned on the same side the surgeon stands on (Figure 4). This system is flexible enough to allow the surgeon to stand where they most comfortably would during surgery. I always stand on the side I’m operating on, but I know surgeons who only operate from the right side of the patient, because they are right-handed. The change in operating room setup may present a learning curve for the staff. We found the only additional step that really affected OR time was the time needed to drape the robot and the increased time was negligible compared to the setup time needed with my conventional cases.

Regarding surgical times, I found that my first ten cases took an average of 30 minutes longer. Once I understood and had mastered some the nuances of this new technology, I found that the surgical time is very similar to that elapsed during a conventional procedure. I think that ultimately, the learning curve for use of a new system is mainly driven by the willingness of the surgeon to adopt new technology, and the volume at which the new technology is implemented. Previous research supports this idea and has shown that Robotic Assisted (RA) TKA is associated with a learning curve for surgical time, but not for component alignment, limb alignment, or gap balancing and that this may also be dependent on the profile of the surgeon (Vermue et al. 2020).
I find that with robotic surgery, there seems to be more upfront time, used for planning, set-up and land marking, and that this ultimately decreases the time required at the end of the case. In my practice, the bulk of the setup is performed by my surgical support personnel prior to my arrival into the OR. I find that with primary osteoarthritis, a straightforward case with cemented implants, including femur, tibia, and patella, has a skin to skin time ranging from 45 to 60 minutes.
6. What about costs? With a large amount of total joint discussions being around cost containment, how does robotics fit into this?
It is without debate that robotic systems come with a high fixed cost. Because robotic systems are costly to acquire, it is important to explore all opportunities of value. Robotic surgery has the potential to increase volumes and create operational efficiency thus spreading the fixed cost over time. For example, robotic assisted surgery allows for the ability to customize and plan a knee replacement before surgery. This may minimize sterile processing turnover and help reduce expenses related to instrument sterilization thus allowing us to embrace more efficient care models.
Robotic surgery does come with a learning curve and a commitment from all stakeholders including staff and surgeon, but a commitment to building this service will create the volumes needed to achieve significant improvements in efficiency and validate long-term quality improvements that, over time, create significant value. Further, robotics can only help as we continue to transition from a fee for service model to a value-based model.
Also, it’s worth mentioning that robotic companies are working on strategies to minimize capital purchases which would allow for higher uptake rates by clinics for these new innovative technologies. For our use of this system, the goal was to see a return on our investment within one year, and we met that goal as we saw a 26.2% increase when comparing year over year pre/post implementation volumes.
7. Is it the future or not?
The real question is: “Is it the present and future, and is it clear that robotics is here to stay?” I think recent innovations in metal and plastic materials used for implants and implant integration are the best they’ve ever been, and implementation of todays’ robotic technology is an opportunity for us to further improve surgical practice. However, clinical studies that evaluate patient outcomes and experiences for both short and long-term outcomes are needed. We are excited to actively be involved in research studies that are testing this and look forward to being able to report the results of these studies.
In short, yes, the present and future of joint arthroplasty lies in continued improvements in technology. Robotic technology today may be different than Robotic technology in the next 5-10 years. The idea of augmented reality is just now coming into the conversation. It will be interesting to watch how technology changes the patient experience.
8. Do you have a series of a minimum of 100 patients you can do basic reporting on?
To date, we’ve completed about 250 robotic total knee replacements and believe the use of RA TKA will lead to improved patient experiences and outcomes. We are currently involved in several scientific research studies documenting the use of RA TKA in challenging circumstances as well as multicenter prospective studies to evaluate patient outcomes. Anecdotally, as mentioned, we have experienced excellent outcomes in this patient population and these research studies will help provide the empirical evidence needed to substantiate these claims. Ultimately, if we can improve patient outcomes and satisfaction while also minimizing the revision burden in the future, we can improve the value of total knee arthroplasty.
Conflict of Interests
NLC is a paid consultant for, and receives institutional research support from Zimmer Biomet. JAP is on the editorial board for the Journal of Orthopaedic Experience and Innovation.
Acknowledgment and funding sources
This work was supported by Zimmer Biomet (Protocol # IRU2020-30CA) and conducted with assistance by the Vail Summit Orthopaedic Foundation. The authors would like to acknowledge Mike B. Anderson, MSc, and Jared D. Heinze, MPH, for their assistance with writing this manuscript.