INTRODUCTION
There are more than one-quarter million hip fragility fractures in the United States every year with an annual economic impact of more than 12 billion dollars (Burge et al. 2007). This injury has potentially devastating consequences in the geriatric population, with substantial impacts on patient mobility and independence, high rates of complications, and one-year mortality rates of 20-33% (Magaziner et al. 2000; Cooper 1997; Keene, Parker, and Pryor 1993; van der Westhuizen et al. 2011; Cenzer et al. 2016; Mears and Kates 2015). The successful treatment of these injuries revolves around several aspects of care that have been shown to be beneficial to outcomes in this population, including inpatient co-management by a geriatrics service; expedited time to surgery; a standardized post-operative mobility protocol; and a carefully scrutinized medication regimen with respect to elderly patients (Ftouh et al. 2011; Bernstein et al. 2014; Potter, George, and Guideline Development Group 2006). A recent retrospective observational study demonstrated a direct correlation between a surgical delay of more than 12 hours and the increased adjusted risk of 30-day mortality (Nyholm et al. 2015). Additionally, it demonstrated a surgical delay of more than 24 hours significantly increased the adjusted risk of 90-day mortality (Nyholm et al. 2015).
Today, evidence-based medicine is a common theme amongst most physicians and health systems as a means to implement practices that can improve the quality and decrease the cost of care. Recently, an operations management strategy known as Lean Six Sigma (LSS) has been used in health care to improve the organization and quality of care and reduce cost (Langabeer et al. 2009; De Mast 2007). LSS is a combination of Lean Synchronization, which allows for speed and elimination of waste, and Six Sigma, which seeks less variability in the results of the process. Together, this methodology seeks to improve quality, reliability, flexibility, delivery, and efficiency of processes (Brandao de Souza 2009; Kumar and Thomas 2010). LSS includes the DMAIC improvement cycle as part of the quality improvement process. This is a data-driven quality strategy with phases that offer a roadmap as an improvement methodology and a conceptual framework to improve processes (Asq.org 2017). The phases consist of Define, Measure, Analyze, Improve, and Control. In this study, LSS and the DMAIC improvement cycle will be used as a framework to map the process of a quality improvement initiative designed to enhance care delivery to geriatric hip fracture patients.
This initiative, named the Geriatric Hip Fracture Program, consisted of a multi-disciplinary disease team and adopted several aspects of treatment that have been shown to be beneficial to outcomes in the population. This study will show a correlation between this process improvement to Lean Six Sigma, which ultimately resulted in significant improvements in the care of our geriatric hip fracture patients.
METHODS
A critical analysis of the operational characteristics behind the care of patients sustaining geriatric hip fractures was performed using an operational management approach. Included patients were admitted to a single Level 1 Trauma Center through the emergency department (ED), trauma bay, or transfer from an outside facility for care of an acute hip fracture. With geriatric hip fractures accounting for just over 10% of the orthopaedic surgical volume experienced by our institution, a careful analysis of this patient population and strategic changes to their management, realized through the DMAIC improvement cycle, could be highly impactful.
Define
The Define phase of the DMAIC roadmap focuses on defining the problem to be solved (Niemeijer et al. 2013). Based on the literature and best practices, the two major benchmarks that hospitals are compared to when treating geriatric hip fractures are time to surgery and length of stay (LOS). The International Geriatric Fracture Society (IGFS), was used as a benchmark as compared to the United States IFGS average. The data for our institution from FY’15 demonstrated as compared to the IFGS average an average time to surgery 3.6 hours shorter; an average length of stay 0.7 days longer; a 30-day re-admission rate 0.21% lower; and an in-hospital mortality rate 0.31% lower (Table 1). The goal of the program was to be better than the IFGS average on all metrics with a focus on the average time to surgery and LOS. More specifically, with evidence demonstrating significant increased mortality after 24 hours, the goal was to have an average time to surgery at or below this (Nyholm et al. 2015) and an average LOS of 4 days.
Measure
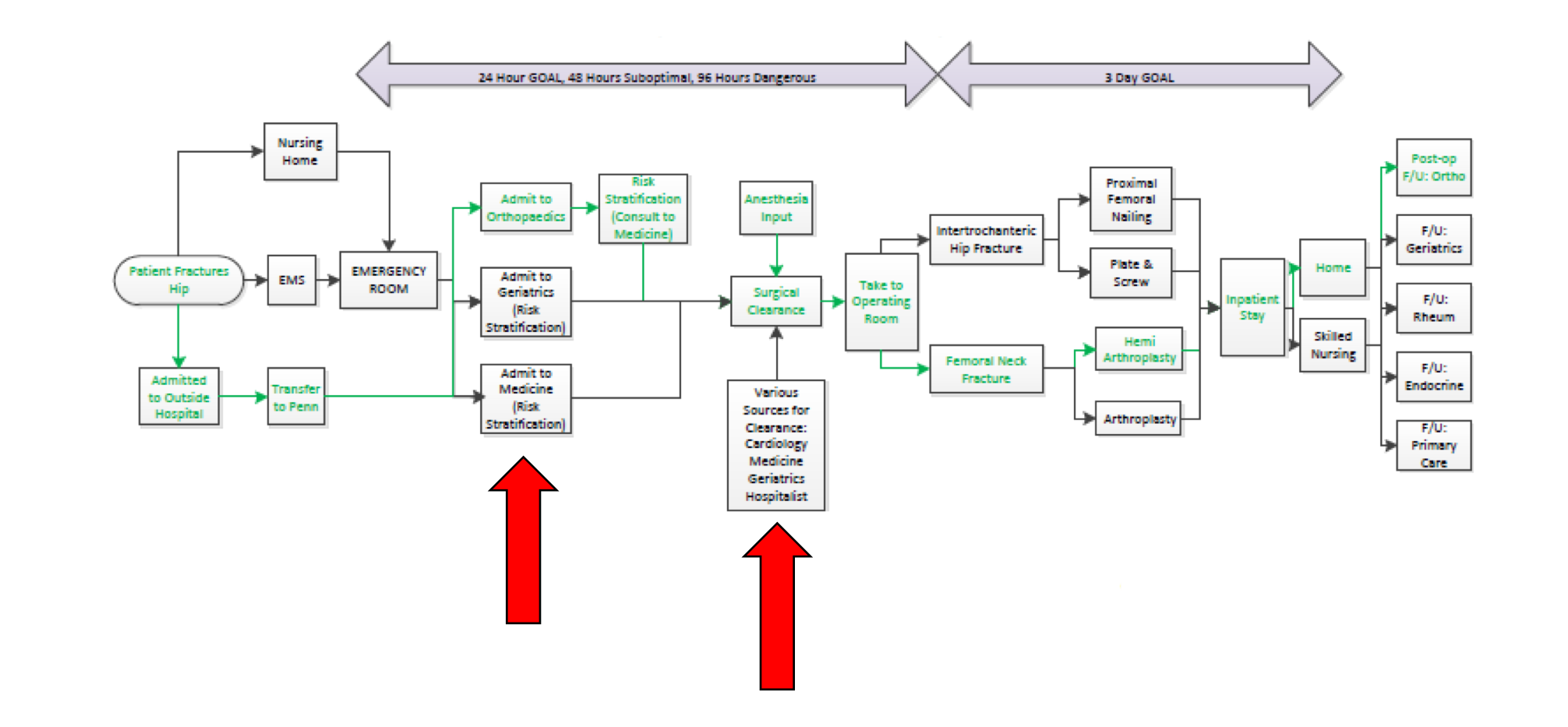
The Measure phase of DMAIC roadmap is concerned with quantifying the current process performance. After identifying in the define phase that our institution was over 24 hours for average time to surgery and that the average LOS was over the IFGS average at 7.1 days, the process was mapped to help identify potential bottlenecks throughout the system that would be delaying our time to surgery and LOS (Figure 1).
As depicted by the process map, the transformed resource in the process was the “patient fractures hip” and is affected by many factors (Slack, Johnston, and Brandon-Jones 2011). When drawing out the process, it was clear that the geriatric hip fracture patient had multiple pathways into our system and multiple pathways through our system. Understanding the goals of decreasing our time to surgery and length of stay, the process map was subdivided into two phases (Figure 1), which framed the groundwork for analyzing the process.

Analyze
The aim of the Analyze phase is to arrive at a data based diagnosis of the current process performance (Niemeijer et al. 2013). Focusing on our two main goals, there were two major areas of bottlenecks that lead to significant delays in time to surgery and LOS (Figure 1). The first major finding was that time to surgery and LOS were directly related to the service that the patients were admitted to. Patients with hip fractures that were not admitted to the Orthopaedic Trauma service had roughly a 4-hour longer delay to surgery (19.37 hours versus 15.88 hours) and 3.86-day longer LOS (8.43 days versus 4.57 days) when compared to those admitted to the Orthopaedic Trauma Service. The other major finding was that time to surgery and LOS were directly related to whether additional perioperative tests beyond routine testing, which included basic laboratory tests, chest x-ray, EKG, and urinalysis, were ordered. Additional perioperative tests were considered to be any test in additional to routine testing including transthoracic echocardiogram, cardiac stress test, carotid ultrasound, rule-out myocardial infarction, electroencephalogram, implantable cardioverter-defibrillator interrogation, and endoscopy. Patients with hip fractures that underwent additional perioperative testing had roughly a 36-hour longer delay to surgery (73.33 hours versus 37.33 hours) and a 3-day longer LOS (12.01 days versus 9.01 days) as compared to those that did not undergo this additional testing.
Improve
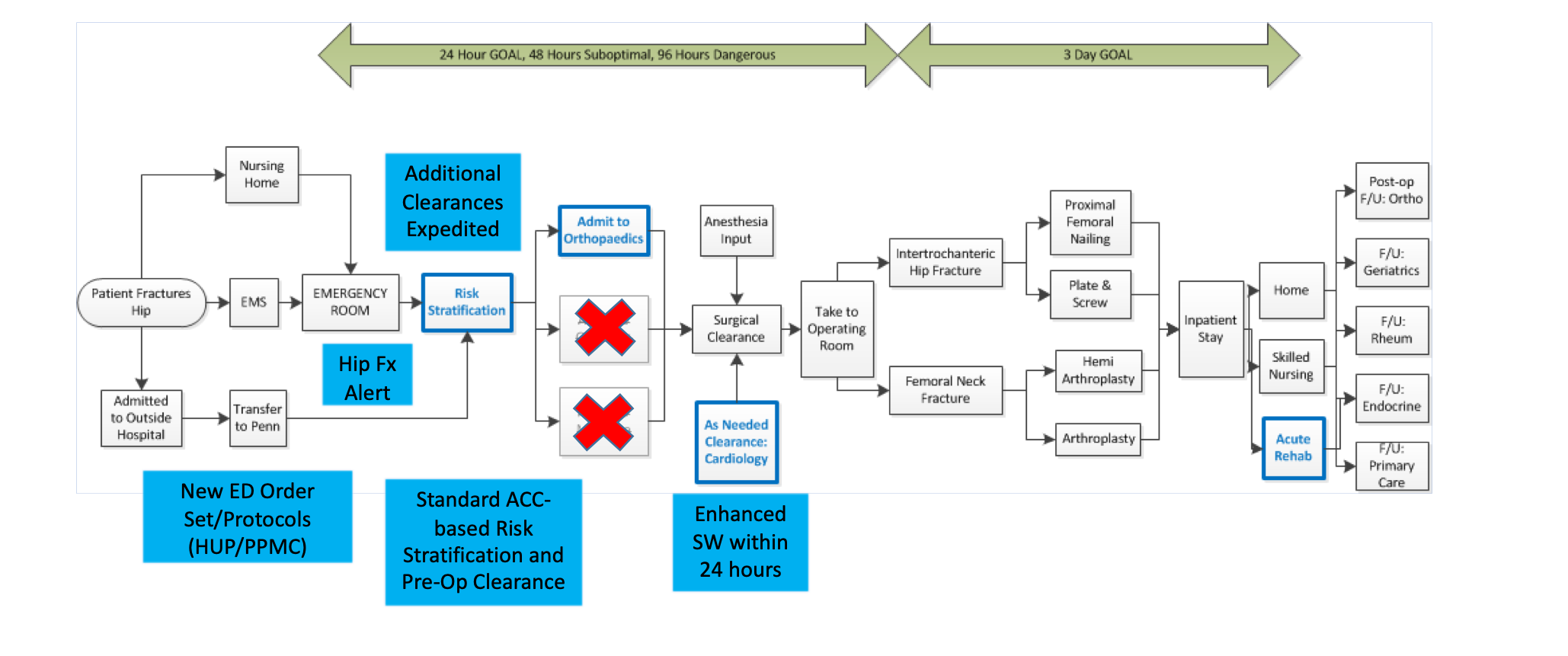
After the process was diagnosed, our Geriatric Hip Fracture Program was implemented in the Improve phase. This was designed as a clinical care program for patients over the age of 60 to provide quick surgical fracture treatment, collaboration of services and specialties, minimize complications, create clear and consistent treatment standards, inform and educate patients and families, control cost, prepare for healthcare reform changes, and to improve patient experience, satisfaction, and continuity of care. With this, the hip fracture disease team was developed including members from Orthopaedic Surgery, Geriatrics, Hospitalists, Anesthesia, Physical Therapy, Pharmacy, Hospital Administration, Nursing, Physical Medicine and Rehabilitation, Infectious Disease, Emergency Medicine, IT, social work, quality improvement, and research. This disease team evaluated the data and implemented a number of processes to help improve the throughput. The first included an “ED Order Set”, which is a pre-populated order set integrated into the electronic medical record that is initiated by the Emergency Room physician in the setting of a triage complaint of concern for a hip fracture or a patient greater than 60 years old or from a skilled nursing home with a history of fall, hip pain, and inability to bear weight. This order set included all routine preoperative studies and orders, fragility labs, and radiographic imaging. Importantly, the order set also contained a “Hip Fracture Notification Alert” that sent a text alert to all care providers and team members that would or could be involved in the patient’s care. This addition ensured that the medical evaluation of these patients was initiated overnight in order to minimize unnecessary delays to the operating room.
Utilizing the data that demonstrated that patients not admitted to the Orthopaedic Trauma service had greater delays to surgery and longer LOS, default admission of these patients to the Orthopaedic Trauma service was implemented. This would allow the treatment teams to maintain focus on the injury and level of necessary rehabilitation, to provide nursing staff and therapists skilled at managing lower extremity trauma, and to maintain a sense of ownership of these patients by the treating surgeons.
Lastly, utilizing the data that demonstrated greater delays to surgery and longer LOS for those patients that underwent additional preoperative testing, clear guidelines were developed for pre-operative risk stratification for these patients. This was used to balance medical optimization and expedient surgery while utilizing established ACC/AHA guidelines to minimize variability in determining clinical risk and reduce unnecessary testing (American College of Cardiology 2017). The “Risk Stratification Guidelines” were provided to all hospitalists and geriatricians in a one-page document clearly stating the goal of surgical stabilization in less than 24-hours and to manage acute medically modifiable risks that could be mitigated within a short window. These initial quality improvements were implemented and a modified process map was produced to depict the ideal patient flow (Figure 2).

Control
This new process is actively monitored to assure that these improvements are producing better results and that these results are retained. The hip fracture design team meets monthly to review and analyze the data. These meetings attempt to identify trends that might indicate the process becoming out of control. Additionally, the outliers that are identified with respect to time to surgery or LOS are further investigated to uncover any pathway deviation or reason for this aberration.
RESULTS
With implementation of these quality improvements in the Improve phase of DMAIC, it was observed over FY’16 that the average time to surgery decreased from 32.4 hours to 17.5 hours. Additionally, average length of stay decreased from 7.1 days to 5.6 days. Additional observations included a decrease in 30-day re-admission rates from 14.29% to 8.33%, a decrease in in-hospital mortality from 2.79% to 0%. Lastly, the process could identify that 100% of the patients were co-managed with either the Internal Medicine or Geriatric service (Table 1).
When utilizing the Lean Six Sigma process, it is important to realize that this is a continuous improvement philosophy. The last point of the DMAIC cycle, which is argued by some to be the most important, is that the cycle starts again at the Define phase (Slack, Johnston, and Brandon-Jones 2011). This philosophy accepts that the cycle never stops and that improvement becomes a part of the culture.
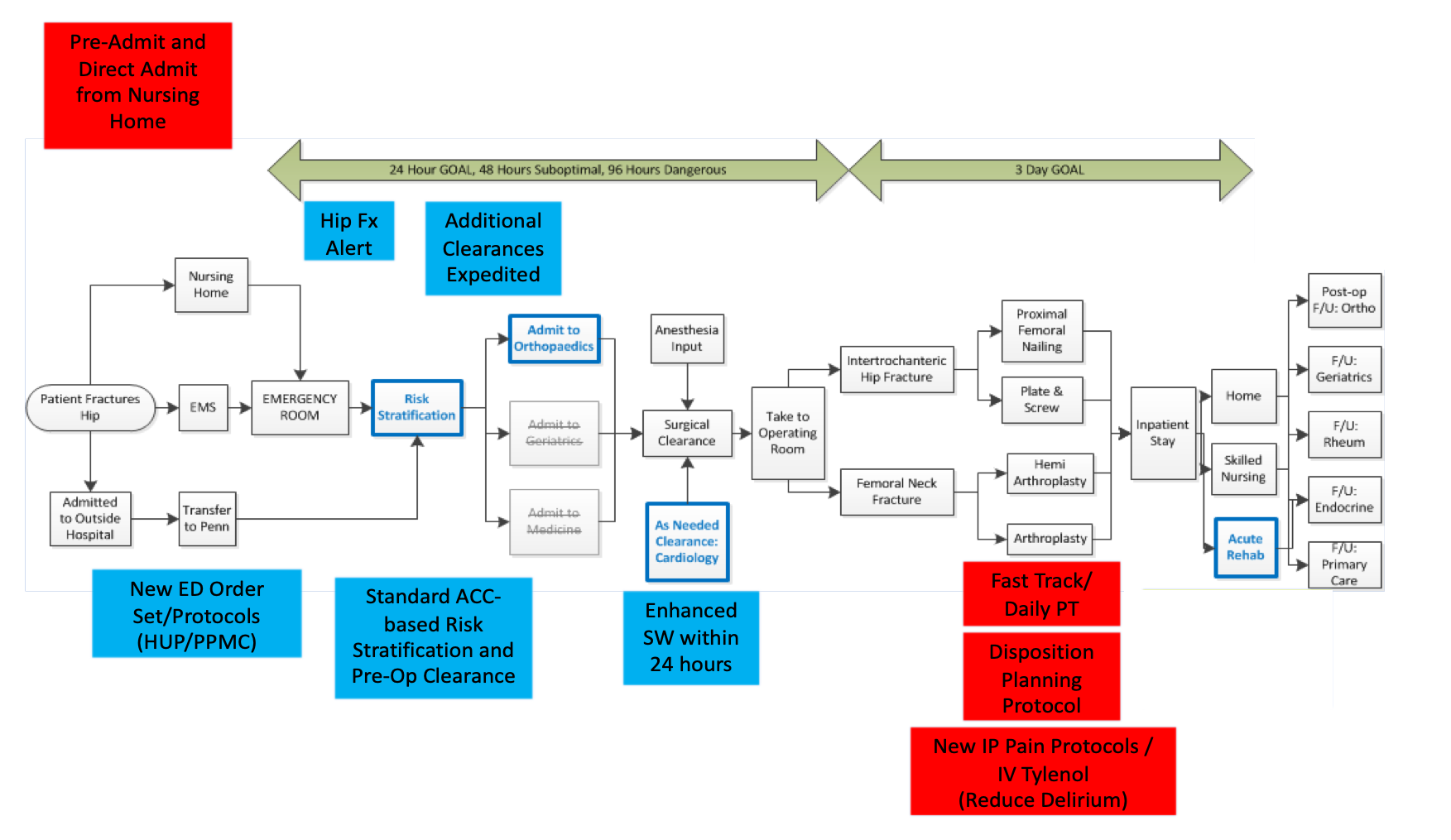
The Geriatric Hip Fracture Pathway was developed to be a continuous quality improvement cycle and throughout this process, additional areas of improvement were identified by the monthly disease team meetings. The first was in the inpatient post-operative care management. Early data demonstrated that patients who underwent surgery between Wednesday and Friday had a significantly longer length of stay than those operated on between Saturday and Tuesday. In response to this, post-surgical orders included that all patients be weight-bearing as tolerated on the operative lower extremity and that geriatric hip fracture cases be prioritized to be completed before noon in order to have physical therapy evaluate the patient the same day of surgery. Following this evaluation, an early mobilization protocol including weekend physical therapy sessions was initiated to help patients reach a safe disposition more rapidly. Additionally, early involvement and intervention by a social worker to commence disposition planning earlier would avoid any unnecessary delays on discharge. Ultimately, these data driven interventions resulted in shorter lengths of stay for our hip fracture patients.
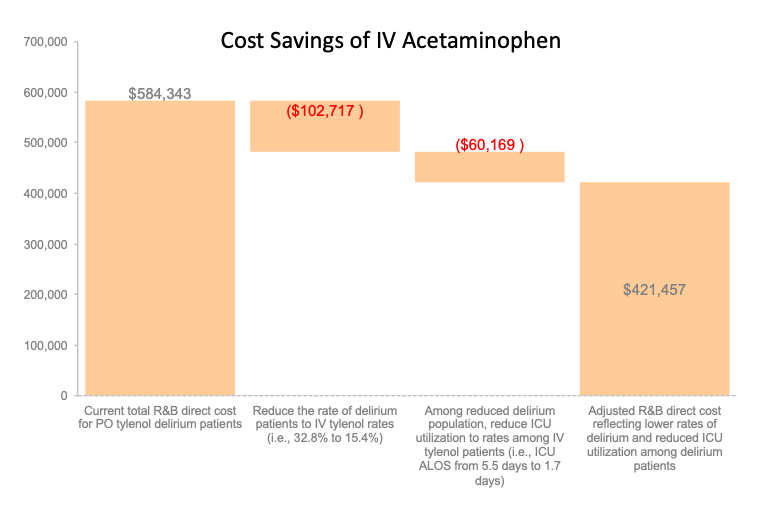
The second area of improvement was initiated to decrease post-operative delirium by adding IV acetaminophen as a part of the post-operative pain protocol. Post-operative delirium in the hip fracture population has an incidence of 16-70% (Schuurmans et al. 2003). Delirium has been identified to increase length of stay, cause worse functional outcomes, and independently increase mortality (Marcantonio et al. 2000). The process was analyzed and demonstrated that the patients that received IV acetaminophen developed delirium 15.4% of the time compared to 32.8% in those who received acetaminophen orally. This demonstrated that converting oral acetaminophen patients to IV acetaminophen would reduce the rate of delirium in hip fracture patients and reduce ICU utilization, resulting in $160,000 cost savings for the health system (Figure 3).

The third area of improvement focused on facilitating the care of patients from skilled nursing facilities with a concern for a hip fracture. The goal was to implement a system that would allow this at-risk patient population to bypass the emergency room and be admitted directly to the hospital floor to enhance the throughput of the patient through the system. With selected skilled nursing facilities, the “direct admissions” quality improvement process was implemented and the first patient directly admitted from a nursing home occurred in May 2017 and was successfully treated and discharged within 3 days after the admission. The process map was revised to incorporate these areas for improvement identified by monthly disease team meetings (Figure 4).

By using this system of continuous improvement, the process has seen progressive gains. Since its implementation, the reductions seen in time to the operating room have been maintained. Patient length of stay and 30-day readmission rates have continued to downtrend with consistent critical evaluation of the pathway (Table 1). These continued successes further highlight the effectiveness of this methodological approach to optimizing care pathways.
DISCUSSION
This study was used to demonstrate the usefulness of an operational management approach to a clinical care pathway for geriatric hip fractures. Utilization of an operational improvement methodology employs a systems-thinking mindset to improving the process. Multiple approaches to improvement have been described, however, recently, in the health care industry the combination of Lean Synchronization and Six Sigma in the form of Lean Six Sigma (LSS) has been utilized as a methodology. LSS can be used as a tool for improving efficiency in providing care to patients with specific disease processes. An additional value of LSS is the combination of the use of a structured DMAIC roadmap to provide a conceptual organizational framework (Niemeijer et al. 2013).
Our Geriatric Hip Fracture Pathway was analyzed via LSS and patient care was improved across multiple domains, which supports the importance of using a systematic approach to process improvement. Identifying the two main benchmarks of average time to surgery and LOS allowed for clear goals to be established. Utilizing the International Geriatric Fracture Society national averages and institutional data allowed for both an external and internal benchmark to compare performances and evaluate the success of the system (Slack, Johnston, and Brandon-Jones 2011). Important to any operational understanding, the development of the geriatric hip fracture process map allowed for the entire process to be mapped out to understand the influence of all the transforming resources. As evidenced by the process map, the geriatric hip fracture patient flowed through an incredibly complex process with many inefficiencies. Utilizing data analysis, two main bottlenecks were able to be identified causing significant delays in time to surgery and increased LOS. These were being admitted to a non-orthopaedic service and having additional perioperative tests ordered. Once these were identified, improvement processes were put in place to facilitate eliminating this waste and improving the efficiency of the process. These improvement processes included a clear admission pathway to the Orthopaedic service and a detailed guide to perioperative medical optimization among other additional flow improvements. With these improvement processes in place, the system realized a significant improvement in the average time to surgery with a decrease from 32.4 hours to 17.5 hours and in the average length of stay with a decrease from 7.1 days to 5.6 days amongst other things.
The system faces many challenges. Most of these challenges in the early phases have been due to the human involvement factor. Humans inevitably create inefficiencies. Early success in overcoming these challenges has focused on education and buy-in to create a sense of pride and ownership. Identifying champions within each subset of the disease team has fostered the environment and enhanced the communication amongst the bigger group. Having a clear stated vision, forming a guiding coalition, and having early wins has started to ingrain this process into the culture and has given everyone a shared purpose.

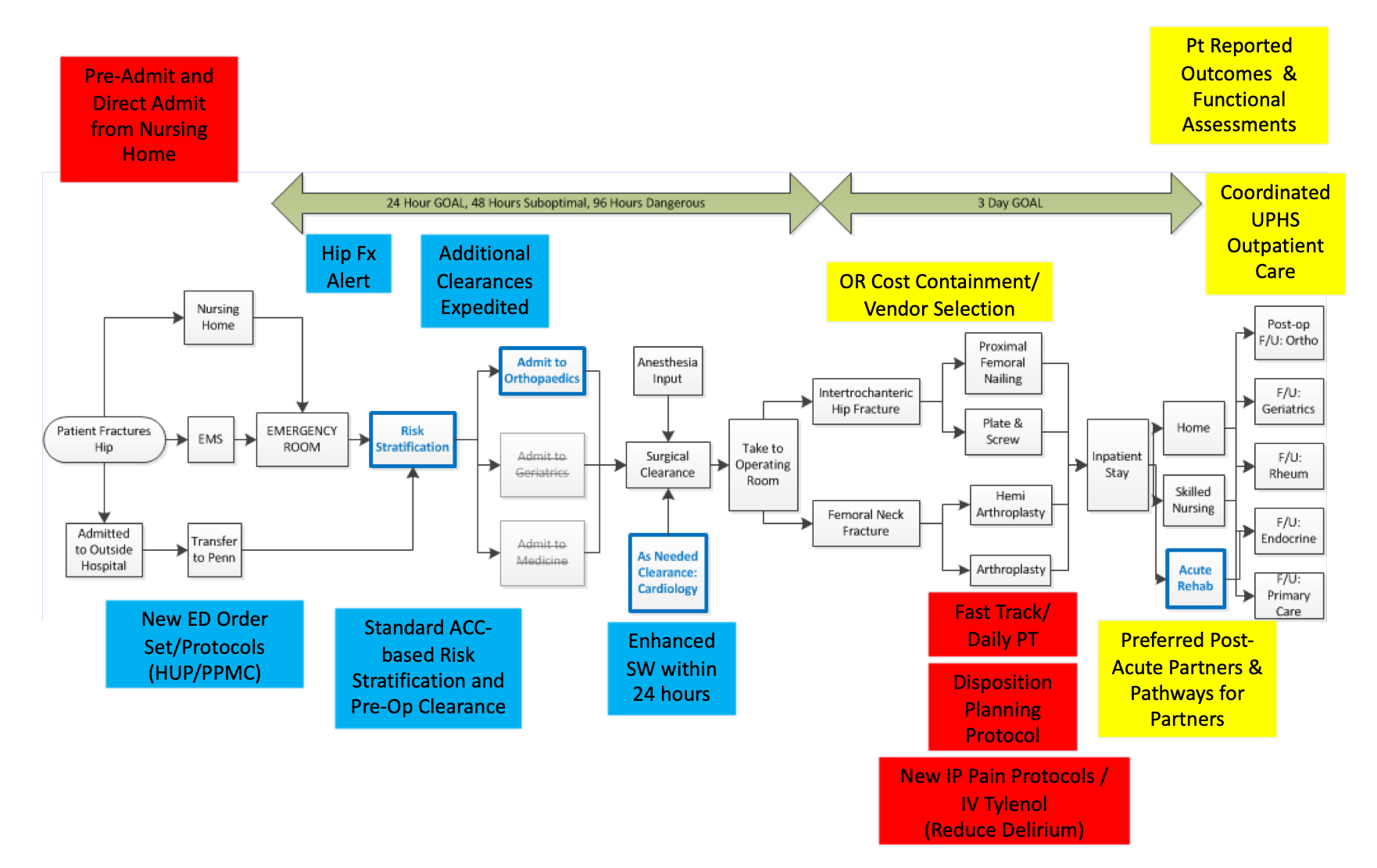
As with any good improvement cycle, the critical phase is the cycle starting again. With a clear control mechanism in place, the repetition of the cycle allowed for more problems and areas of improvement to be defined. In addition to the quality improvement processes that were initiated through the Control phase, other areas for improvement have been identified that will be the focus of future quality improvement projects. First, operating room cost containment and careful vendor selection will reduce the cost of the implants placed in patients based on best practices for fracture pattern, age, preoperative physical status, and medical co-morbidity indices, and ultimately will allow better control over the cost of care in the future. Second, preferred post-acute care partners and pathways for partners to align the inpatient process with post-acute hospitalization rehabilitation centers and skilled nursing facilities were identified in order to increase the quality and drive down the cost of post-acute care. Lastly, the coordination of outpatient care with multiple medical services and patient reported outcomes will be a significant focus in the future to improve the overall quality of care of the hip fracture patients. This has led to the conceptualization of an ideal state pathway which will allow for continued gains in the care of our patients (Figure 5).
The initial success of this pathway proved to be critical for the continued support by the health system and led to a redefined operation strategy which influenced the strategic decisions of the Department of Orthopaedics. This redefined operations strategy has provided insight and guidance throughout other core functions within the organization. Specifically, this strategy has made our institution a regional leader in the management of geriatric hip fractures and has allowed us to guide our affiliate hospitals in optimizing the care of these patients. Our impact on the community has also been furthered by developing relationships with the local nursing and rehabilitation facilities that manage these patients after discharge. Lastly, the care of hip fracture patients has undoubtedly been enhanced through this systems-thinking initiative and will continue to be improved allowing their care to be optimized to mitigate risks and minimize complications so they can continue to age gracefully and enjoy their golden years a little longer.