
Introduction
Management of massive acetabular bone loss remains one of the most complex challenges in revision hip arthroplasty. Patients presenting after trauma, infection, multiple prior surgeries, or failed fixation frequently demonstrate segmental and cavitary defects that compromise both mechanical support and the quality of host bone required for durable biological fixation (De Martino et al. 2019; Sanghavi et al. 2024). In advanced defect patterns such as Paprosky type III defects or pelvic discontinuity, conventional hemispherical revision components and modular augments may be insufficient to restore hip biomechanics and achieve long-term mechanical stability (Pandey et al. 2023).
The reconstructive challenge is amplified in the setting of prior infection. Post-infectious acetabular defects are characterized not only by bone loss, but also by altered local biology, scarred soft tissues, retained hardware from previous procedures, and weakened bone structure. Successful management typically requires staged reconstruction, beginning with debridement and antibiotic spacer placement, followed by definitive reconstruction only after infection eradication is achieved (Craig et al. 2022; Sporer 2020). Even after infection control, the mechanical environment remains demanding, with limited viable host bone available for fixation and altered load transfer across the pelvic ring.
Custom triflange acetabular components have emerged as a reconstructive strategy for severe segmental and cavitary bone loss, especially in Paprosky type III defects and pelvic discontinuity (Broekhuis et al. 2023; Alexander et al. 2023). Designed using patient-specific computed tomography data, these implants allow fixation across the ilium, ischium, and pubis, enabling restoration of the hip center of rotation while maximizing contact with remaining host bone (Scharff-Baauw et al. 2021). By spanning multiple pelvic columns, triflange constructs provide immediate mechanical stability in situations where conventional hemispherical components and modular augments are insufficient, thereby creating conditions favorable for long-term biological fixation in the setting of compromised bone stock.
Post-traumatic acetabular defects can be more difficult because of distorted anatomy, retained hardware, prior infection, and compromised bone quality (Sanghavi et al. 2024). When infection is present, staged reconstruction is often required, beginning with hardware removal and antibiotic spacer placement, followed by definitive reconstruction once infection eradication is achieved (Craig et al. 2022; Sporer 2020). In these settings, custom implants may play a crucial role in restoring pelvic continuity and function when standard revision options are insufficient (Broekhuis et al. 2023; Alexander et al. 2023).
However, reconstruction in the post-infectious setting raises additional considerations beyond geometry alone. Implant material properties influence load transfer, stress distribution, and the biological interface between implant and host bone (Cheng et al. 2019; Morrison et al. 2017). Although metallic triflange constructs have demonstrated success, concerns related to stiffness mismatch, stress shielding, and imaging artifact remain relevant in complex revision scenarios (McCloskey et al. 2026; Broekhuis et al. 2023; Alexander et al. 2023).
Compared with conventional metallic implants, PolyArylEtherKetone (PAEK) materials such as PolyEtherKetoneKetone (PEKK) demonstrate an elastic modulus closer to that of cortical bone, which may reduce stress shielding and promote more physiologic load transfer (Hong et al. 2024; Jackson et al. 2023). In addition, PEKK is radiolucent and produces minimal artifact on advanced imaging modalities, facilitating postoperative assessment (Vaishya et al. 2026). PAEK materials also demonstrate favorable mechanical strength and fatigue resistance, with properties influenced by polymer structure and processing (Gu et al. 2021) . Additive manufacturing of PAEK materials has enabled the development of patient-specific implants with complex geometries; however, most published clinical experience remains limited to selected applications, particularly in craniofacial reconstruction. These characteristics may influence load distribution at the bone–implant interface and improve radiographic evaluation, particularly in cases of compromised bone stock. Despite expanding clinical use, the role of PEKK in complex acetabular reconstruction remains incompletely defined in the current literature.
This case is notable not only for the severity of the defect, but for the reconstructive environment in which definitive treatment was performed. The combination of post-traumatic deformity, retained hardware, infection, and limited residual bone stock required a strategy in which both implant geometry and material selection were integral to surgical planning. To our knowledge, reports describing the use of patient-specific PEKK triflange implants in post-infectious acetabular reconstruction remain limited.
Case Report
A 67-year-old male presented with history of left hip pain and severe functional limitation following prior pelvic trauma and multiple surgical interventions. The patient sustained injuries in a motorcycle crash resulting in pelvic and acetabular fractures and subsequently underwent open reduction and internal fixation, followed by additional procedures involving the left hip.
His medical history was significant for hypertension, obesity (body mass index approximately 39–40 kg/m²), obstructive sleep apnea, neuropathy, depression, and prior traumatic brain injury. He was a former smoker.
Over time, the patient developed increasing difficulty with ambulation, requiring assistive devices including a walker and wheelchair. Functional decline persisted despite prior interventions.
On physical examination, the patient demonstrated an antalgic gait. Range of motion of the left hip was limited in all planes and associated with pain. At initial evaluation, measurements included approximately 5° of internal rotation, 20° of external rotation, less than 5° of adduction, 15° of abduction, and 80° of flexion, with a flexion contracture of approximately 20°.
Motor strength was generally preserved, although the patient reported subjective weakness in hip flexion and abduction. The surgical incision was well healed without persistent erythema or drainage. Neurovascular examination remained intact.
Diagnostic Assessment
The patient underwent comprehensive evaluation to define the etiology of progressive left hip pain, functional decline, and structural failure in the setting of prior high-energy pelvic trauma and multiple surgical interventions.
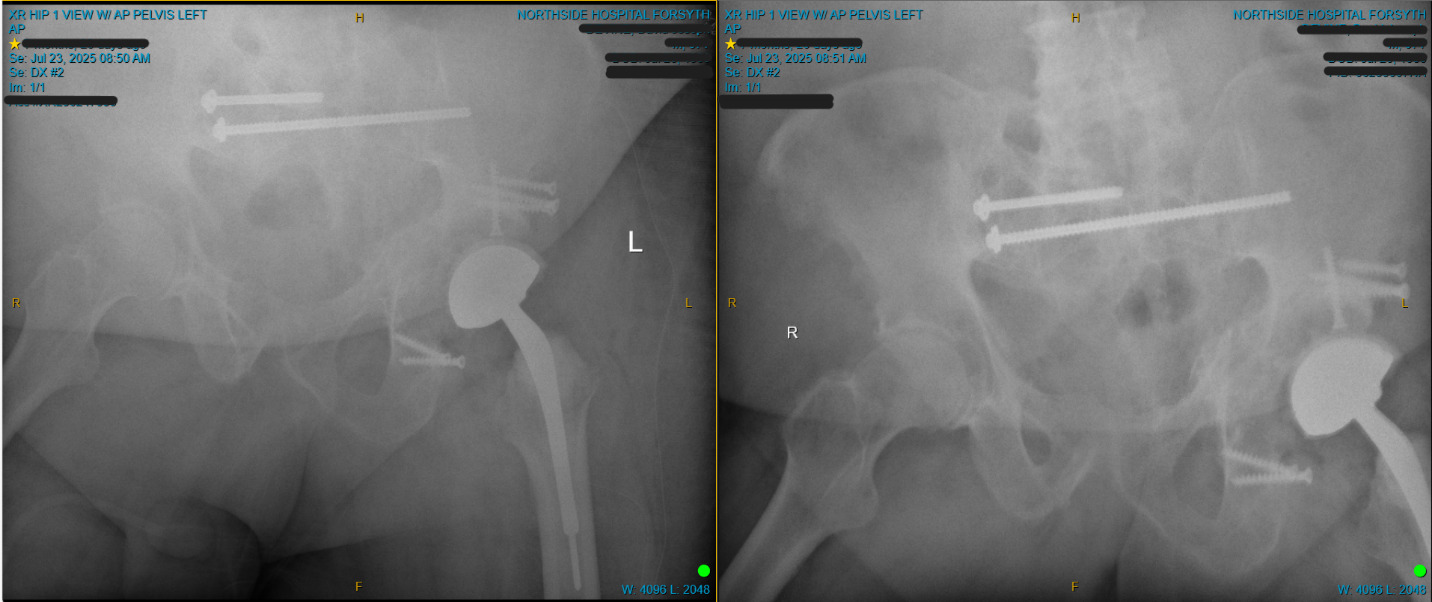
Initial radiographic assessment demonstrated advanced degenerative changes of the left hip, including traumatic dysplastic changes, joint space absence, femoral head deformity, and retained fixation hardware.
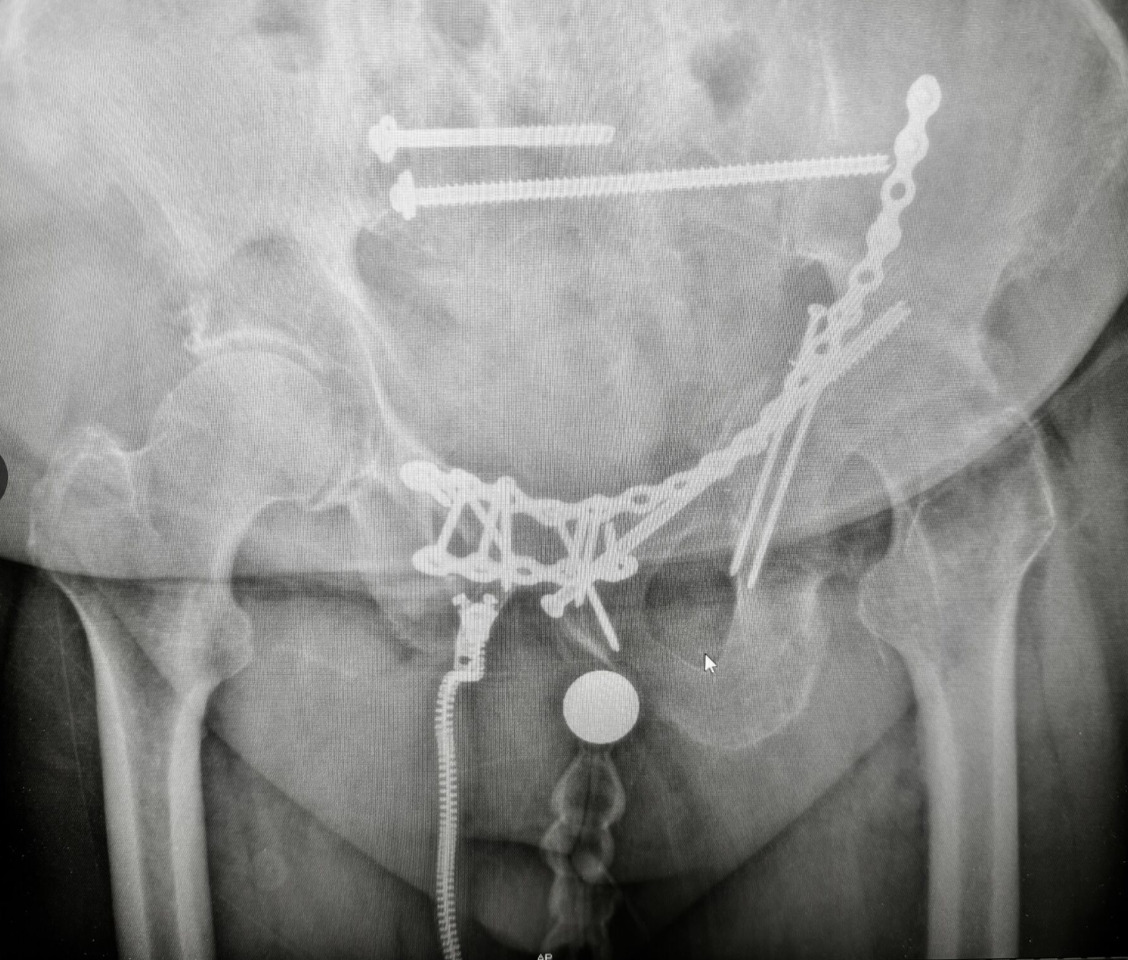
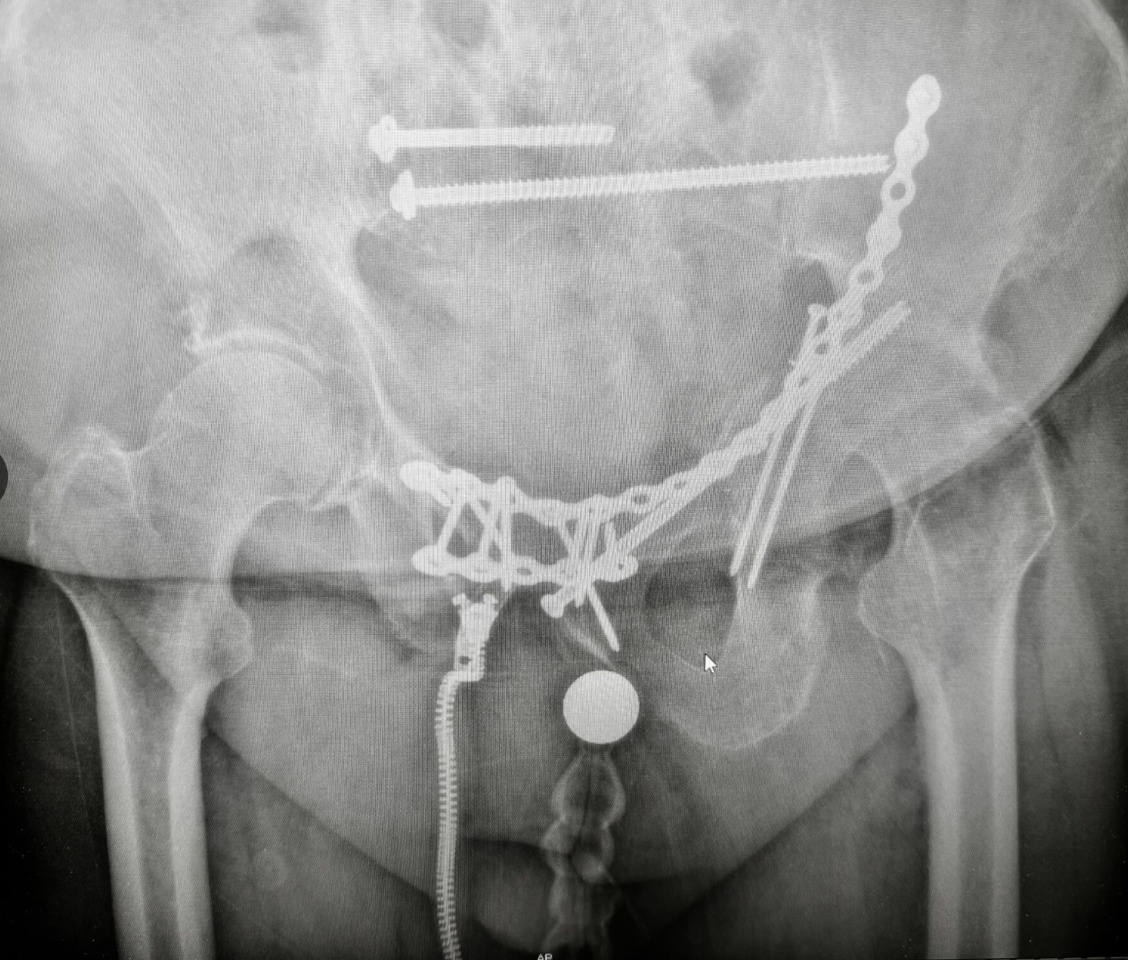
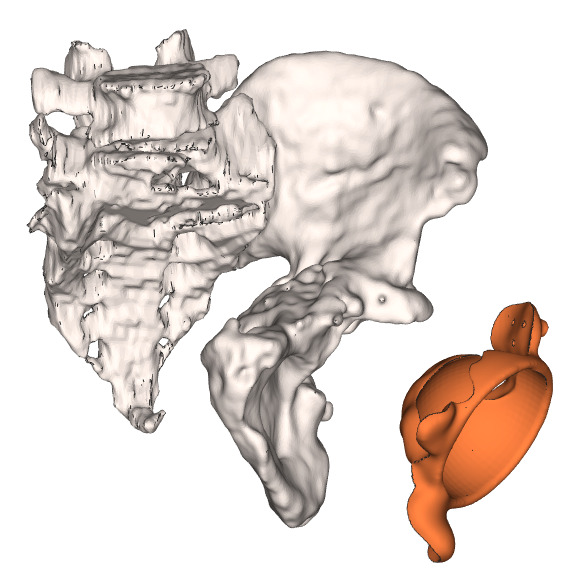
Computed tomography (CT) of the pelvis without contrast was obtained for operative planning and detailed characterization of the defect. Imaging demonstrated extensive post-traumatic and post-surgical changes involving the left hemipelvis, with retained hardware including anterior reconstruction plating extending across the pubic symphysis and into the left iliac bone, as well as multiple screws traversing the pelvic ring.
A long lag screw was identified breaching the acetabular articular surface and extending into the joint space, indicating direct hardware-related intra-articular compromise. Additional fixation elements along the medial acetabulum closely approximated the joint surface, further contributing to mechanical disruption.
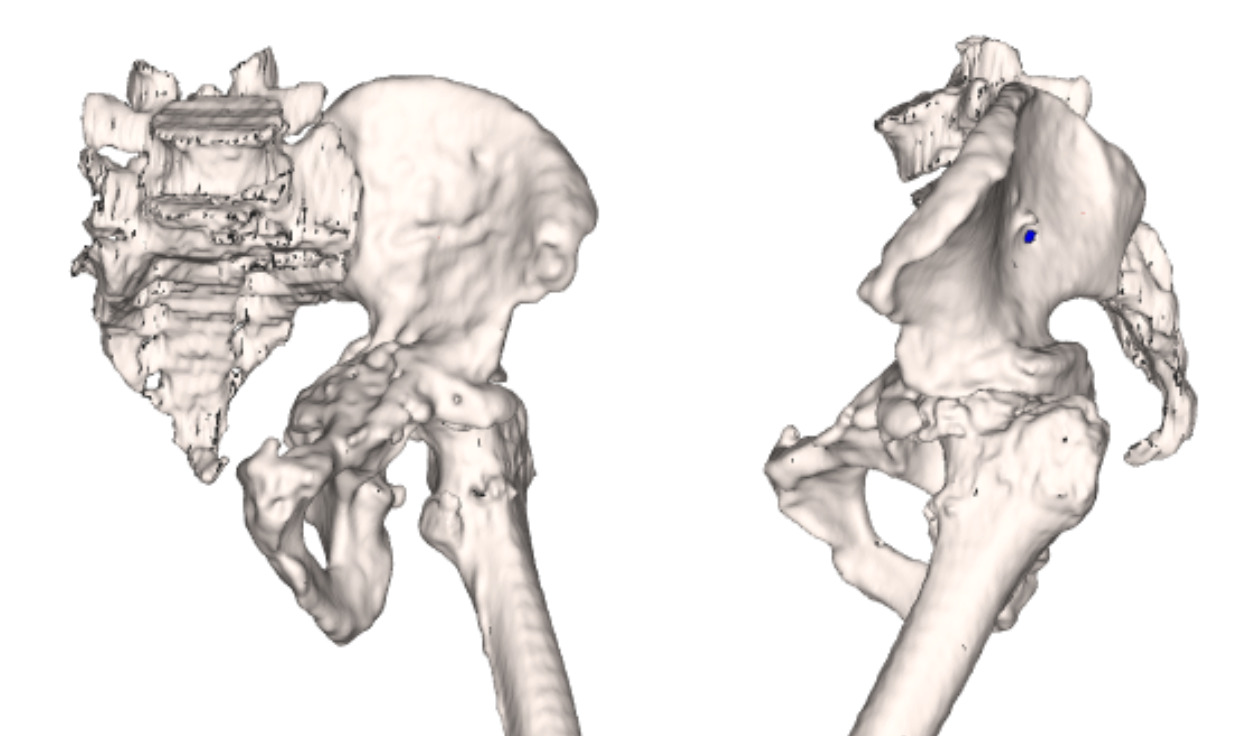
There was severe deformity of the left acetabulum with chronic remodeling and substantial widening of the acetabular socket. The posterior column demonstrated deformity with sclerosis and ghost tracts consistent with prior fixation. Heterotopic ossification was present along the medial and anterior acetabular walls, and the medial wall appeared thickened with focal ossification.
A focal region of near-complete bone loss was identified in the superomedial acetabulum, measuring approximately 16 × 22 mm. The femoral head demonstrated severe flattening and collapse of the articular surface with associated sclerosis, consistent with advanced degenerative change and avascular necrosis.

Additional findings included bony bridging across the pubic symphysis with anterior translation of the left pubic body relative to the right, as well as multiple screw tracks within the pubic bodies, superior pubic rami, and acetabulum. A cluster of asymmetrically enlarged left inguinal lymph nodes was identified, measuring up to approximately 2.4 × 1.5 cm, likely reactive in the clinical context. No large joint effusion or periarticular fluid collection was identified.
Laboratory evaluation demonstrated persistent abnormalities. White blood cell counts remained within normal limits, ranging from 7.8 to 9.1 ×10⁹/L. In contrast, there was consistent anemia, with hemoglobin values ranging from 8.2 to 8.6 g/dL and hematocrit ranging from 25.2% to 26.5%. Red blood cell counts ranged from 2.73 to 2.85 ×10¹²/L, and red cell distribution width was elevated (14.6–15.2%), consistent with a chronic inflammatory state. Platelet counts ranged from 165 to 292 ×10⁹/L.
Renal function remained stable, with creatinine values between 0.7 and 0.8 mg/dL and estimated glomerular filtration rate consistently greater than 60 mL/min/1.73 m². Serum glucose levels ranged from 105 to 110 mg/dL, and calcium levels ranged from 8.5 to 8.7 mg/dL.
Creatine kinase was elevated, with values of 943 U/L and 1419 U/L documented during the evaluation period.
Inflammatory markers were elevated, with C-reactive protein measured at 2.2 mg/dL and subsequently 5.1 mg/dL, with prior values reported up to 100 mg/L, consistent with a sustained inflammatory or infectious process.
Given the patient’s clinical presentation, prior hardware, and laboratory abnormalities, further evaluation for infection was pursued. The patient underwent biopsy and culture to assess for underlying infection. Synovial fluid analysis demonstrated elevated inflammatory markers, including a white blood cell count of 11,087 cells/µL and 87.4% polymorphonuclear cells, exceeding accepted thresholds for chronic periprosthetic joint infection. Synovial C-reactive protein was measured at 53.25 mg/L.
Next-generation sequencing (NGS) analysis identified Staphylococcus lugdunensis (relative abundance 83%). While molecular identification alone does not establish causality, this finding, in conjunction with clinical, laboratory, and imaging data, was considered supportive of a clinically significant deep musculoskeletal infection.
Infectious disease consultation was obtained, and the patient was treated with a course of intravenous antibiotics with serial clinical and laboratory monitoring.
Taken together, the findings demonstrated a severely compromised acetabulum characterized by post-traumatic structural bone loss, hardware-related intra-articular failure, advanced femoral head collapse, and superimposed chronic infection. In this setting, conventional reconstructive strategies were considered insufficient to provide durable fixation.
A staged surgical approach was therefore selected, consisting of hardware removal, debridement, and placement of an antibiotic spacer, followed by definitive reconstruction after completion of antimicrobial therapy and clinical assessment of infection control
Therapeutic Intervention
Given the combination of post-traumatic acetabular destruction, hardware-related intra-articular violation, femoral head collapse, severe soft tissue contracture, and chronic infection, a staged surgical strategy was undertaken after failure of nonoperative management, including activity modification, assistive device use, and pharmacologic pain control.
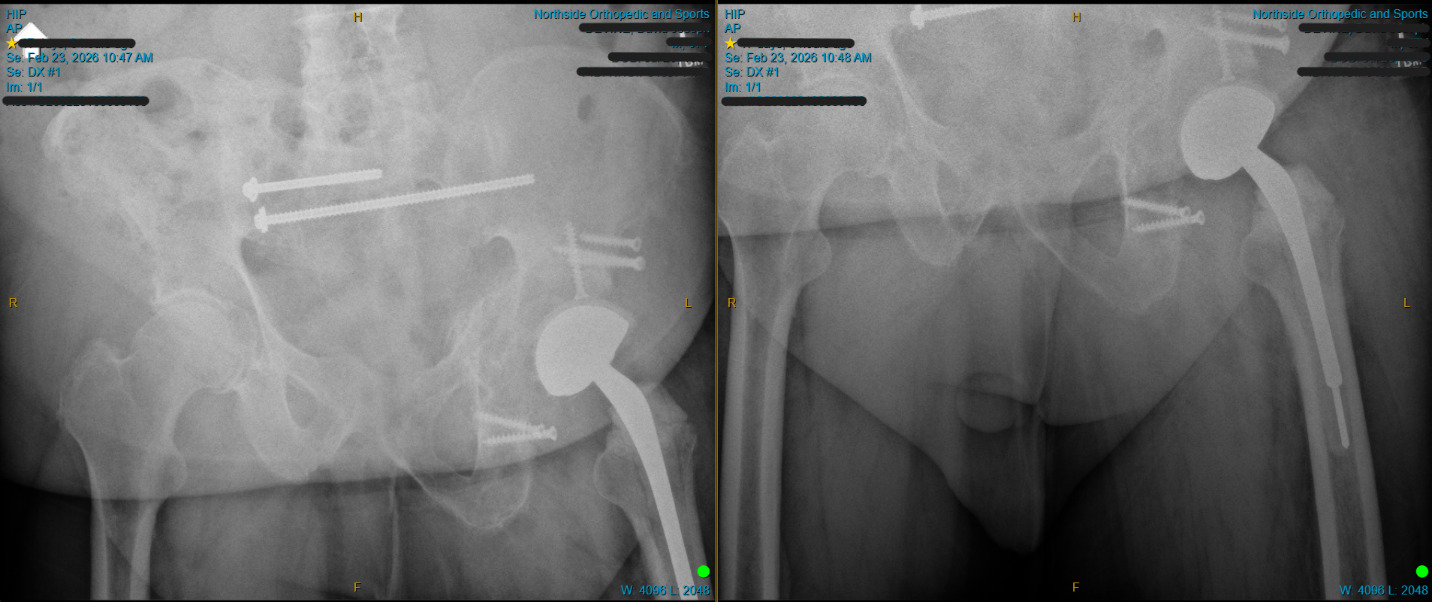
The patient underwent initial surgical management consisting of removal of retained hardware. Subsequent surgery was consistent with a total hip arthroplasty of the left hip, extensive irrigation and debridement, and placement of an antibiotic spacer. A direct lateral approach was utilized. Exposure was technically demanding due to dense scar tissue, heterotopic ossification, and markedly distorted anatomy related to prior trauma and multiple surgical interventions. Severe longstanding contracture was present, and the hip was essentially immobile at the start of the procedure, requiring extensive soft tissue release to achieve adequate mobilization and exposure.
The acetabulum demonstrated substantial structural compromise with severe bone loss and disruption of normal pelvic architecture, consistent with preoperative imaging findings. The femoral head exhibited advanced degenerative changes with collapse consistent with avascular necrosis. Approximately 5 mL of bloody synovial fluid was aspirated and sent for microbiologic analysis, and multiple intraoperative tissue specimens were obtained for culture. Thorough irrigation and debridement of nonviable and infected tissue were performed, followed by placement of an antibiotic-impregnated spacer to maintain joint space and provide local antimicrobial delivery.
Estimated blood loss was approximately 150 mL, and no intraoperative complications were encountered.
Postoperatively, the patient was admitted for monitoring and initiation of intravenous antibiotic therapy under infectious disease guidance. A peripherally inserted central catheter was placed to facilitate prolonged antimicrobial treatment. The postoperative course was stable, and the patient was discharged with continued intravenous antibiotics, wound care instructions, and protected mobilization. Weight-bearing was restricted, and the patient required assistive devices for ambulation. Serial clinical assessments and laboratory monitoring were performed during the interval period, demonstrating improvement in inflammatory markers and stabilization of symptoms consistent with control of the infectious process.
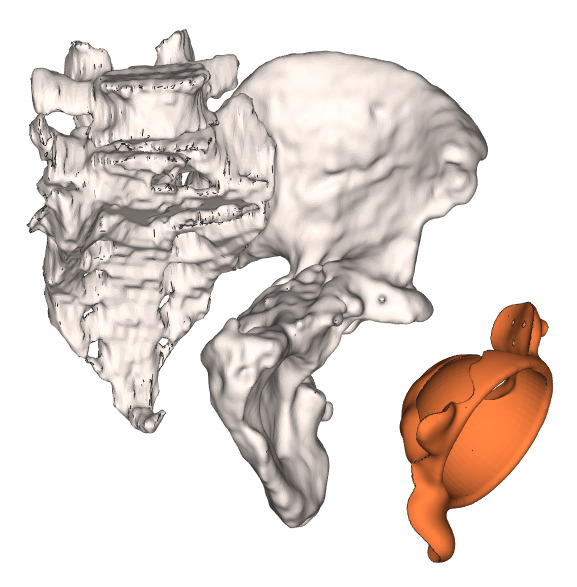
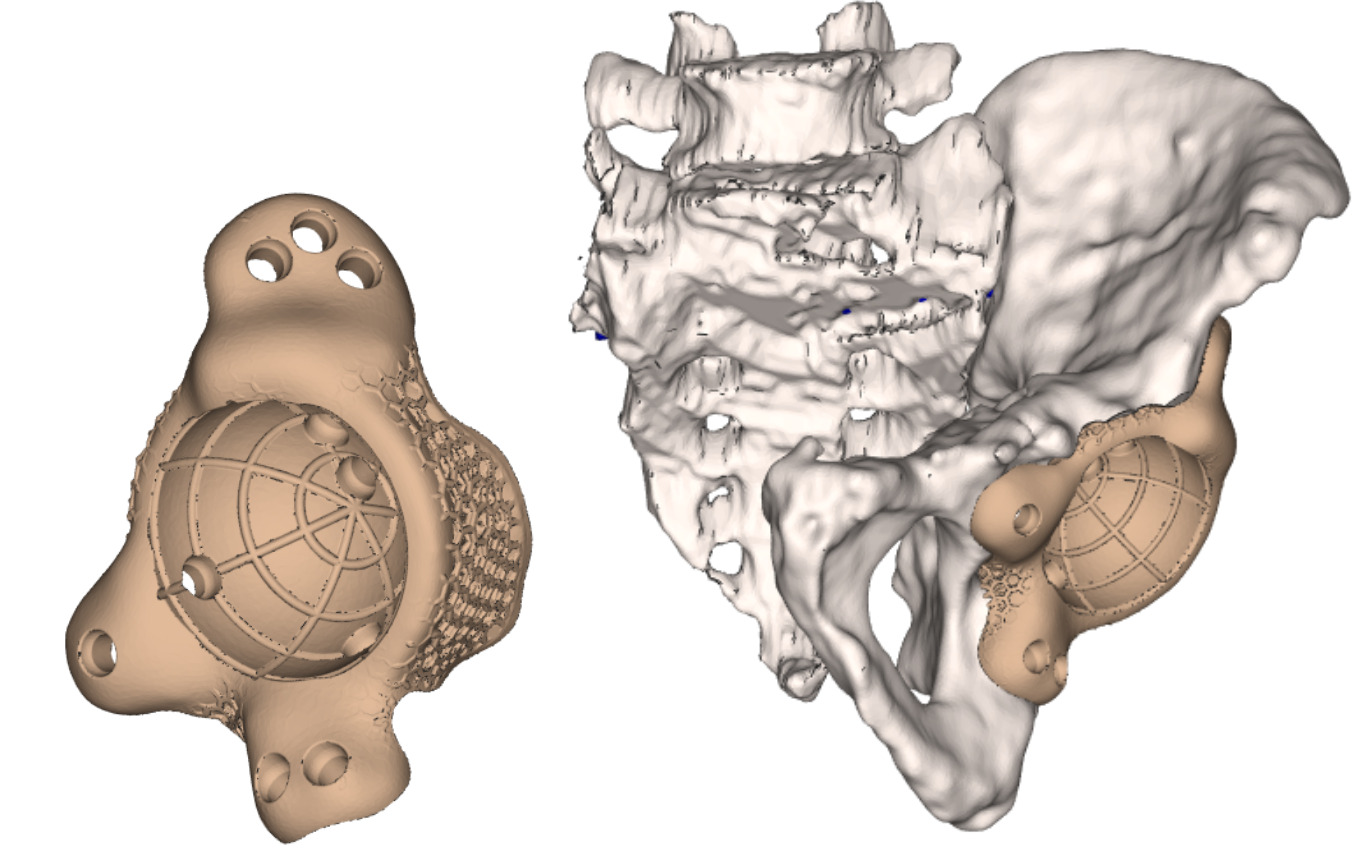
Following completion of antimicrobial therapy and clinical confirmation of infection control, the patient was indicated for definitive reconstruction. Given the severity of acetabular bone loss, pelvic deformity, prior hardware failure, and altered anatomy, conventional reconstructive options were deemed insufficient to achieve stable fixation or restore hip biomechanics. Preoperative planning was therefore performed using advanced imaging and three-dimensional reconstruction to design a patient-specific implant capable of addressing the segmental defect and restoring hip center.
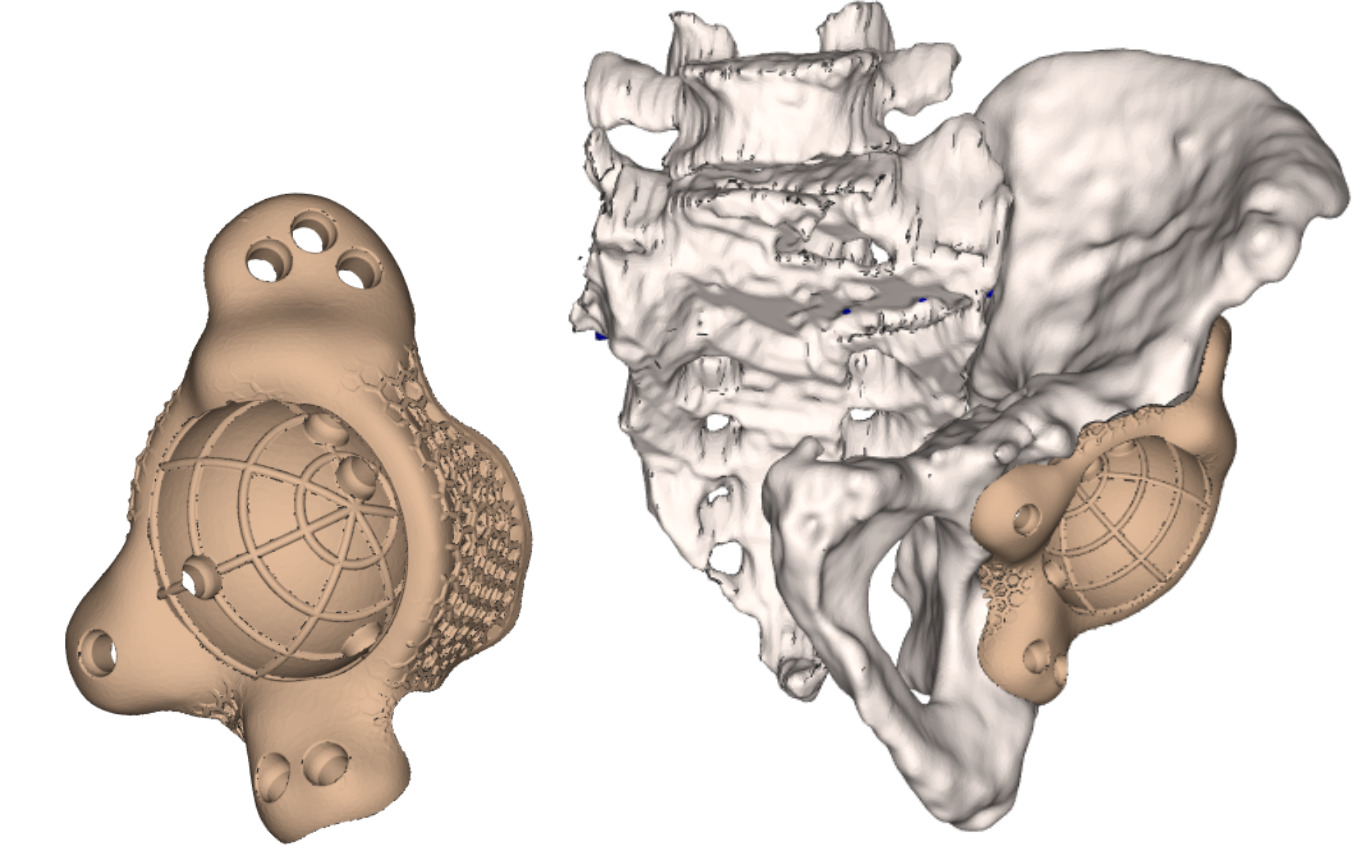
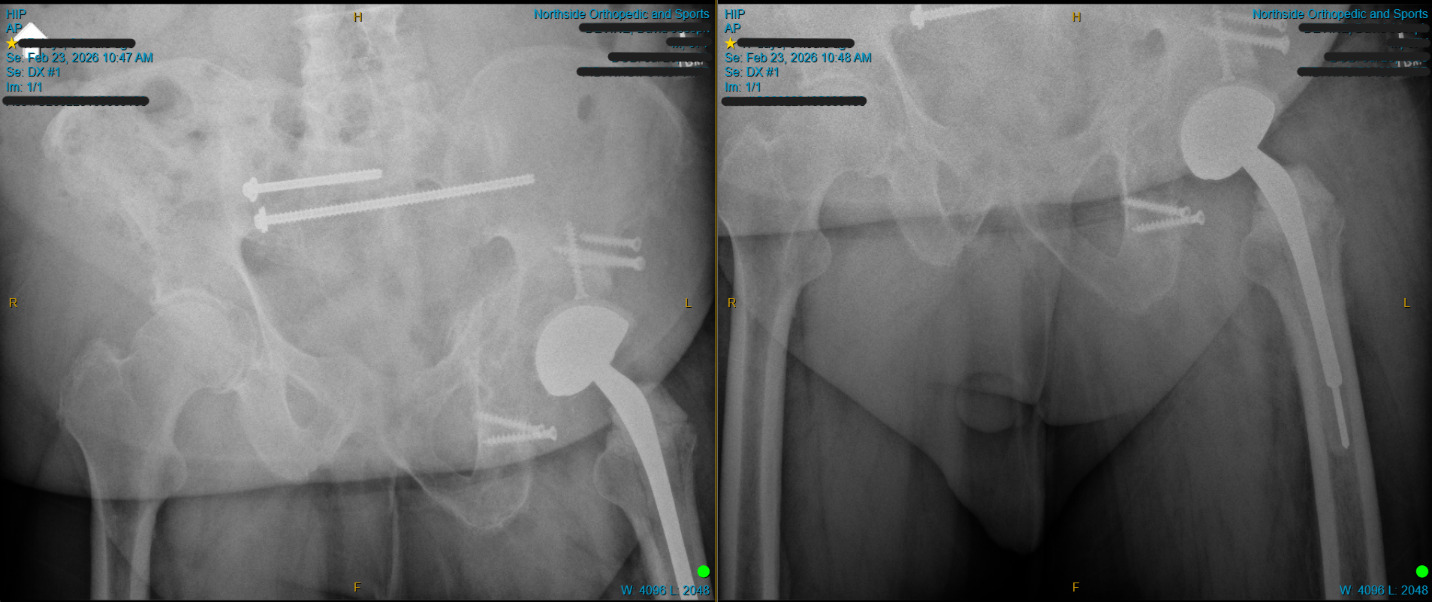
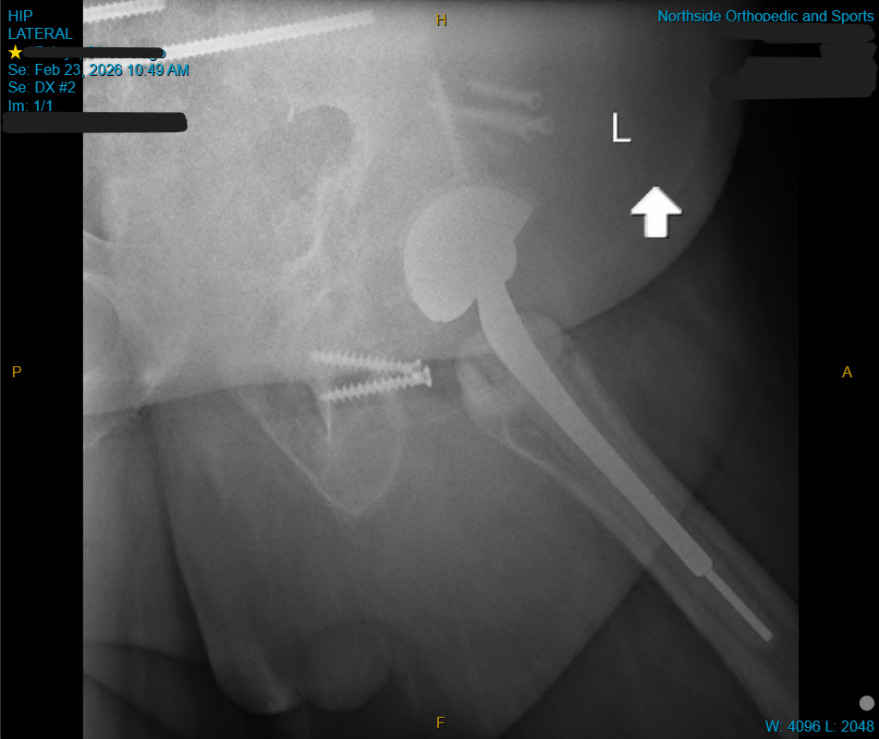
Definitive reconstruction was performed using a custom PEKK triflange acetabular component (OsteoFab® platform, Oxford Performance Materials). The implant was positioned according to the preoperative plan, with fixation achieved across the ilium, ischium, and pubis using multiple screws placed along preplanned trajectories to maximize fixation in available host bone. Additional soft tissue release was performed as necessary to allow reduction, and stable articulation was achieved following reconstruction.
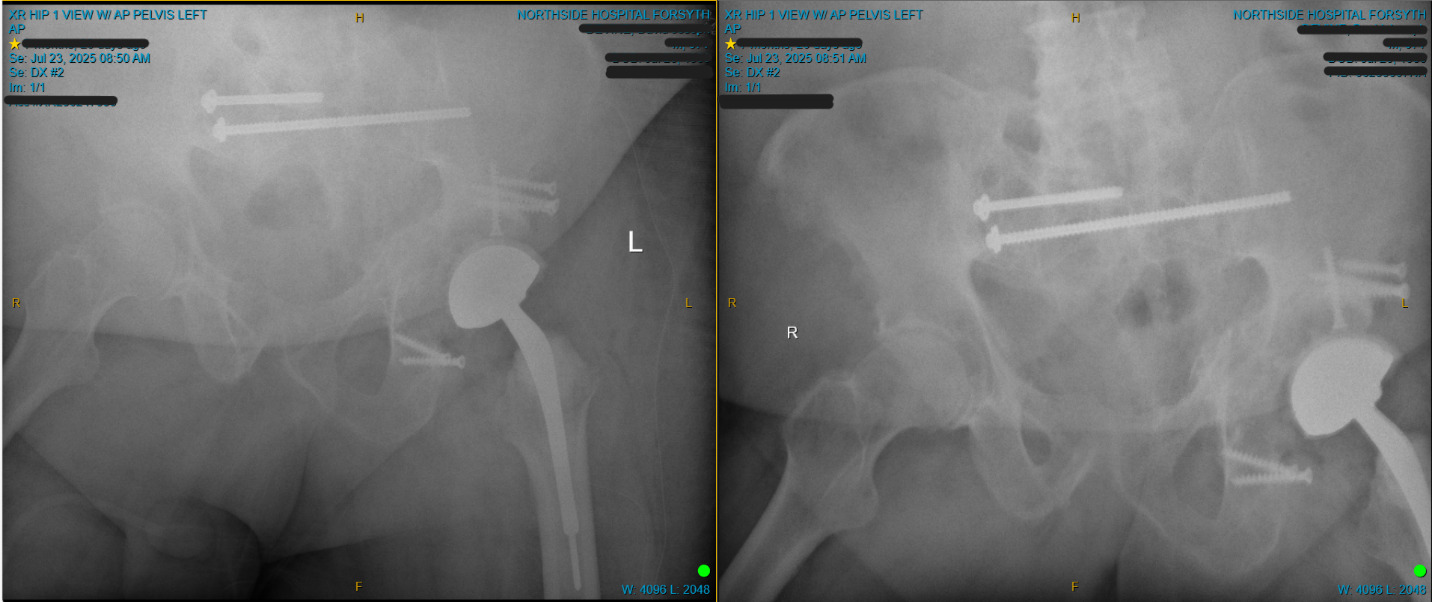
The procedure was completed without intraoperative complications. Postoperative recovery was uneventful, and the patient was managed with protected weight-bearing and a guided rehabilitation plan, with follow-up demonstrating stable implant position and continued clinical improvement. At most recent follow-up of approximately 7 months, the patient demonstrated progressive clinical improvement, including reduction in pain and improved functional status compared to the preoperative condition. Serial laboratory values showed no evidence of recurrent infection, and radiographic evaluation demonstrated stable implant position without signs of loosening or mechanical failure. No additional surgical intervention was required during this follow-up period.
Discussion
This case illustrates the complexity of managing post-traumatic acetabular defects in the setting of prior surgical intervention, hardware failure, and superimposed infection. The combination of structural bone loss, distorted pelvic anatomy, and compromised soft tissues represents a challenging reconstructive scenario in which standard techniques may not be adequate to achieve durable fixation or restore hip biomechanics.
Post-traumatic acetabular defects are frequently associated with altered load distribution, progressive joint degeneration, and loss of bone stock. In this case, prior fixation constructs failed, with hardware-related intra-articular violation contributing to further cartilage damage and mechanical deterioration. The presence of femoral head collapse and advanced degenerative changes reflects the cumulative effect of trauma, altered biomechanics, and delayed reconstruction.
Superimposed infection further complicated management and necessitated a staged approach. Laboratory findings, synovial analysis, and microbiologic data supported the diagnosis of a chronic infection. Next-generation sequencing identified Staphylococcus lugdunensis, an organism known for its potential virulence among coagulase-negative species. Although molecular diagnostics should be interpreted in conjunction with clinical findings and may be subject to limitations, including detection of non-viable organisms, the presence of this organism in a severely compromised joint environment was considered clinically relevant. Staged management with resection arthroplasty, thorough debridement, antibiotic spacer placement, and targeted antimicrobial therapy remains the commonly used approach in these cases, allowing for infection control prior to definitive reconstruction.
The degree of acetabular bone loss and pelvic deformity limited the applicability of standard reconstructive options, including hemispherical cups, augments, and cages. Custom triflange acetabular components provide a solution for severe segmental defects by enabling fixation across the ilium, ischium, and pubis while restoring hip center and load transfer. In this case, patient-specific design allowed accurate matching of the implant to the residual host bone and facilitated preoperative planning of fixation strategy.
The use of a custom PEKK implant represents an additional consideration. Compared with conventional metallic implants, PEKK offers an elastic modulus closer to cortical bone, radiolucency for improved postoperative imaging assessment, and favorable fatigue characteristics. Additive manufacturing further enables patient-specific designs adapted to complex defects. These properties may provide potential benefits in load sharing and evaluation of the bone-implant interface, particularly in complex revision settings. However, clinical evidence supporting the use of PEKK in large joint reconstruction remains limited, and its role in acetabular reconstruction continues to be defined. In this context, implant selection was based on both geometric requirements and potential material characteristics rather than any established superiority over conventional materials.
Soft tissue considerations were equally important. Severe contracture and scarring required extensive release to achieve adequate exposure and reduction, emphasizing the role of soft tissue balancing in complex reconstructions. Failure to address these factors can compromise implant positioning and functional outcome.
At most recent follow-up of approximately 7 months, the patient demonstrated progressive clinical improvement with reduction in pain and improvement in functional status compared to the preoperative condition. Serial laboratory values showed no evidence of recurrent infection, and radiographic evaluation demonstrated stable implant position without signs of loosening or failure. No additional surgical intervention was required during the follow-up period.
This case emphasizes the value of a multidisciplinary approach incorporating infection management, advanced imaging, and patient-specific implant design. Staged reconstruction combined with custom triflange fixation can provide a viable solution in cases of severe post-traumatic acetabular destruction complicated by infection.
Continued follow-up is necessary to further evaluate long-term implant durability and functional outcomes.
Conclusion
Complex post-traumatic acetabular defects with superimposed infection represent a significant reconstructive challenge. Staged management with infection control followed by patient-specific reconstruction can provide a viable solution when conventional options are not adequate. Custom triflange acetabular components, including those manufactured from advanced materials including PEKK, may represent a feasible reconstructive option in selected cases of severe bone loss and distorted anatomy. Further studies are required to evaluate long-term outcomes and define the role of PEKK in acetabular reconstruction.
Patient Perspective
The patient reported improvement in pain and mobility following the procedure and expressed satisfaction with the surgical outcome.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflict of Interest
Both authors serve as consultants for Oxford Performance Materials. No other conflicts of interest were reported.