Introduction
Orthopaedic injuries are common in rural and remote regions of the world. Individuals living in these areas experience higher rates and greater severity of orthopaedic injuries compared to their urban counterparts. This can lead to delayed diagnosis, delayed treatment, and poor clinical outcomes (Bang et al. 2019; Dixit et al. 2025; Lapointe et al. 2020; Malhotra 2019). Furthermore, limited numbers of orthopaedic specialists practice in rural areas which adds to the burden of orthopaedic injuries. In 2019, 39% of U.S. counties lacked orthopaedic specialists, with 82% of these counties being classified as rural (Hecht et al. 2023). Given the limited number of orthopaedic specialists in these areas, patients must travel great distances to receive basic orthopaedic care.
In rural areas of the United States, nurses, advanced practice providers, primary care physicians, and other medical professionals must attempt to fill the role of providing orthopaedic care. Telemedicine exists as a solution to this issue; however, it lacks the ability to provide real-time, first-person perspective for guidance and feedback during procedural scenarios.
Augmented Reality (AR) technology offers a unique solution to bridge the gap between telemedicine and providing orthopaedic care. AR allows the consulting orthopaedic specialist to view a clinical scenario through the treating medical professional’s perspective while providing real-time visual and audio feedback, enhancing the telemedicine experience and quality of care. AR technology has the potential to expand orthopaedic care to rural areas and improve the quality of essential orthopaedic procedures.
Few studies have evaluated the use of AR to support the delivery of orthopaedic care in rural communities. The objective of this pilot randomized simulation study was to evaluate the feasibility of AR technology to improve procedural execution among novice medical learners performing orthopaedic procedures for the first time. Furthermore, this study also sought to evaluate the reliability of an off-grid application setup of AR technology to better facilitate care in rural locations. We hypothesized that participants receiving AR guidance from a board-certified orthopaedic surgeon would demonstrate superior procedural accuracy compared with participants receiving AI generated instruction alone. We assessed the ability of AR technology to guide novice medical learners, without specialized orthopaedic training, to perform a series of orthopaedic tasks that are commonly encountered in the emergency department, inpatient, and outpatient settings.
Methods
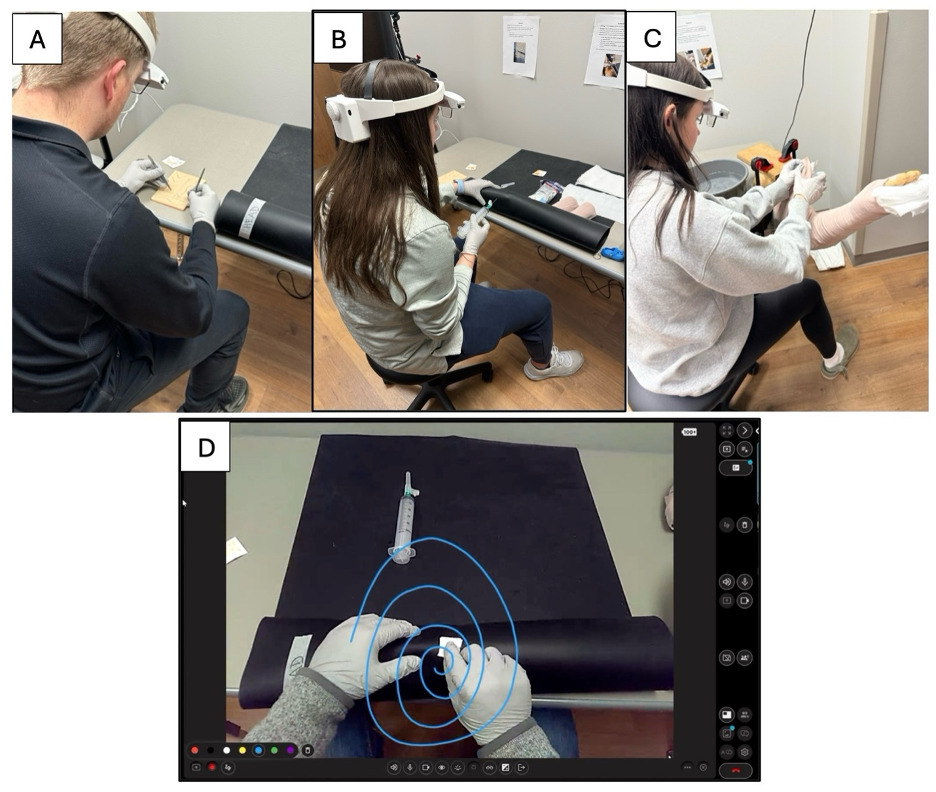
This study was conducted as a pilot randomized simulation trial. Twenty-four first-year medical students, with no prior experience performing orthopaedic procedural tasks, were enrolled. The medical students were randomized into an AR-assisted study group (n=12) and control group (n=12). Both groups were instructed to perform three simulated procedural tasks; (1) suture removal in an outpatient clinical setting, (2) knee joint aspiration on an inpatient unit and (3) application of a left arm posterior slab splint in an emergency department (Figure 1A-C). These three specific tasks were selected for this study as they are commonly encountered by medical professionals in our rural health system.
_study_participant_with_ar_headset_completing_procedural_steps_during_suture_removal_tas.png)
For all participants, each station was equipped with an artificial-intelligence (AI) prompt with background information, a single picture describing the scenario, and the goals for each task. The AI prompts were generated by Google Gemini (Gemini 2.5 Flash) and queried by the author group based on common search prompts that would be used by medical professionals without prior experience with these procedures; “How to remove surgical sutures?”, “How to aspirate a knee?”, and “How to place a long arm splint?”
The study group received real-time procedural instruction and guidance from a board-certified orthopaedic surgeon (NWS). This surgeon was located 20 miles off-site and viewed the scenarios on a laptop computer. The study participants connected to the laptop via an AR headset powered by a solar charged battery (Ecoflow, San Francisco, California) and connected over a satellite internet connection (SpaceX, Starlink) to create the “off grid” platform. The participating surgeon provided live annotations and verbal instructions to the study group throughout each task via the TeleAssist AR interface through the AR headset (ARSpectra, Luxembourg).
The control group wore the same AR headset for standardization and were instructed to utilize the AI generated prompts alone for procedural guidance. All participants were recorded performing each task and were later reviewed by co-investigators for data collection. Participants were assessed based on binary (yes/no) completion of pre-defined critical procedural steps for each task, as well as time-to-task completion. The procedural steps were defined by an orthopaedic surgeon familiar with these procedures as well as their application in rural health care. Failure to complete one or more procedural steps would result in unsuccessful completion of the entire task.
The number of annotations marked by the participating surgeon was recorded for each participant in the study group (Figure 1D). A single annotation was defined as (1) marking an area of interest (e.g. line, circle, arrow) or (2) illustrating a concept (e.g., drawing a specific suture type and marking it with an “X” illustrating where to cut). Following completion of the study, participants in the AR-assisted group completed a brief survey assessing their experience using the ARSpectra headset and system. The survey included questions related to usability and functionality, user experience, as well as potential impacts and benefits.
Suture Removal Task
A silicone suture mat was prepared with five different types of nylon sutures in a random order. The random order was chosen to determine if the off-site board-certified orthopaedic surgeon could identify the suture types during procedural guidance through the video feed. The nylon sutures consisted of one simple interrupted, one horizontal mattress, one vertical mattress and two arthroscopy sutures. One subcutaneous Prolene and one subcutaneous Monocryl suture spanning approximately two inches in length with free tails on both ends were also prepared. Time-to-task completion was recorded from the first purposeful action to the removal of the final suture. Binary data of critical step completion were recorded as follows:
-
Sterile technique: cleaning sutures with an alcohol pad prior to removal.
-
Nylon suture removal: proper technique consisting of grasping suture knot with forceps and cutting suture just below the knot, pulling suture across wound to remove it.
-
Prolene suture removal: cutting one tail and removing the remaining suture in one motion.
-
Monocryl suture removal: cutting both suture tails at skin level and leaving the remaining suture in place.
-
Completed all suture removals: removed all types of sutures with acceptable techniques.
Knee Joint Aspiration Task
An anatomic right adult knee model with a balloon filled with 50 mL of water was used to simulate an infected knee joint effusion. The construct was covered with a black silicone mat to mimic skin and simulate anatomic accuracy of an adult knee.
Time-to-task completion was recorded from the first purposeful action (i.e. grasping the alcohol pad or knee palpation) to handing off the syringe to a co-investigator as the final step. The following variables were recorded as follows:
-
Number of attempts: Each needle insertion and withdrawal.
-
Aspiration volume: Total volume of aspirated fluid.
-
Sterile technique: Use of an alcohol pad to clean area of interest.
-
No-touch technique: maintain sterility after skin preparation with the alcohol pad.
-
Landmark Verification: Correctly palpated the medial, lateral, and superior joint aspects.
-
Joint Access: Aspiration of any amount of fluid.
-
Needle redirection: Needle adjustment required for fluid aspiration.
-
Safe syringe handling: Appropriately capped the needle before hand-off to a co-investigator.
Application of Posterior Slab Splint Task
An adult left arm model (Sawbones, Seattle, WA) positioned at 90 degrees was used to simulate a supine patient. Materials provided to each participant included pre-cut soft roll, a single layer of soft roll to complete the opposite side of the splint, a 4-inch x 3-foot roll of fiberglass casting material, a water bucket for fiberglass activation, two ace-wraps, and tape to secure the final construct.
Time-to-task completion was measured from the first purposeful movement to the placement of the last piece of securing tape. Binary data were collected as follows:
-
Comprehensive skin assessment: 360-degree skin assessment of arm to assess for open fracture.
-
Soft roll placement: Correct sandwiching of fiberglass with soft roll.
-
Distal MCP coverage: Ensuring fiberglass extended to metacarpophalangeal (MCP) joints.
-
Proximal soft roll length: Correct placement relative to anatomical landmarks.
-
Cuff margin: Maintenance of a minimum one-inch cuff on soft-roll before fiberglass application for patient comfortability.
-
Layering of fiberglass: Appropriate multi-layer construction.
-
Correct plaster length: Measured independently or matched to pre-cut roll, maintaining a cuff.
-
A whole roll of fiberglass was used.
-
Fiberglass activation: Dipping fiberglass in water.
-
Soft roll application: Correct placement of thicker, soft roll on the patient’s skin.
-
Splint security: Use of ace-wrap for splint-stabilization.
-
Successfully completed all steps of splint.
Data was analyzed using Mann-Whitney-U test for non-binary outcomes such as time-to-task completion, fluid aspiration volume and number of attempts for the knee aspiration task. Fisher’s exact test was used for binary outcomes due to the small sample size and low expected cell counts. Confidence intervals were calculated for key findings using the Wilson method due to our small sample size. Statistical significance was set at a p-value of 0.05.
Results
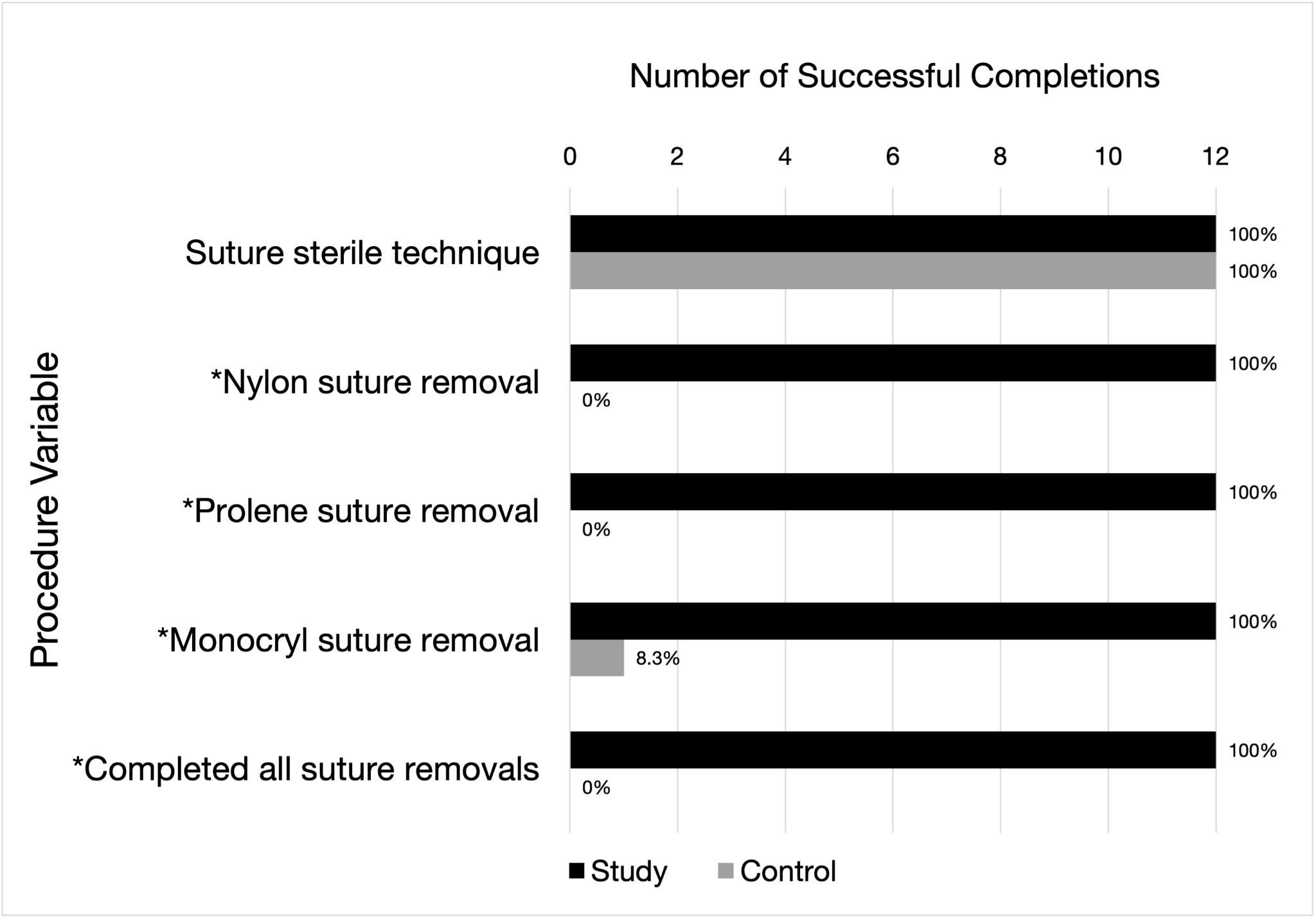
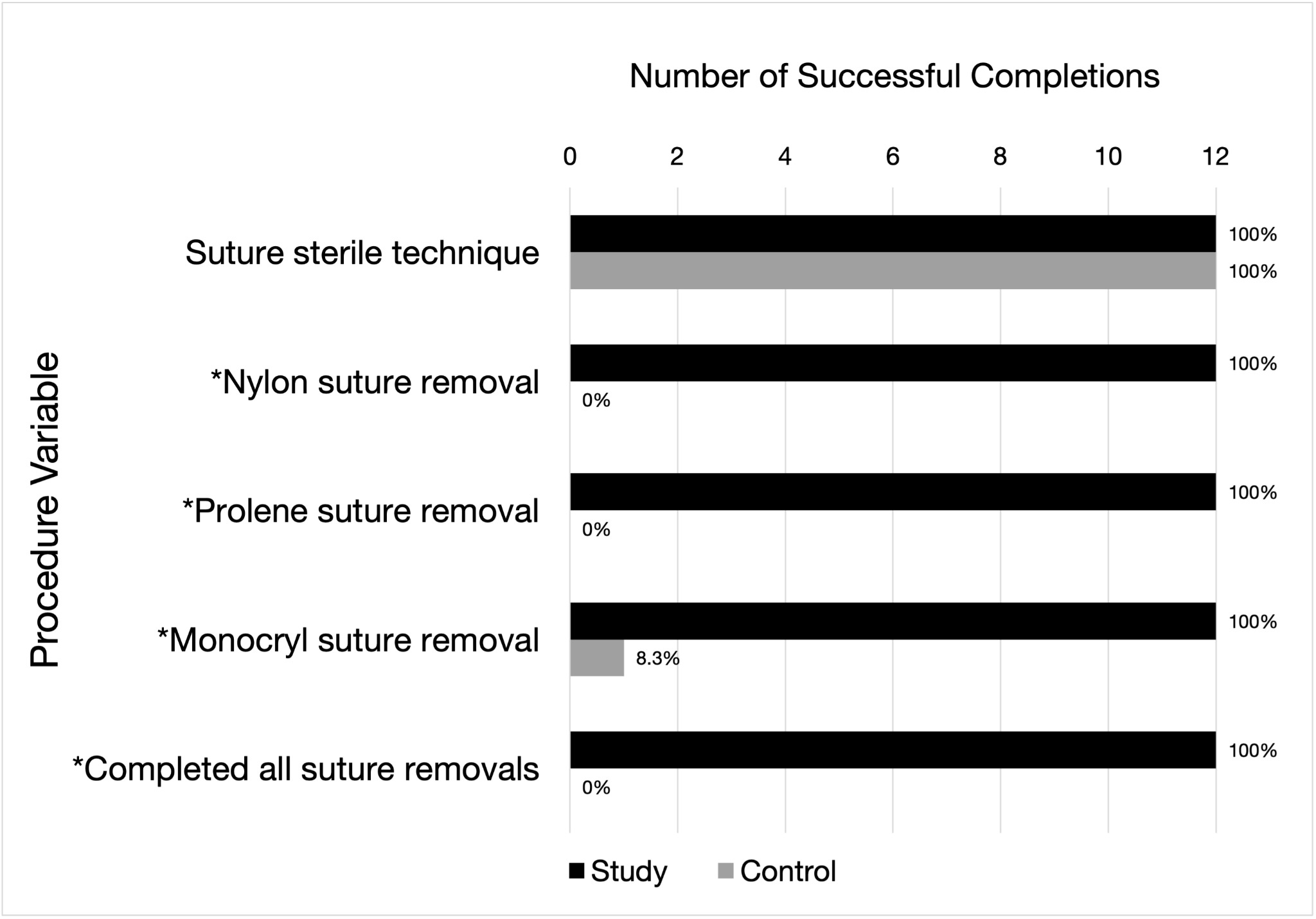
Participants in the AR-assisted study group demonstrated significantly higher procedural success rates across all three tasks. In the suture removal task, each study group participant identified and removed all nylon, Prolene and Monocryl sutures in the correct fashion, thereby successfully completing the entire task (100% [95% CI:73-100%]) compared to zero such instances (0% [95% CI: 0-24%]) in the control group (Figure 2). While participants in the control group ultimately removed each type of suture, all participants did so without adhering to proper technique and principles, resulting in failure to complete the suture removal task. Time-to-task completion for the suture removal task was not significantly different between groups, with the study group completing the task in an average time of 3.69 minutes and the control group completing the task in 4.14 minutes (p=0.166) (Table 1).
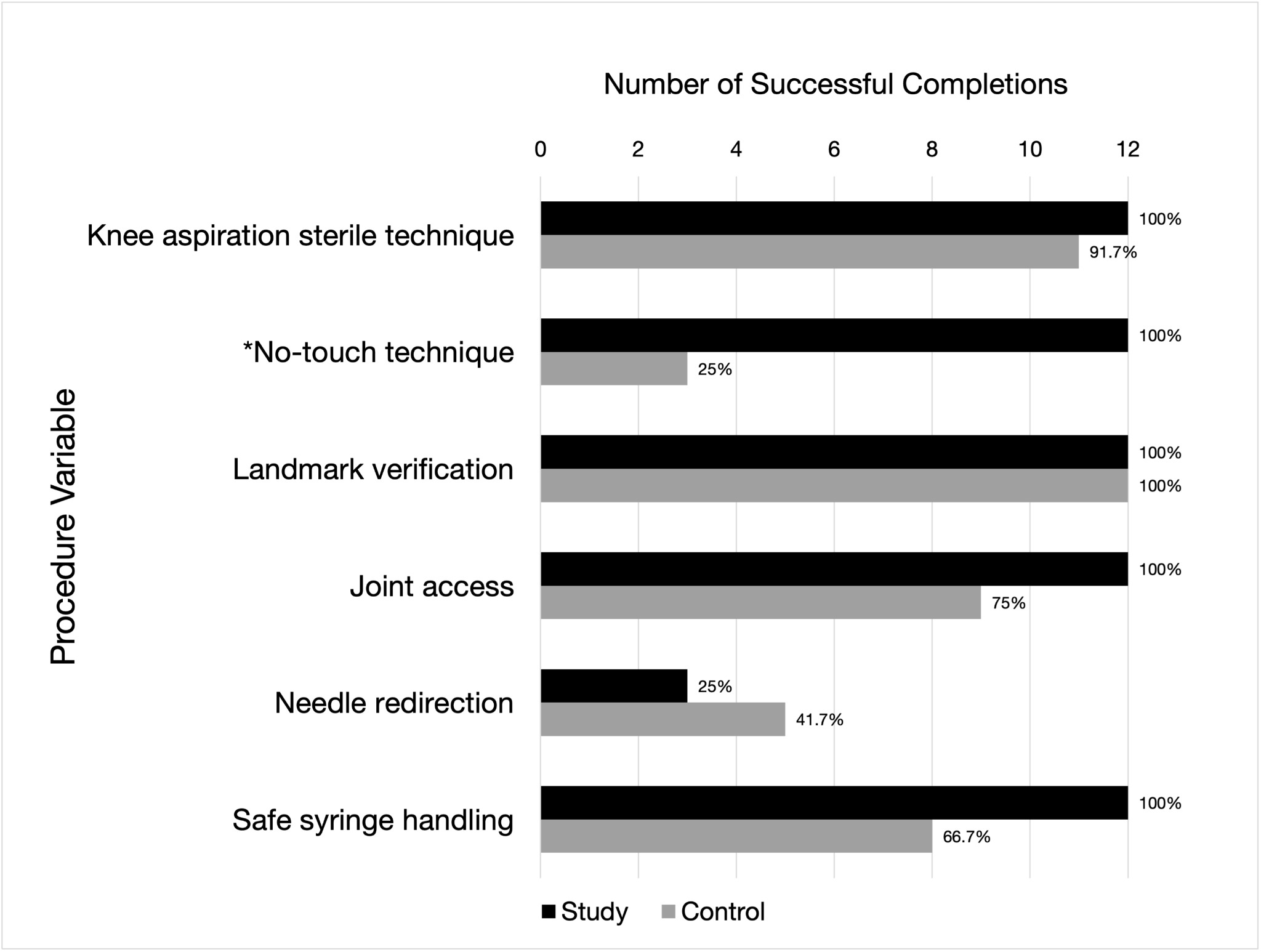
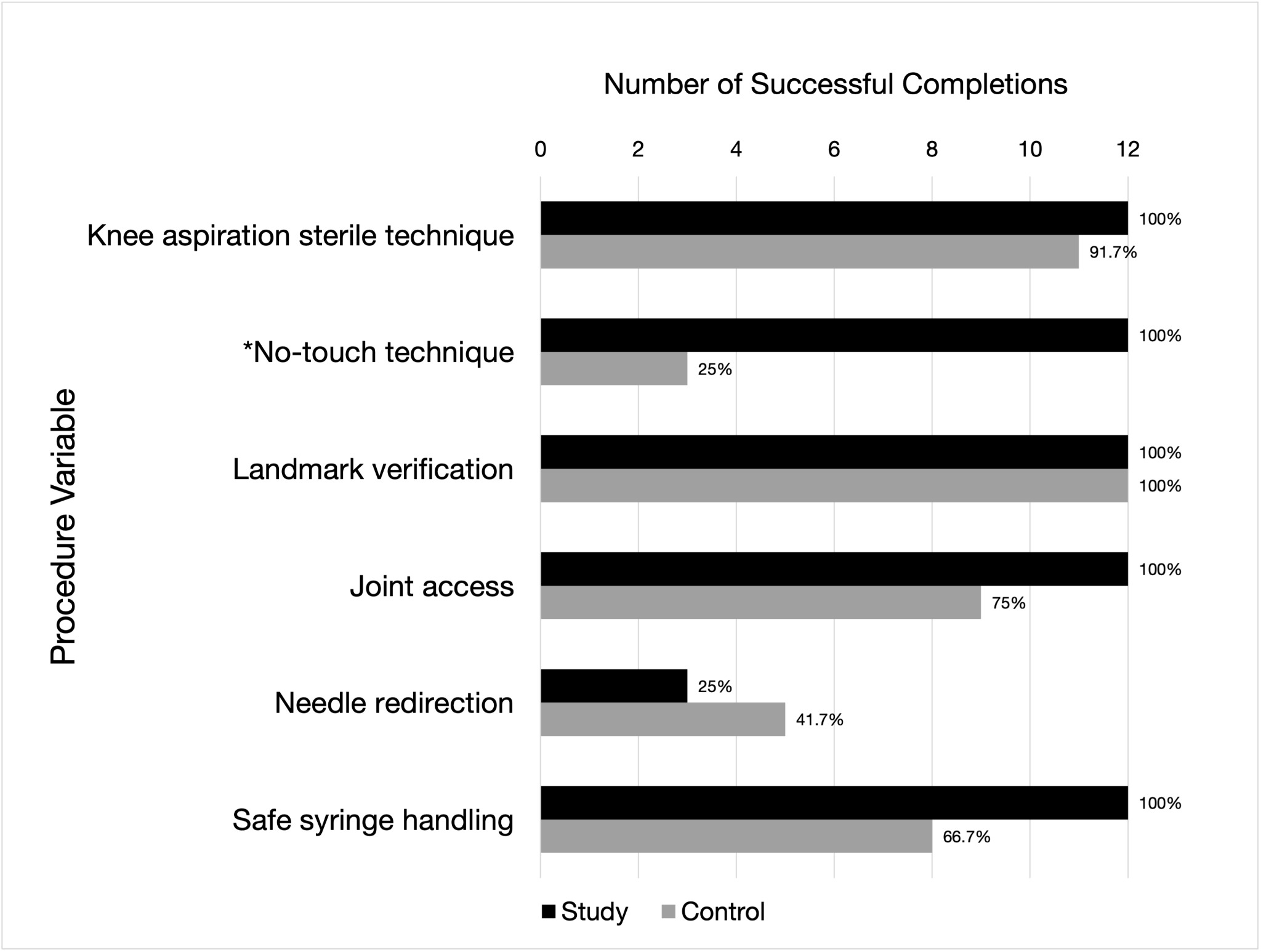
For the knee aspiration task, the study group demonstrated greater adherence to a sterile, no-touch technique (100% [95% CI:73-100%]) compared to the control group (25% [95% CI: 9-53%]) (p<0.01), however, there were no other statistically significant findings between the study and control group for the binary, procedural-step data points (Figure 3). The study group aspirated a greater mean amount of fluid (41.67 mL [95% CI: 33.69-49.65%]) compared to the control group (12.67 mL [95% CI: 8.73-29.43%]) with a p-value < 0.01. The mean time-to-task completion was significantly longer for the study group at 4.18 minutes compared to 2.35 minutes in the control group (p < 0.01) (Table 1). The mean number of attempts to access the knee joint did not demonstrate significant variation between each group.
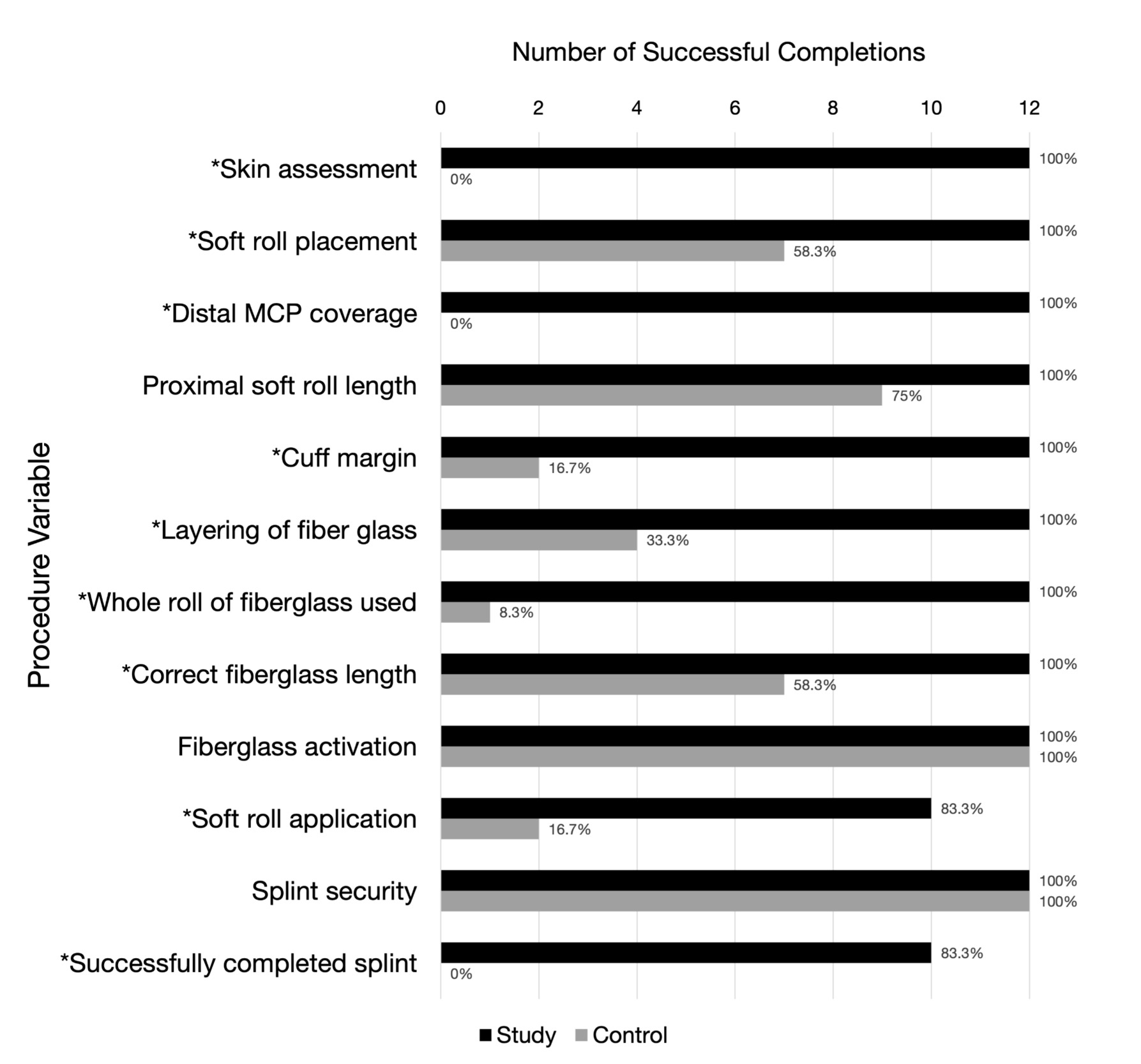
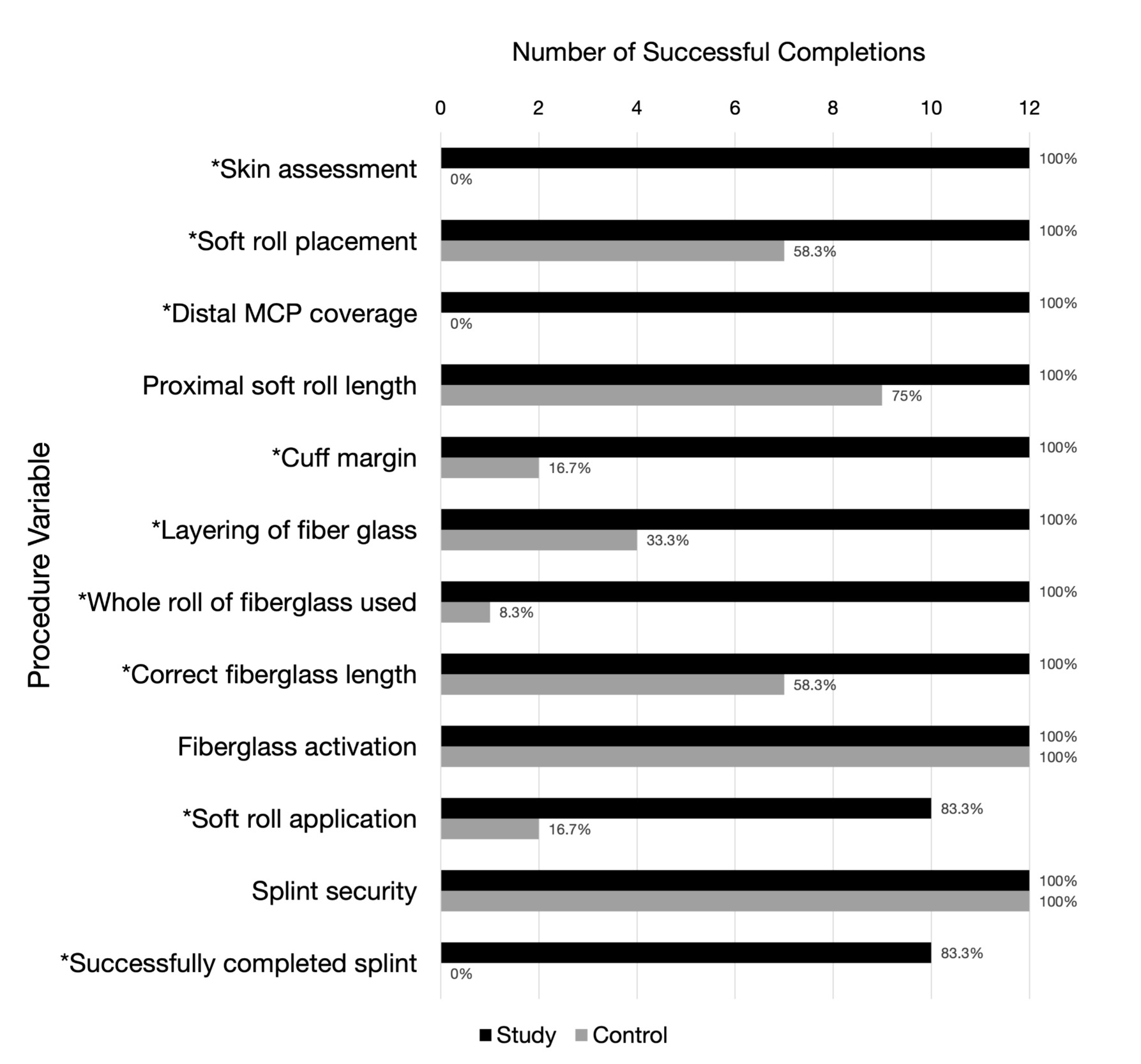
The study group demonstrated superior performance in several critical steps for the left arm posterior slab splint. The number of successfully completed steps was significantly greater in the study group with regard to skin assessment, distal MCP coverage, cuff margin, layering of fiberglass, whole roll of fiberglass used, correct fiberglass length, soft roll application, and overall correct completion of the splint (83.3% [95% CI: 55-95%] vs 0% [95% CI: 0-24%]) (Figure 4). The mean splint completion time for the study group (7.49 minutes) was longer than the control group (4.46 minutes), with a p-value of <0.01 (Table 1).
The number of annotations used by the participating surgeon varied between each task. The knee aspiration task required a mean of 8 annotations (SD = 2.17) to complete the task, while the splint task required a mean of 11 annotations (SD = 2.63). The suture task required a mean of 9.08 annotations (SD = 1.73).
In the post-study survey, the AR-assisted study group reported the AR technology was easy to use (mean score 8.25), and the headset was comfortable to wear (mean score, 8). Participants also reported the instructions and guidance provided was sufficient for them to effectively utilize the AR technology. The AR technology was perceived to be highly intuitive, effective in teaching and providing guidance, with participants noting enhanced understanding and engagement with the procedures. Based on this experience, participants also reported they would consider using this AR technology in a real-world patient care scenario (Table 2).
Discussion
Our study demonstrated that remote AR guidance by an orthopaedic specialist significantly improved procedural performance and accuracy for the AR-assisted study group in all three simulated orthopaedic tasks compared to the control group. Most notably, the AR-assisted feedback and guidance by the remote orthopaedic surgeon enabled all participants in the study group to successfully navigate and complete each procedural task in a stepwise and organized fashion with accurate results. No issues related to internet connection, hardware, or software interface were encountered in the AR-assisted study group.
Although improved overall performance was observed in the AR-assisted study group, more time on average was required for completion in both the knee aspiration (4.18 vs. 2.35 minutes) and posterior slab splint (7.49 vs 4.46 minutes) tasks when compared to the control group. This may be explained by the additional time for deliberate instruction, annotations, and guidance provided by the orthopaedic surgeon to ensure proper and accurate technique for the study participants. These findings may also be due to increased cognitive load associated with the AR interface and from the learning curve required to effectively utilize the AR technology. However, usability data from the survey completed by the AR-assisted study group indicates this finding is unlikely due to difficulty using the AR interface. Study participants reported the AR headset and interface to be easy to use (mean score 8.25/10) and highly intuitive (mean score 8.17/10), suggesting the longer completion times may reflect careful instruction rather than increased cognitive burden associated with the AR system. This finding supports other AR-based studies that have also reported increased accuracy and reduced errors in AR-assisted groups despite longer times for task completion (Follmann et al. 2019; Rojas-Muñoz et al. 2019).
Overall, our study findings add to the growing body of literature supporting the feasibility and efficacy of AR as a telemedicine tool to help support medical interventions and enhance medical education (Dinh et al. 2023). Although to our knowledge, no studies have explored the application of AR as a method to assist and provide rural-based medical professionals with the skills necessary to complete orthopaedic procedures via satellite internet connection. After our study assessment, we surveyed the study participants about their experience using the headset and AR-technology. The survey respondents replied on a scale of 0-10 that the AR platform was “very effective” (mean score 9.2/10) at teaching and providing guidance while performing the medical procedure. They also reported the AR technology was “very effective” (mean score 9.1/10) at enhancing their understanding and engagement with the study procedures.
Specialized orthopaedic care is limited in rural areas. Rural clinicians often assume the initial role of evaluating and treating patients with orthopaedic injuries. Conventional telemedicine methods, such as videoconference or phone consults, can help guide management when treating orthopaedic injuries, however, these methods are less helpful for providing direct “hands-on” guidance. As evidenced by the results of this study, AR-assisted guidance can bridge this gap by offering first-person perspective instruction and feedback through audiovisual communication and annotations that traditional telemedicine lacks. The high-performance results of the novice AR-assisted study group should instill confidence for rural clinicians that AR guidance can serve to overcome limited prior orthopaedic procedural experience to obtain successful procedural outcomes.
Along with limited access to specialized orthopaedic care, rural areas also face unreliable internet connectivity that is essential for providing remote healthcare services. Conventional telemedicine platforms in rural healthcare systems depend heavily on stable broadband connections, yet many rural hospitals continue to lack high-speed internet infrastructure or broadband services (Maita et al. 2024). Implementation of satellite internet offers a potential solution to improve internet connectivity barriers for rural hospitals. In our study, we successfully incorporated off-grid satellite internet connection (SpaceX, Starlink) which was utilized by the participating orthopaedic specialist located in a remote off-site location. The orthopaedic specialist provided instructions via the AR TeleAssist interface to the study participants without delays or interruptions in connectivity during the entirety of our study. Similarly, the video quality was sufficient for him to identify details such as suture patterns, colors, and splint padding length. Five study participants reported brief technical issues in the post-study survey, specifically brief loss of the heads-up display that resolved spontaneously. No connection was lost during these episodes. Our integration of satellite internet connectivity supporting the use of AR offers a blueprint for rural healthcare systems without sufficient internet infrastructure or telehealth systems. However, aspects such as data security, complex installation, and high costs serve as potential barriers for implementation.
There are several other limitations to this study. First, the sample size was small and consisted of 24 first-year medical students from a single university, which may not be representative of practicing rural clinicians, thereby limiting generalizability. Second, this study focused on simulation-based tasks to imitate real-world clinical scenarios. Therefore, this study is limited in assessing how AR technology affects real-world patient care and outcomes. Third, the orthopaedic tasks were basic in nature which warrants further assessment of AR technology as a tool for assisting more complex procedures. The three procedural tasks were selected based on real-world scenarios that are frequently encountered in rural health systems; however, these specific scenarios have not undergone formal external validation. While the scoring criteria were developed by experienced clinicians to ensure alignment with current standards of care, further validation studies may strengthen reproducibility.
Finally, the control group was limited to AI generated prompts alone. They did not have access to additional support material such as textbooks, videos, or standardized protocols that clinicians could use when performing unfamiliar procedures for the first time. In some situations, clinicians have a knowledge gap in understanding or may not know that they are performing a procedure incorrectly. This discrepancy in information presented may have favored the AR assisted group. The control group was limited in the resources they could access to address their knowledge deficit. This limitation did not completely replicate real-world practice of a novice clinician.
This study should be viewed as a proof-of-concept investigation that highlights the potential of AR to assist and enhance orthopaedic interactions and procedures. The study was designed to replicate real-world clinical scenarios that our health system encounters with rural clinics. Further studies with larger sample sizes and more detailed methodology will be necessary before this technology can be used widespread in clinical applications.
Future studies should be performed to better understand the longitudinal implications of AR technology as a tool to enhance patient care in a rural health setting, seeking to compare retention rates, learning curves, and outcomes. Furthermore, future research should incorporate practicing rural clinicians as study participants to better understand the capabilities of AR as a support tool in rural health care. In conclusion, AR technology demonstrates substantial potential as an adjunct to rural telemedicine for the purposes of guiding clinicians through the process of completing orthopaedic procedural tasks.