


Introduction:
In this article, we present a case study of a 31 year old male who developed slipped capital femoral epiphysis, secondary to an endocrine disorder.
Slipped capital femoral epiphysis (SCFE) is the most common hip disorder affecting adolescents with an incidence of 10.8 per 100,000 children in the US (Lehmann et al. 2006). It affects more males than females (64.3% vs 35.7%; Loder and Skopelja 2011), more Polynesians and African Americans than Whites (4.5:1 and 2.2:1 respectively; Loder 1996). In unilateral cases, the left hip is affected 60% of the time (Loder and Skopelja 2011). Bilateral involvement ranges from 37% to 61% (Loder, Aronson, and Greenfield 1993; Loder, Wittenberg, and DeSilva 1995).
Typical presentation of SCFE is limping with gradual onset of pain 80-86% of the time and acute or acute on chronic pain 14-20% of the time (Matava et al. 1999). Pain usually occurs in the groin but presents 15% to 50% of the time as distal thigh pain or knee pain (Matava et al. 1999). This pain is exacerbated by activity and relieved with rest. 2/3 of SCFE patients are obese. There is decreased internal rotation and abduction of the hip, as well as obligate external rotation with hip flexion. In unilateral SCFE cases, there may be a leg length discrepancy. A lateral X-ray of the hip demonstrates an anteriorly subluxed femoral neck relative to the femoral head (Gholve, Cameron, and Millis 2009). In SCFE, Klein’s line will have little to no intersection with the epiphysis (Figure 3). SCFE is classified according to the percentage of the slip: mild if the displacement is less than 30% of the width of the femoral neck, moderate if between 30%-60, and severe if over 60%. The Southwick Angle or Head-Shaft Angle also classifies the slip: mild if the angle is 0-29 degrees, moderate if 30-50 and severe if >50. A technetium bone scan may demonstrate increased uptake of the femoral physis. The most sensitive test for SCFE is an MRI, which can detect physeal abnormalities prior to slippage. On the STIR sequence marrow edema will be seen within the physeal plate.

_demonstrates_a_scfe_with_superimposed_kleins_line_(right)_sho.png)
SCFE typically occurs in adolescents during their pubertal growth spurt, but can present later in life if the epiphysis is not closed (Hu et al. 2011; Marquez, Harb, and Vilchis 2014; Macía-Villa, Sanchez-Lite, and Medina-Luezas 2016). During a growth spurt, there is decreased physeal strength secondary to increased width of the cartilage (Speer 1982). SCFE is most commonly associated with obesity, but has also been associated with local trauma, disorders of calcium (rickets, renal disease, osteodystrophy, and vitamin D deficiency), genetic disorders (Marfan’s syndrome, Downs syndrome), and endocrine disorders (hypothyroidism, hypopituitarism, hyperparathyroidism, hypogonadism, excess or deficiencies in growth hormone, and cranial tumors). Obesity and trauma increase the mechanical shear force across the physis, predisposing it to failure between the zones of hypertrophy and provisional calcification (Ogden and Southwick 1977). Disorders affecting calcium homeostasis increase bone resorption which depletes calcium available for the zone of calcification (Alghamdi, Ahmad, and Almalki 2016). If chondrocyte proliferation is greater than calcification, the epiphysis widens and weakens. Untreated SCFE he can lead to avascular necrosis, cam-type femoroacetabular impingement, and hip osteoarthritis (Zaltz, Baca, and Clohisy 2013; Wensaas et al. 2014).
Statement of Informed Consent:
We received institutional IRB exemption and have an approval through our board’s Human Subjects Research determination that the project does not meet the definitions of human subjects research and may be submitted for publication.
Case:
A 31 year old male reported to our clinic with acutely worsening chronic right hip pain with weight bearing, localized to the groin. The pain started three years after a car accident. It improved and became tolerable with the use of NSAIDS. Two weeks prior to presentation, the pain began to escalate without any inciting trauma or event. It progressively worsened with activities and he became unable to ambulate. He was antalgic and using crutches.
His past medical history was positive only for childhood chicken pox, however he had not seen a physician since adolescence. He and his parents denied any recollection of childhood hip or knee pain. He denied smoking and drank alcohol socially. On review of systems, he denied any other symptoms like excessive thirst, urination, heat/cold intolerance, weight gain/loss.
Physical exam revealed a BMI of 38. The right lower extremity demonstrated no shortening. He had groin pain with log roll of the right femur. He was unable to perform a straight leg raise due to pain. His hip range of motion was limited and painful: abduction 30 deg, adduction 20 deg, flexion 70 deg with obligate external rotation, internal rotation 0 deg, and obligate external rotation 30 deg. Examination of the contralateral hip demonstrated no pain with log roll. He could perform a straight leg raise and he had painless ROM including abduction 30 deg, adduction 20 deg, flexion 110 deg with no obligate external rotation, internal and external rotation were 15 and 30, respectively. He was neurovascularly intact.
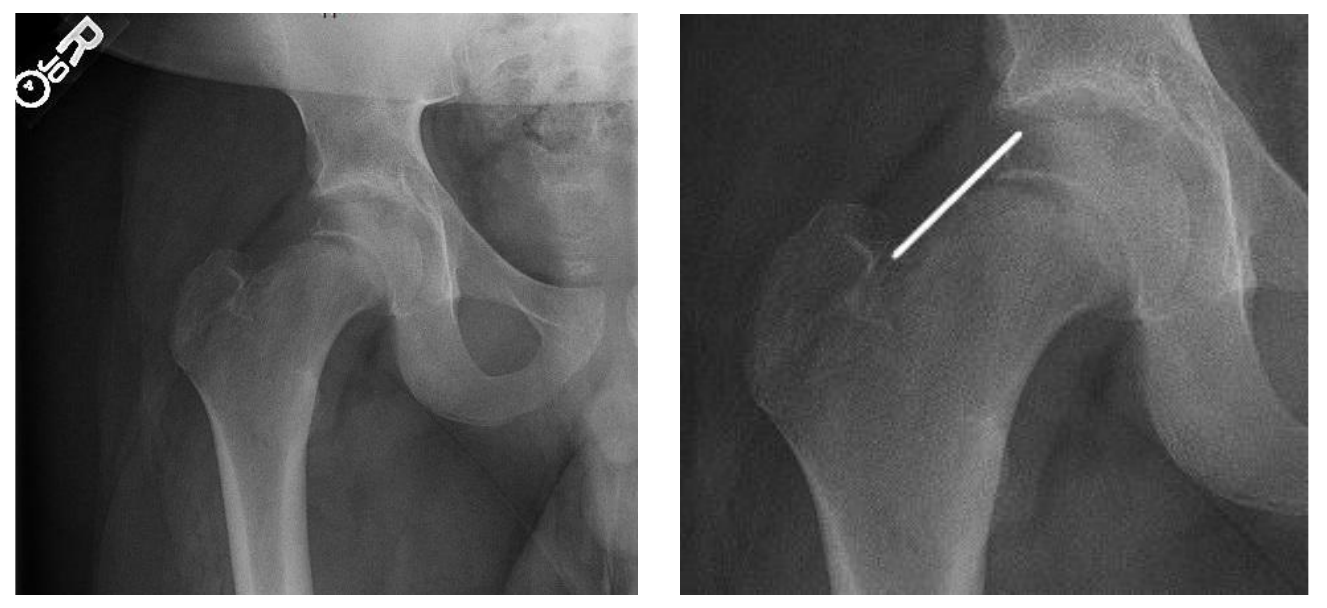
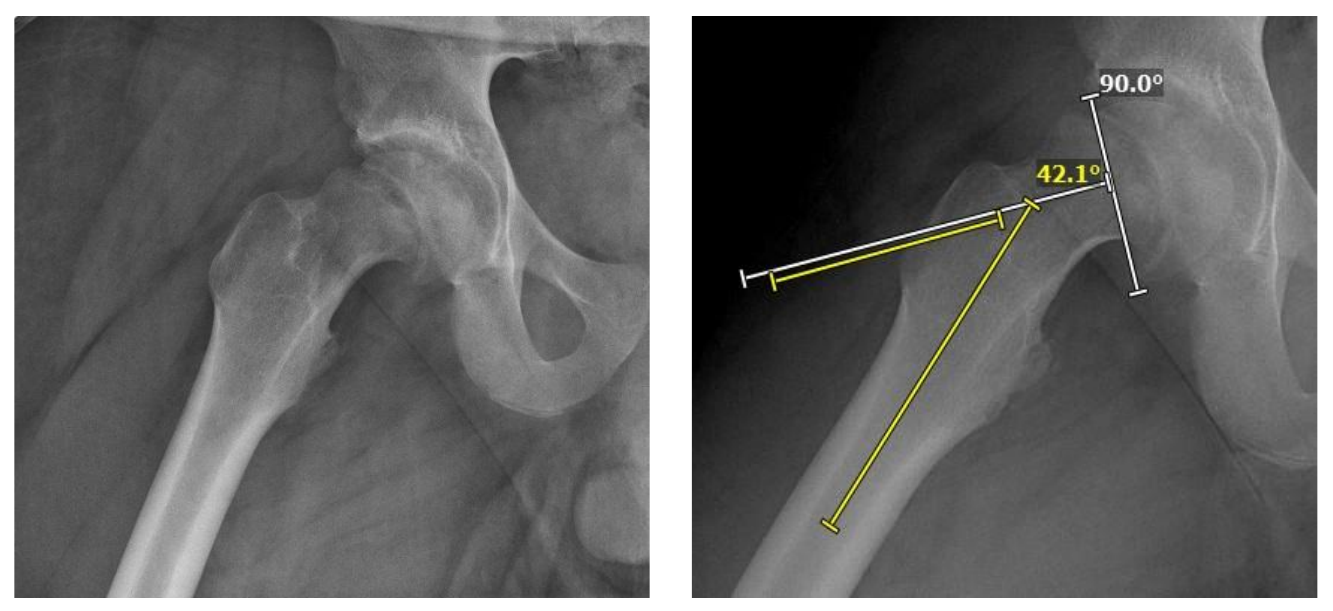
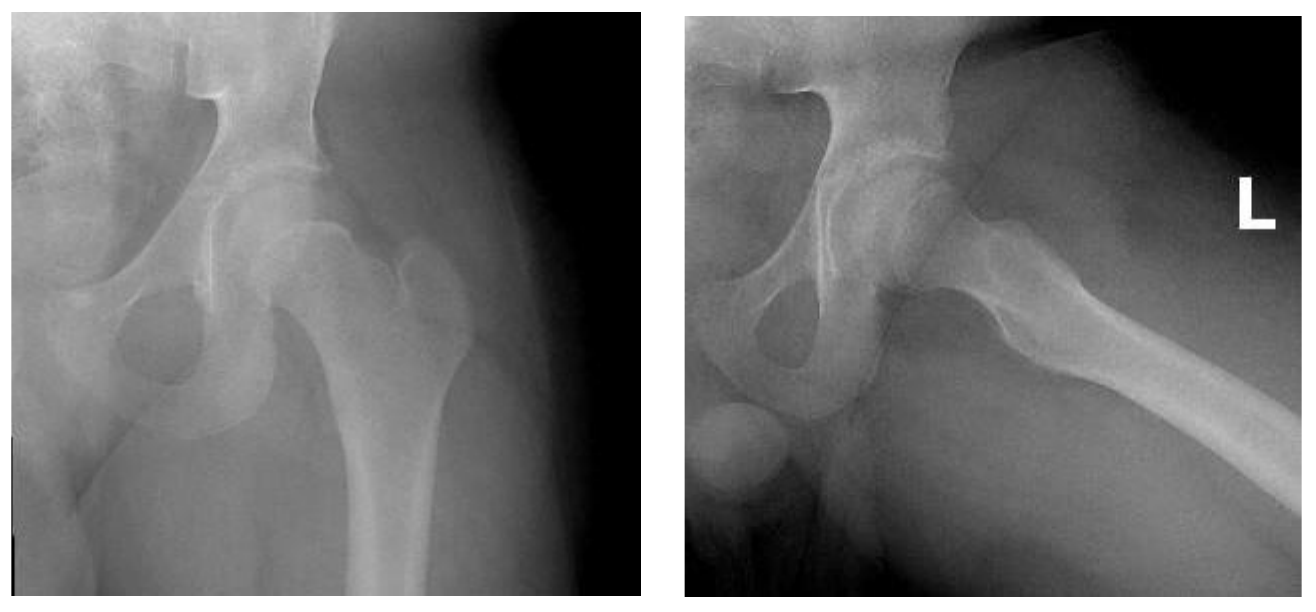
Radiographs including AP pelvis, AP and lateral (frog leg) of both hips demonstrated skeletal maturity at the stage of Risser 1 with closed triradiate cartilage and open proximal femoral physis of both hips (Figure 1). The right hip revealed a slipped capital femoral epiphysis with a disrupted Klein’s line and Southwick angle of 42.1 (Figures 2-7). Thus, due to his radiographs as well as his two weeks of inability to bear weight, he was found to have an acute-on-chronic unstable SCFE on the right.
_and_lateral_(right)_of_the_contralateral_left_hip_demonstrating_an_ope.png)
He was made non-weight bearing to the right lower extremity with crutches. We sent him for an endocrine consultation and scheduled him for surgery. He underwent percutaneous pinning in-situ of the right hip with two screws and prophylactic pinning of the left hip with one screw. Postoperatively, he was kept toe-touch weight bearing on the right side and weight bearing as tolerated on the left. At his two, six and twelve week follow ups, radiographs revealed no progression of the slip and the hardware maintained its position (Figures 8-11). He progressed to full weight bearing at 8 weeks postoperatively. At his latest follow up (1 year postoperative), his symptoms had completely resolved.
_is_a_post-operative_radiograph_demonstrating_two_partially_threade.png)
The endocrine consultation revealed no developmental delays, however he was always “short for his age.” He was noted to have a syndromic appearance with wide set eyes, low set ears, and a cognitive impairment. He also had minimal body hair, multiple patches of acanthosis nigricans as well as gynecomastia. A battery of lab work was ordered, the results of which are shown in Table 1.
A bone age radiograph of the right hand was found to be consistent with an 18 year old (Figure 12). He was diagnosed with hyperprolactinemia, hypogonadism, and hypothyroidism. He was started on levothyroxine. Thus, the cause of our patient’s delayed skeletal maturity was concluded to be hypogonadism secondary to hypothyroidism.

Discussion:
SCFE, by definition, can only occur in a patient with an open growth plate, therefore you would not expect it in an adult. The primary cause of an open physis in an adult is an endocrine disorder. In a study of adolescent patients with SCFE and endocrine disorders, 40% had hypothyroidism, 25% growth hormone (GH) deficiency, and 35% other disorders (Loder, Wittenberg, and DeSilva 1995). Hypothyroidism causes increased chondrocyte degradation, improved mineralization of the matrix, but inhibits the ossification of the mineralized matrix (Marquez, Harb, and Vilchis 2014). Hypothyroidism also delays fusion of the epiphysis, prolonging vulnerability (Feydy et al. 1997). Excess levels of GH cause proliferation and stacking of chondrocytes which increases the size of the zone of proliferation, thereby weakening the physis. In a retrospective study of patients with SCFE and a GH deficiency, 92% of SCFE cases did not occur until after starting or finishing growth hormone supplementation (Loder, Wittenberg, and DeSilva 1995). Estrogen reduces physeal width and increases physeal strength in both males and females (Witbreuk et al. 2013). In low concentrations, estrogens increase secretion of GH and IGF-1 which stimulates chondrocyte growth in the proliferation zone. In high concentrations, estrogens close the epiphysis by inhibiting clonal expansion and cell proliferation in the hypertrophic zone, inducing apoptosis of hypertrophic chondrocytes, and stimulating osteoblast invasion in the physis (Witbreuk et al. 2013). Androgens increase bone formation and growth in early puberty which can reduce physeal strength (Clarke and Khosla 2009). It is only after aromatization to estrogen in late puberty that testosterone helps close the growth plate. This may cause the increased incidence of SCFE among males vs females. In patients with hypogonadism, lower levels of sex hormones will lead to delayed physeal closure. In our case, the patient was 31 years old with an open growth plate.
We have found 7 other cases of SCFE in adults, all of them having an endocrine disorder. A summary table is shown below in Table 2. Huang et al reported a similar case of a 29 year old male who presented with SCFE associated with hypothyroidism, hypogonadism, low level of serum cortisol, but normal level of growth hormone (Huang et al. 2019). Hu et al, reported in a 29 year old man with panhypopituitarism following a craniopharyngioma excision (Hu et al. 2011). Huang and Hu came to a similar conclusion to our study that their patient’s physis were not closed secondary to hypothyroidism and hypogonadism. Marquez et al, reported in a 28 year old woman with hypothyroidism secondary to pituitary hypoplasia secondary to arachnoidocele compression (Marquez, Harb, and Vilchis 2014). Their patient did not have hypogonadism or features of sexual immaturity. Hennessey and Jones reported in a 21 year old male marine with hypothyroidism secondary to hashimotos thyroiditis (Hennessy and Jones 1982). They wrote of the association between hypothyroidism and delayed / defective epiphyseal fusion back in 1982. Marquez and Hennessey documented that hypothyroidism alone is enough to cause delayed physeal closure. Vallier et al reported SCFE in a 24 year old man with Kallmann syndrome (Vallier, Bergman, and Kargas 1994). Kallmann syndrome is a congenital form of hypogonadotropic hypogonadism associate with anosmia (Dodé and Hardelin 2009). Prolactin and thyroid hormone are usually normal. It is caused by a defect in the migration of GnRH cells which causes GnRH to not be produced correctly or released correctly. This differs from our patient as GnRH was suppressed due to low thyroid hormone causing high prolactin levels. Once thyroid hormone is administered, prolactin levels should decrease and GnRH would subsequently increase due to the presence of functional GnRH cells. These studies demonstrate that persistently open growth plates can occur with isolated hypogonadism or hypothyroidism.
Feydy et al reported in a 20 year old boy with acromegalic gigantism and hypogonadism (Feydy et al. 1997). Excessive growth hormone widened this patient’s physis and hypogonadism prevented closing of his physis. Macia-Villa et al, reported in a 47 year old woman with history of 6 years corticosteroid use and a severe vitamin D deficiency (Macía-Villa, Sanchez-Lite, and Medina-Luezas 2016).
The presentation of SCFE in an adult is an exceeding rare circumstance. While there have been other cases of SCFE in adults reported in the literature, we hope to add our experience.
Conclusion:
While SCFE is classically found in adolescents, it can be found in older patients as long as the physis is open. An open physis in adults is exceedingly rare and should immediately trigger an endocrine consultation in conjunction with surgical treatment. When endocrine disorders are discovered, careful thought should be given to prophylactically pinning the contralateral side, especially if there is question whether the patient will be compliant with monitoring for a contralateral SCFE and compliant with the endocrine treatment. The cause of our 31 year old patient’s delayed physeal closure was concluded to be the result of hypogonadism secondary to severe hypothyroidism. Due to the endocrine nature and cognitive impairment in this patient, there was a question of whether he would be compliant with his follow up. Therefore we decided to prophylactically pin his contralateral hip. The literature would have supported close follow up because none of the other 7 authors reported a contralateral slip.