INTRODUCTION
Total knee arthroplasty (TKA) and total hip arthroplasty (THA) are common surgical interventions for treating end-stage osteoarthritis in patients that have not responded to conservative treatment such as physical therapy or injections (Petterson et al. 2024). TKA and THA are among the most frequently performed procedures worldwide, ranking second and fourth, respectively, in most frequently performed procedures in the operating room with 1 million TKA and 594,000 THA cases performed in 2022 (McDermott and Liang 2021). By 2040, TKA cases are projected to rise to 2.7 million cases annually and THA to 2.1 million (Scuderi and Mont 2025). The goals of TKA and THA are to reduce joint pain, restore joint function, and improve patients’ quality of life (Varacallo et al. 2024). Due to the soft tissue damage sustained during surgery, patients experience high levels of pain and inflammation post-op. Patients often report severe post-op pain with 58% of patients reporting severe pain after a TKA and 47% of patients after a THA (Wylde et al. 2011). Opioids have long been the primary medication used to manage post-op pain. However, opioids carry well-documented risks, including dependence, constipation, mental status changes, fall risk, and respiratory depression.
Orthopedic surgeons account for 7.7% of all opioid prescriptions in the United States, ranking as the highest prescribing surgical specialty, and the third highest prescribing specialty, following family physicians and internists (Waljee et al. 2023). Mismanaging pain can lead to patients developing an opioid addiction; several studies have shown that as much as 69% of patients are on opioids at least 90 days after their TKA and 20% for THA (Ward et al. 2022; Tay et al. 2021). Reducing opioid use should be a top priority for physicians, as opioid overdoses made up 80,000 out of 105,000 drug overdoses in 2023 (Centers for Disease Control and Prevention (CDC), 2024) Other side effects of opioids include sedation, nausea, constipation and respiratory depression (CDC, 2024). Notably, opioid prescribing patterns following TKA vary widely, with some studies reporting up to 60% higher discharge doses compared to other surgical procedures (Dawson et al. 2024). Opioid consumption following total joint arthroplasty remains among the highest of all surgical procedures, with patients consuming an average of 24.0–85.3 pills after TKA and 33.1 pills after THA (Dawson et al. 2024; Atwood et al. 2021).
Patients receiving IV opioids in the Post-Anesthesia Care Unit (PACU) have a higher likelihood of filling an opioid prescription within 90 days after their surgery (Daigle et al. 2025). Even seemingly harmless opioid prescriptions carry significant risk, as the likelihood of long-term use is approximately 6% after just one day of therapy and increases to nearly 20% after only 10 days of use (Shah et al. 2017). Given the downsides associated with opioid prescribing, physicians should look for non opioid based interventions to control pain for patients after a total joint arthroplasty.
Suzetrigine (Journavx), a novel sodium channel blocker, represents a new option for pain management. This orally administered agent targets voltage-gated sodium channels (VGSCs) in the peripheral nervous system, specifically Nav1.8, which play a key role in initiating and transmitting nociceptive signals to the central nervous system. Blocking these channels reduces the excitability of pain-transmitting neurons without affecting motor function. The target receptor, Nav1.8, is not expressed in the brain and therefore mitigates opioid related adverse effects. Suzetrigine, unlike opioids, does not interact with μ receptors, which are linked to addiction.
The goal of this study was to determine if the addition of suzetrigine to an effective, previously described, low swelling, low opioid peri-operative protocol would provide additional reductions in rescue opioid medications in first and second stage recovery as compared to baseline.
METHODS
This study was designed as a retrospective, non-randomized, cohort, single-site study.
The site used was Apex Surgical in Westmoreland, NY. All total joint procedures were conducted by a single surgeon. The study protocol was reviewed and approved by the Institutional Review Board for the protection of Human Subjects of Mohawk Valley Health System in Utica, NY. A total of 240 patients were included in the study: 120 with TKA and 120 with THA. Patients were divided into control (no suzetrigine) and experimental (suzetrigine) groups within each procedure type. Each cohort consisted of 60 patients. The control cohort comprised the last 60 cases performed before the introduction of suzetrigine, while the experimental cohort included the first 60 cases following implementation of preoperative suzetrigine administration. Patients in the experimental cohort received one dose of 100mg of suzetrigine PO preoperatively at least 90 minutes before the incision was made.
All patients in both cohorts underwent cemented TKA with kinematic alignment, using the same prosthesis. All cases included patella resurfacing without tourniquet use. All patients undergoing a THA had an anterior approach using cementless implants, using a specialized table and capsulectomy. The surgeon had previously developed separate multimodal perioperative protocols for TKA and THA, which were used for all cohorts (Wickline et al. 2023; 2025; 2020). Patients received the same education booklet, watched the same pre- and postoperative videos, and followed the same at-home physical therapy protocol based on their surgery.
Patient demographic information was recorded, including age, surgical side, sex, BMI and ASA score. For all patients, the dose of fentanyl administered intraoperatively PACU was recorded. The same standard anesthesia protocol was used intraoperatively for all cohorts, which included general anesthesia using propofol with sevoflurane and fentanyl. Any additional fentanyl use in the PACU or opioid use in phase two of recovery was also recorded for patients. Patients who reported a pain score ≥7 and stayed awake were given additional opioids as part of the pain protocol. The total morphine milligram equivalent (MME) was calculated for patients using the conversions in the NYS Prescription Monitoring Program Registry. The conversion rates used were 0.1 MME/mg for Tramadol, 1.0 MME/mg for Hydrocodone, 1.5 MME/mg for Oxycodone and 0.3 MME/mcg for IV fentanyl. The opioid use was then compared for each procedure between the control and experimental cohorts.
RStudio (version 2024.12.0+467) was used to perform all statistical analyses and make all graphs. Chi-square tests were used to determine significance for the percentage of patients taking opioids during each phase of recovery. A Welch’s t-test was used when comparing fentanyl use and MME consumed.
RESULTS
In total, 240 patients were enrolled in the study: 120 TKA and 120 THA. Each cohort was comprised of 60 patients. There were no significant differences in the demographic or comorbidity profiles between the control and suzetrigine groups within either the TKA or THA cohort (Table 1A and Table 1B).
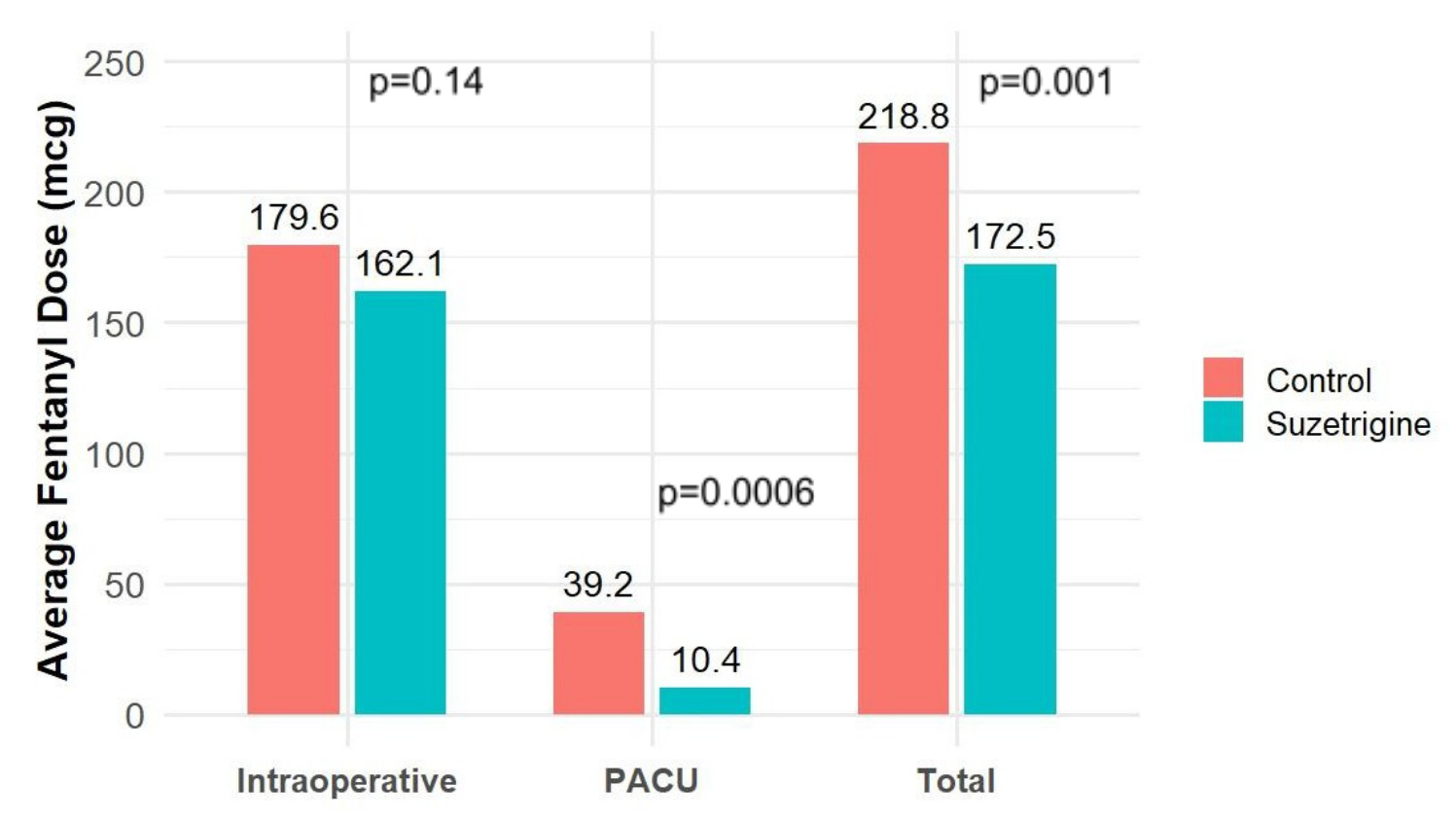
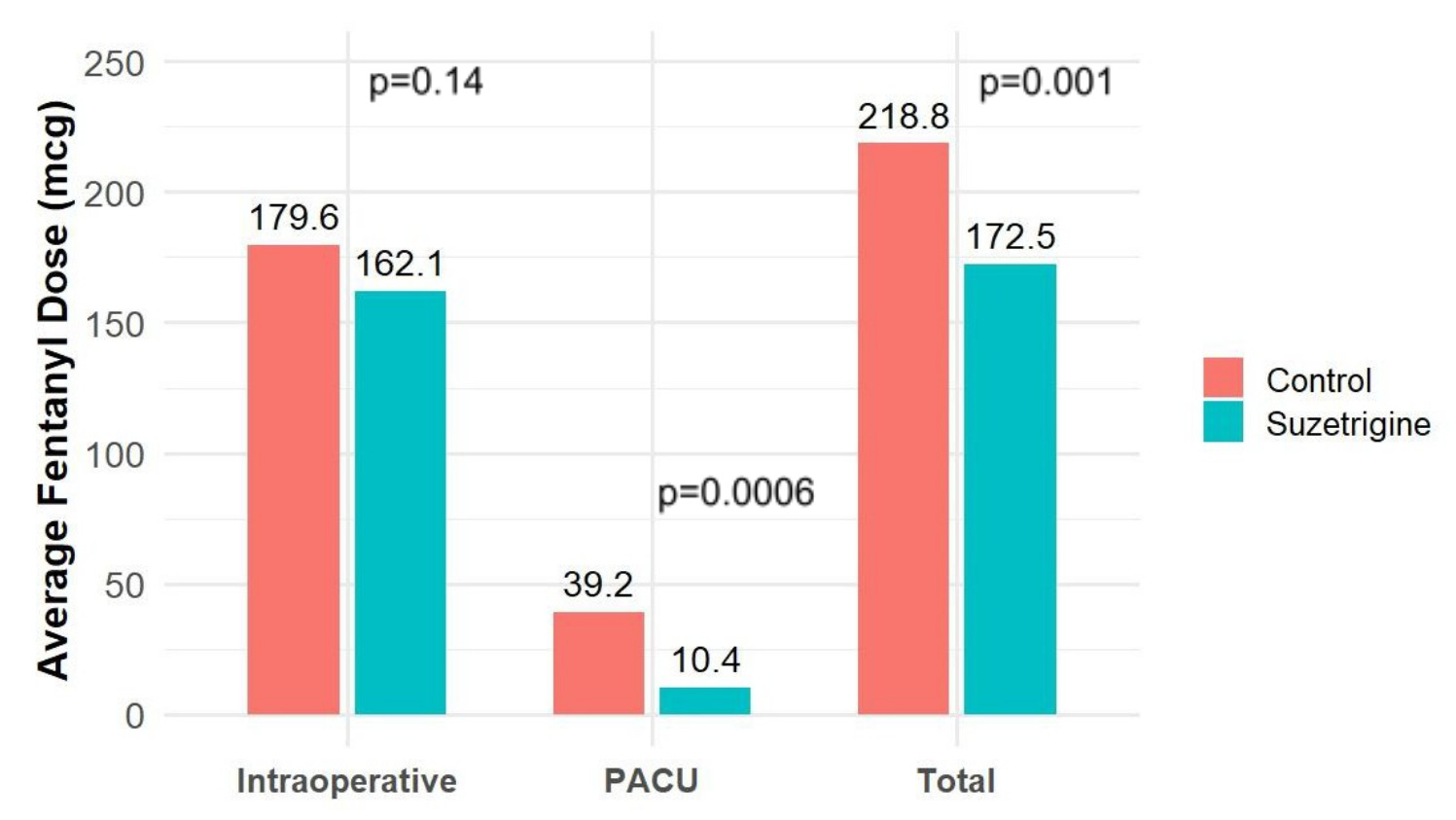
The dose of fentanyl was recorded for patients undergoing a TKA. There was no difference in the intraoperative fentanyl that was used between the experimental and control cohort (p=0.14) (Figure 2).
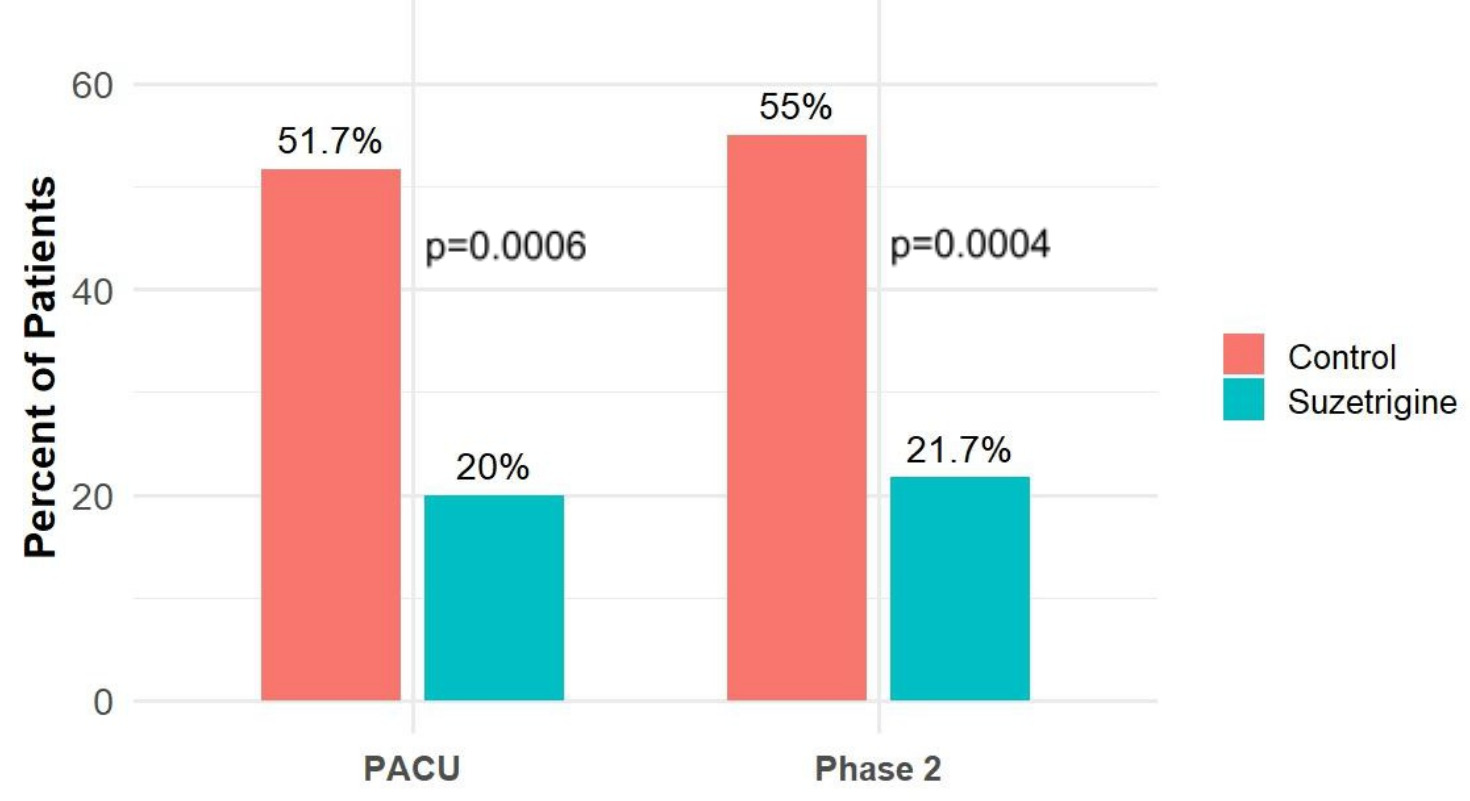
In the PACU, following a TKA, 51.7% of patients in the control cohort needed additional fentanyl compared to 20% in the experimental cohort (p=0.0006) (Figure 1). The patients in the control cohort received an average of 39.2 mcg of fentanyl per patient compared to 10.4 mcg per patient for the experimental (p=0.0006) (Figure 2).
In phase 2 recovery, 55% of TKA patients in the control cohort needed a rescue opioid compared to 21.7% of patients in the experimental cohort (p=0.0004) (Figure 1). The average MME given per patient in phase 2 was 3.2 for the control cohort compared to 1.2 for the experimental (p=0.0001) (Table 2).
The total average fentanyl use per TKA patient was 218.8 mcg for the control and 172.5 mcg for the experimental (p=0.001) (Figure 2). The total MME given to patients while in the surgical center was 68.8 for the control vs 53 for the experimental showing a 23% decrease (p=0.0002) (Table 2).

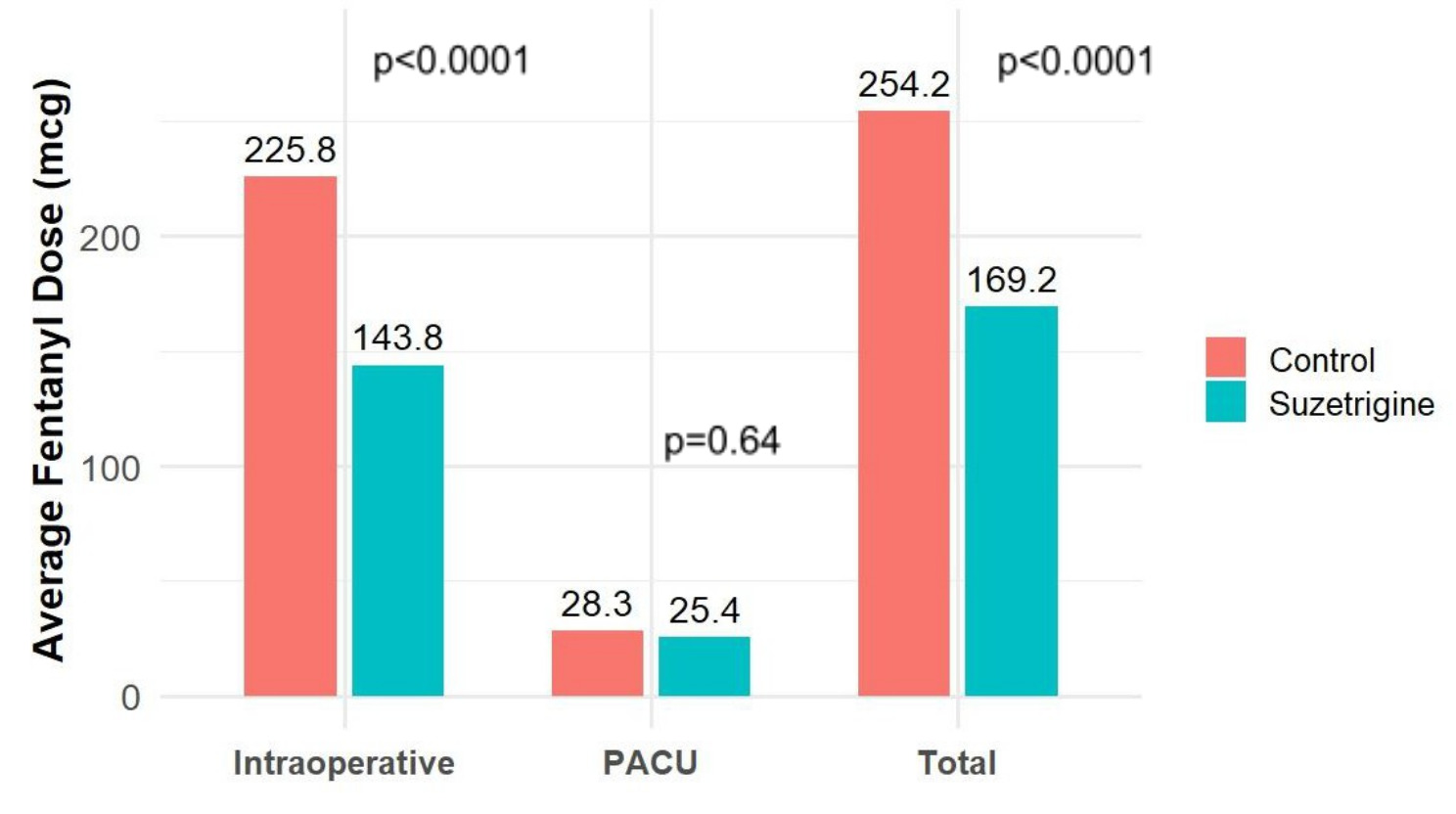
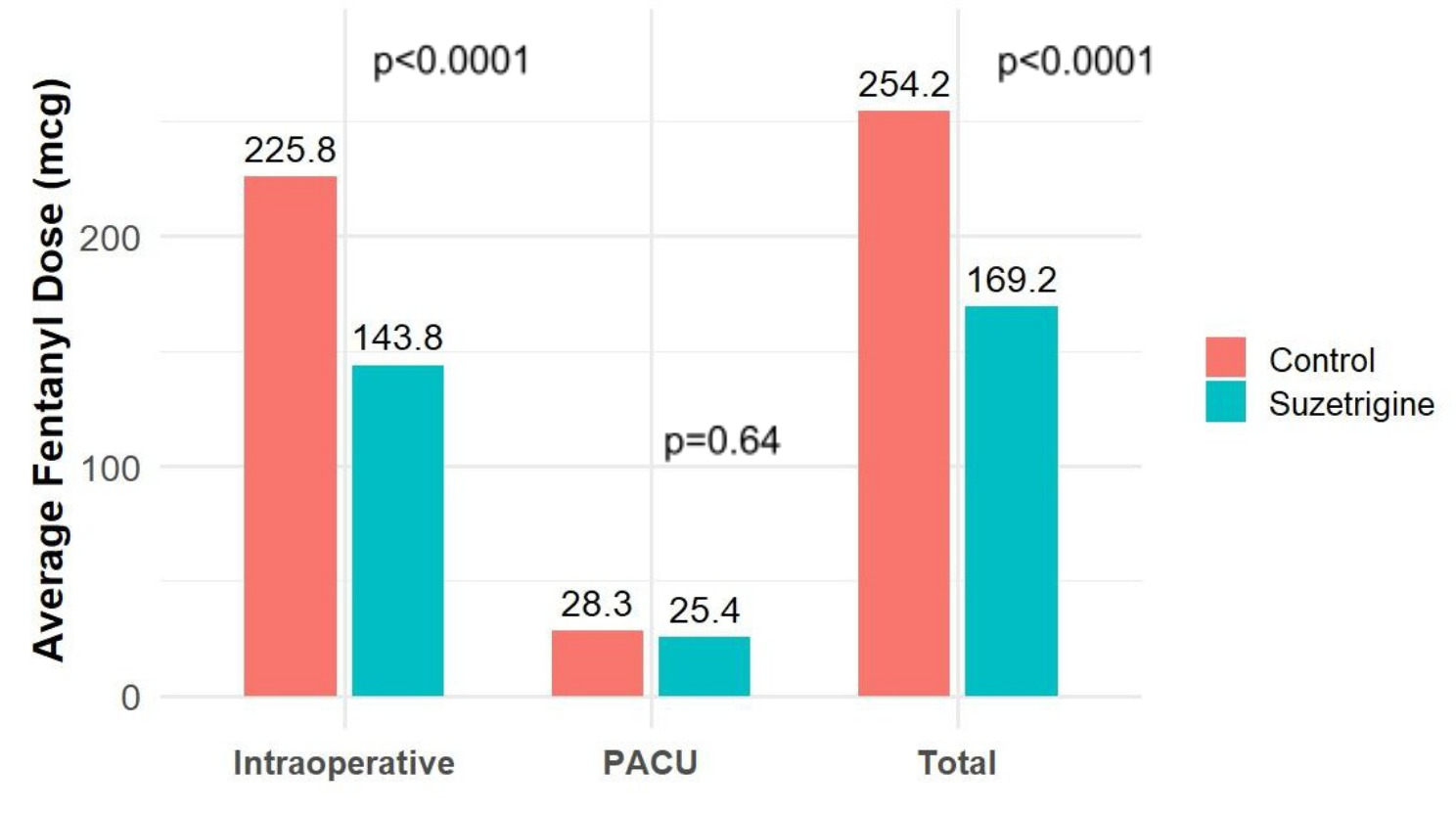
The dose of fentanyl was recorded for patients undergoing a THA. The intraoperative fentanyl use per patient was 225.8 for the control cohort and 143.8 for the experimental cohort (p<0.0001) (Figure 4).
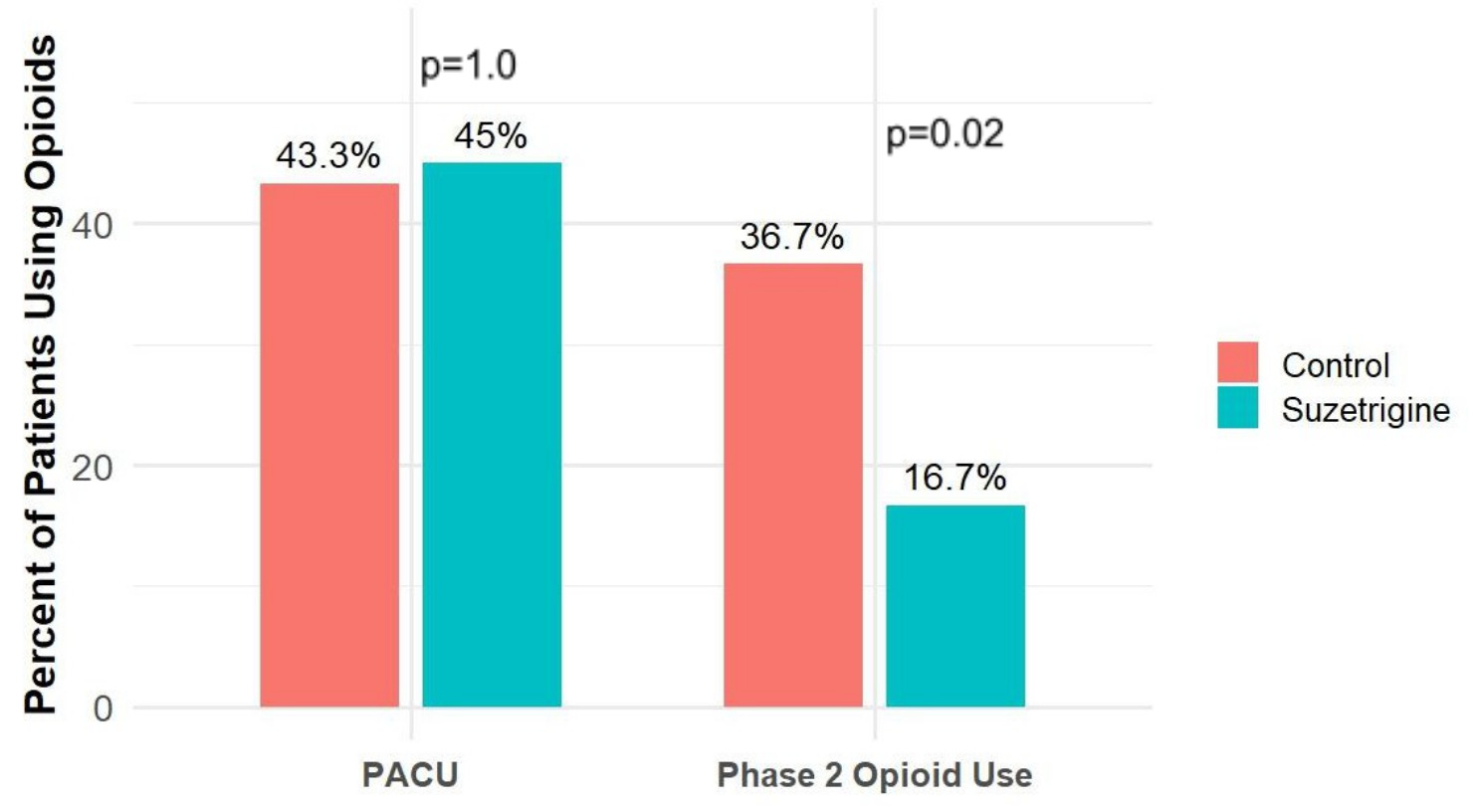
Following a THA, in the PACU there was no significant difference in the percentage of patients requiring additional fentanyl (p=1.0) (Figure 3). There was also no significant difference in the amount of fentanyl given per patient in the PACU (p=0.64) (Figure 4).
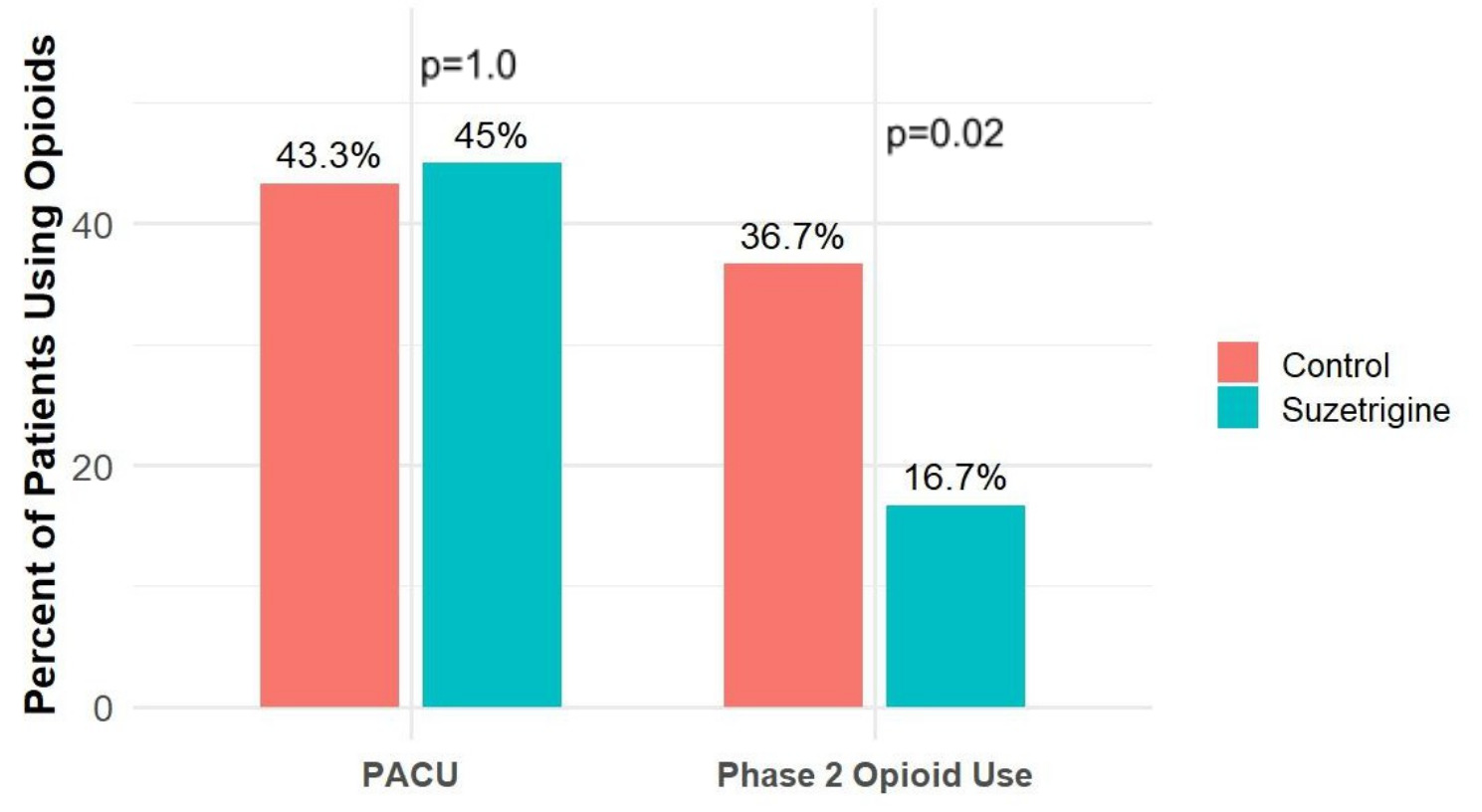
In phase 2 of recovery 36.7% of patients in the control cohort needed a rescue opioid compared to 16.7% of patients in the experimental cohort (p=0.02) (Figure 3). The average MME given per patient in phase 2 was 2.1 for the control cohort compared to 1.0 for the experimental (p=0.02) (Table 3).
The average fentanyl use per THA patient was 254.2 mcg for the control and 169.2 mcg for the experimental (p<0.0001) (Figure 4). The total MME given to patients while in the surgical center was 78.4 for the control vs 51.8 for the experimental showing a 34% decrease (p<0.0001) (Table 3).
DISCUSSION
Opioids were responsible for 80,000 overdose deaths in 2023, and it has been shown that opioid prescriptions for as little as 10 days put patients at a 20% risk for long term use (Shah et al. 2017; CDC, 2024). Suzetrigine appears to be a safe, non-narcotic intervention for controlling acute pain after a total joint procedure without opioid related adverse effects. The goal of this study was to determine if preoperative suzetrigine lowered opioid use intraoperatively, in the PACU, and in phase 2 recovery following a TKA or THA. Previous studies have associated patients who receive opioids in the PACU have a higher risk of filling an opioid prescription within 90 days of their surgery (Daigle et al. 2025).
Pain following joint replacement is multi-factorial. Early multimodal protocols added a periarticular local anesthetic, following the addition of NSAIDs and acetaminophen. These medications focused on specific pain receptors and made an impact on patient recovery (Stevenson and Wickline 2020). Subsequent protocols focused on swelling reduction to further enhance postoperative pain control and earlier functional recovery (Wickline et al. 2023; 2025). Since FDA approval of suzetrigine, anecdotal reports have suggested a range of responses from miraculous to negligible in regards to pain control and opioid usage. It is the senior author’s opinion that, similar to adding acetaminophen or NSAIDs, surgeons should not expect to immediately transition from prescribing 100 oxycodone to opioid free recovery when prescribing suzetrigine.
This study strongly suggests that preoperative suzetrigine blockade of peripheral nerve sodium channels (Nav1.8) is a useful adjunct for day of surgery pain control. Clear opioid reduction was identified for both TKA and THA compared to control subjects. The total MME consumption in the facility per patient was reduced from 68.8 MME to 53.0 MME (p=0.0002) following a TKA showing a 23% reduction (Table 2). For patients receiving a THA this was reduced from 78.4 MME to 51.8 MME (p<0.0001) making a 34% reduction (Table 3). Follow-up studies measuring secondary measures such as failure to launch, time to discharge, nausea/vomiting, falls, and hypotension may provide further incentive to add suzetrigine to the preoperative multimodal cocktail. These findings imply that persistent blockade in the first several weeks of recovery may continue to provide opioid reduction compared to current protocols and warrant urgent research.
The limitations of this study were that all cases were performed by a single surgeon at one center and was retrospective in design. It would be ideal if other sites could perform a similar study to verify that suzetrigine is an effective intervention that reduces opioid use on the day of surgery. This would confirm that the medication works as intended. Its effects may be more measurable on the day of surgery rather than measuring opioid reduction during the first several weeks postoperatively where significant variability in recovery protocols exist. Also, because this is a retrospective study, certain parameters, such as pain scores and preoperative function scores would have been helpful to collect and compare between cohorts. Additionally, patients enrolled in this study were not assessed for opioid naive status.
Future studies examining longer term outcomes will be useful for determining the overall impact suzetrigine may have on recovery after a TKA or THA. Patients enrolled should be opioid naive, as preoperative opioid use could impact opioid requirements on the day of surgery. It is recommended that day of surgery data should be collected and analyzed independently of data collected in the first several weeks after surgery due to the wide variations in recovery protocols.
In summary, adding suzetrigine as a preoperative intervention, appears to decrease the overall amount of narcotics that patients need, PACU opioid use, and the need for a rescue opioid in phase 2 of recovery.