
1. Introduction
This year, the Coronavirus Disease 2019 (COVID-19) pandemic has caused orthopaedic departments across the world to postpone or cancel substantial numbers of elective surgery, including total knee arthroplasty (TKA) procedures (Athey et al. 2020; Sarac et al. 2020; Thaler et al. 2020). The financial implications of these cancellations on healthcare providers could be catastrophic, particularly in countries like the United States where revenues from elective procedures like TKA are heavily relied upon (Athey et al. 2020; Anoushiravani et al. 2020; O’Connor et al. 2020). As restrictions ease and elective procedures resume, many orthopaedic departments will be placed under pressure to perform a higher volume of procedures than usual to recoup recent financial losses and more importantly, address the growing waiting lists and patient demand (Athey et al. 2020; O’Connor et al. 2020).
In light of the COVID-19 pandemic, operating room (OR) protocols are likely to change. There will be longer turnover times between surgical procedures to allow more thorough cleaning of the OR between cases and changes to anaesthetic practice (de Caro, Hirschmann, and Verdonk 2020). Furthermore, to allow clearance of aerosols, ORs that undergo the minimum recommended 12 air changes per hour may have to be left empty for a further 23-35 minutes after each case (Public Health England 2020; Centres for Disease Control and Prevention 2003). This length of time could be reduced by increasing the ventilation rate. Nevertheless, offsetting this time by improving OR efficiency will become increasingly desirable meet demand. Failure to adapt to these changes may result in fewer cases being completed each day and further cancellations.
A growing body of evidence supports the use of patient-specific instrumentation (PSI) to improve OR efficiency in TKA (Attard et al. 2019). PSI eliminate the need for some intra-operative steps which are necessary with conventional instrumentation, thus reducing the overall length of the operative procedure (Attard et al. 2019).
Our previous research has shown that procedures that combined PSI with disposable or single-use instrumentation (SUI) saved time in the OR when compared to procedures that were carried out with conventional reusable instrumentation (Attard et al. 2019). SUI also have the advantage of not needing to be sterilised after the surgery for re-use. As a response to the pandemic, the use of disposable medical devices may become preferable in the OR for infection control, and to cut costs on the sterilisation of instruments post-operatively (Awad et al. 2020). SUI are therefore expected to become more commonplace in the orthopaedic OR.
This article presents a protocol for TKA with PSI and SUI. This protocol has been used by the authors in private hospitals and public teaching hospitals and is therefore applicable to multiple hospital environments.
2. Protocol
This is a protocol for implanting the GMK Sphere TKA with MyKnee Efficiency PSI and GMK Efficiency SUI (Medacta International S.A., Switzerland). These instruments and the corresponding implant can be purchased as a bespoke package (Efficiency Knee Pack) specifically for the individual patient.
MyKnee Efficiency PSI are cutting-blocks that use the anatomy of the patient’s knee to allow the surgeon to create accurate intra-operative bone resections. They are created from images of the pre-operative leg captured with Computer Tomography (CT) or Magnetic Resonance Imaging (MRI). The imaging technique employed is at the discretion of the orthopaedic surgeon. Approximately 96% of procedures are performed from a brief scanning CT scan of the hip, knee and ankle, which carries less radiation exposure than standard diagnostic CT scanning. Surgeons wishing to use MyKnee PSI with their patients must register their radiology department with Medacta International before any bespoke procedures can be carried out.
2.1 Patient Selection
Any patient who is deemed eligible for TKA following radiographic and clinical assessments of the knee by a consultant orthopaedic surgeon may receive the GMK Sphere using PSI and SUI. The eligibility criteria for this particular procedure therefore does not differ from conventional TKA. However, surgeons should note that the MyKnee PSI are made from Polyamide PA12, thus an allergy to this material would contradict the patient to this type of surgery.
As the patient pathway for TKA with PSI involves an additional scan of the pre-operative leg, surgeons must check their patient’s medical history for contraindications for their chosen imaging method (CT/MRI). The need for this additional scan, and the risks involved, must be communicated to patients before consenting them for the procedure.
2.2 Pre-Operative
Imaging
-
Surgeon or surgical scheduler creates a new case for the patient in a secure web portal and specifies here that the case will be carried out with PSI, with or without SUI.
-
Radiology technician carries out CT/MRI of the knee, which is uploaded to an official web portal.
-
Patient attends all routine pre-admission checks.
Official protocols for the CT and MRI scans should be followed by a technician to ensure that the images are of optimal quality for the generation of the bespoke cutting-blocks. Table 1 outlines the key aspects of these protocols.
CT and MRI scans should ideally be completed 4 weeks before surgery to ensure that any specific requirements of the case can be discussed between the surgeon and their dedicated biomedical engineer prior to manufacture of the bespoke blocks. Images older than 7 months will be rejected, as they may no longer truly represent the morphology of the knee at the time of surgery.
Surgical Planning
-
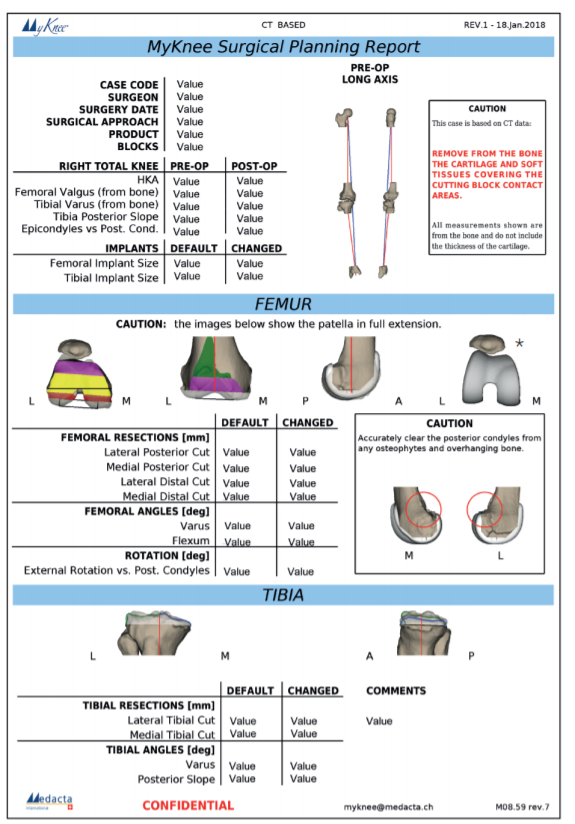
A pre-operative plan from the uploaded images is co-created by the surgeon and engineers in the web portal (Figure 1). Any specific surgical preferences the surgeon may have (such as preferred approach) can be included here to be incorporated into the plan.
-
Surgeon validates or changes the following parameters in the web portal: Femoral implant size, tibial implant size, femoral resections, femoral angles, femoral rotation, tibial resection, tibial angles.
-
Surgeon confirms pre-operative plan.
-
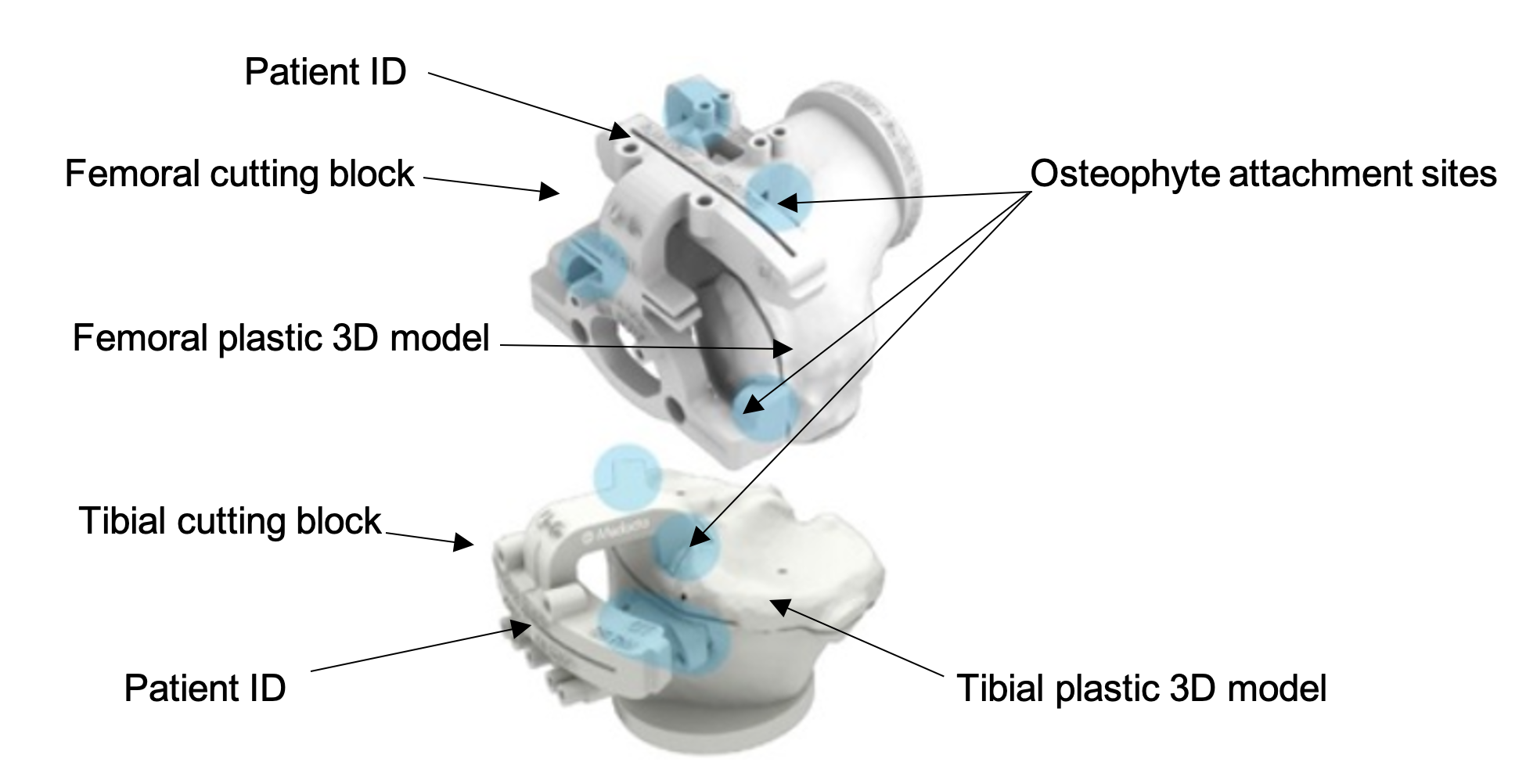
A 3D-printed life-size replica copy of the patient’s knee is manufactured (Figure 2) and the MyKnee PSI cutting blocks, as per the finalised pre-operative plan.
-
MyKnee PSI and GMK Efficiency SUI are delivered to the surgeon’s hospital.
.png)
.png)
2.3 Intra-Operatively
Specific Trays Required in OR
-
1 x General Efficiency Instrument tray
-
1 x Efficiency Femoral tray
-
1 x Efficiency Insert tray
-
1 x MyKnee PSI tray
The sizes of some of the instruments provided in the trays are bespoke to the case and are based on the pre-operative plan (Figure 3).
Implant Specifications
-
1 x GMK Sphere femoral component
-
1 x GMK Sphere tibial component
The sizes of components provided are bespoke to the case and are based on the pre-operative plan.
Backup Material Required in OR Set-up Room
- 1 x Backup tray of GMK Efficiency SUI
__femoral_(middle)__and_instrument_(right)_trays.jpeg)
Other Equipment
The instruments described above only include those required to implant the device. All other OR equipment and materials routinely needed to execute a TKA (e.g. bone cement, scalpels, sutures etc.) must also be prepared for use.
Surgical Procedure
-
OR staff prepare the OR with all essential instruments and equipment.
-
Anaesthetist and surgeon prepare patient for surgery as per routine for TKA.
-
Scrub nurse opens General Efficiency Instrument tray and MyKnee PSI tray. The blocks are double checked for the patient identification (Figure 2).
-
Surgeon begins procedure via their preferred approach.
-
The soft tissues are debrided from the bony points of contact with the blocks, and bone cuts made directly through the blocks. Of note, the blocks are full cutting blocks not merely pin-placers (Figure 2). Gap balancing and ligament tension can be assessed by SUI that attach to the blocks.
-
Trial implants are used as normal. These are provided in the pack sized same, up and down from the surgical planning, so a full range of trial implants does not need to be opened for each case. The trial implants are also disposable.
Closure
- Surgeon implants GMK Sphere and closes as per usual protocols for TKA.
OR Turnover
-
When the surgeon has completed the surgery and closed the wound, OR staff dispose of the efficiency trays and contents directly into the theatre waste bags. No clean-down is required for the disposable instruments and jigs. The only reusable tray requiring processing/sterilisation is the basic tray.
-
OR prepared for next case.
2.4 Efficiency
Surgery
PSI have been reported to lead to improved OR efficiency, by eliminating steps that are usually required for standard instrument procedures. According to our previous research* statistically significant improvements in time were recorded during set-up and clean-up times of TKA with PSI (Attard et al. 2019). Differences between procedure times (defined as knife-to-skin to closure with last clip) almost reached significance (p = 0.054). The average procedure time for PSI TKA with standard reusable instruments was 58 minutes 10 seconds. Little difference was observed when SUI were combined with the PSI (58 minutes 48 seconds). On average, these procedures were 5-6 minutes faster than those carried out with conventional instrumentation. This was also true for the total instrument time, which was defined as the time between the scrub nurse opening the first tray and returning the final tray to the sluice room for cleaning. An OR that is performing 4 TKAs a day could therefore save almost the same time as a joint replacement. This time saving, combined with an increased OR ventilation rate, could prevent the OR daily capacity from being reduced by one case post-pandemic (Table 2).
Turnover Time
MyKnee PSI and GMK Efficiency SUI can be delivered pre-sterilised, removing the need for the hospital to clean and sterilise the instrumentation before use. This may have a significant impact on turnover time between cases. Our previous research has showed that sterilisation times of TKA trays can be very variable (Attard et al. 2019). The late arrival of trays was shown to delay the start of some procedures (Attard et al. 2019). Intra-operative delays were also reported due to missing instruments following sterilisation (Attard et al. 2019). Such delays could potentially lead to later cases being postponed, particularly if sterilisation occurs at an external site. Opting to receive pre-sterilised instrumentation may save precious time between cases as well as during the procedure itself. These minutes are particularly important in a time when the average turnover time is likely to be increased to allow for deeper cleaning of the OR.
Further benefits of using SUI include post-operative cost savings, due to the need to sterilise fewer trays after surgery. According to our previous research in 2014, the cost of sterilising trays of reusable instrumentation for TKA with MyKnee PSI was £327.73 (~$400), or £424.12 (~$550) for sterilising reusable instrumentation for conventional TKA. These costs could be saved with the use of SUI.
The need for fewer trays also benefits OR staff wellbeing. Trays of conventional reusable instruments have been reported to total over 30kg (Attard et al. 2019). When using SUI however, the weight is no greater than 5kg (Attard et al. 2019). In terms of OR efficiency, fewer and lighter trays mean that the time it takes for the member of staff to move the trays in and out of the OR is reduced. It also means the task can be delegated to a single member of staff, leaving other staff free to continue working on other tasks. This seemingly unimportant variable could therefore save time between cases.
Inpatient Stay
Our previous research has shown that patients who underwent TKA with PSI were discharged from hospital one day earlier than those who underwent conventional TKA (Attard et al. 2019). Surgery with PSI is also a quicker procedure that avoids instrumentation of the medullary canal with alignment guide rods. This has been associated with lower blood loss. Our previous research estimated that patients who underwent PSI TKA lost 785.2ml of blood when reusable instruments were used and 812.0ml when SUI were used. Both groups experienced less blood loss than those who underwent conventional TKA (898.9ml when reusable instruments were used vs 936.8ml when SUI were used) (Attard et al. 2019). Actual blood loss was estimated from pre- and post-operative haematocrit levels and patient weight in kilograms using a formula (Attard et al. 2019; Gross 1983). None of the patients required transfusion.
Although inpatient stay does not impact OR efficiency, it is a significant cost saving, and allows for greater patient turnover within the department. This lowers the average cost per-patient. With this in mind, it should be highlighted that the purchase cost of personalised instrumentation for TKA is more expensive than conventional TKA. Differences in actual implant costs are negligible, and are therefore unlikely to affect the cost-efficiency of implementing PSI and/or SUI for TKA. For example, the implant described in this particular study is not sold at a premium price; instead, it is sold at the same price as leading knee systems. However, instrument costs are greater for personalised TKA. TKA with PSI and reusable instrumentation have been reported to cost £723.73 per person (Attard et al. 2019). This cost was reduced to £610.00 when SUI were used in combination with the PSI. This is an additional cost of up to £300 per person when compared to traditional approaches to TKA. The increased cost of the instrumentation may be offset by reduced inpatient stay following personalised TKA, however. Earlier discharge may also reduce the patient’s likelihood of developing a nosocomial illness (O’Connor et al. 2020; de Caro, Hirschmann, and Verdonk 2020).
One limitation to this study is the lack of long-term data on the failure, infection, and readmission rates of patients undergoing TKA with PSI and SUI. Future research on the outcomes of personalised TKA should therefore follow patients up for longer.
3. Conclusion
Over the next few months, orthopaedic surgeons and OR staff will be returning to the OR with longer elective waiting lists, but a potentially limited daily capacity for OR use. The pressure to return to business-as-usual and accelerate throughput will be heightened by changes to departmental budgets and rising expenditures in certain areas (particularly infection control and testing for COVID-19) (O’Connor et al. 2020; de Caro, Hirschmann, and Verdonk 2020). Orthopaedic departments will need to adapt to the crisis by increasing OR efficiency, whilst maintaining good clinical outcomes and standards of care (O’Connor et al. 2020).
This article has described how our team optimises OR efficiency both intra-operatively and between cases. Although the instrumentation used in TKA with PSI is more expensive, the reduced hospital stay may result in a negligible cost difference overall. Combining this approach with SUI also has ergonomic benefits, potentially reducing the number of OR staff required to prepare the OR. SUI also have benefits for infection control. TKA with PSI and SUI is therefore economic and appropriate for orthopaedic departments resuming elective procedures ‘post’ pandemic. Importantly, combining this protocol with an increased OR ventilation rate may enable orthopaedic departments to return to their usual daily OR capacity for elective TKA.
Conflict of Interest
The research on which this article was based was indirectly funded via a grant from Medacta International. However, it was conducted independently and Medacta did not have sight of any results until accepted in a peer-reviewed scientific journal. GT and LCB receive indirect institutional research funding from Medacta. LCB receives a stipend for teaching at Medacta educational events.