Introduction
Peptide therapies have rapidly entered mainstream musculoskeletal culture, driven by social media promotion, direct-to-consumer wellness and optimization clinics, and the expanding commercialization of biologic optimization (Vasireddi et al. 2025). Compounds such as BPC-157 and thymosin beta-4 derivatives, commonly marketed as TB-500, are increasingly used by athletes and patients seeking accelerated recovery from tendon injury, ligament reconstruction, cartilage pathology, and postoperative rehabilitation (Vasireddi et al. 2025; Mayfield et al. 2026). Despite widespread adoption, these agents are not approved by the U.S. Food and Drug Administration (FDA) for musculoskeletal indications, and the evidence supporting clinical efficacy is limited. Recent orthopaedic literature has emphasized that clinical exposure to BPC-157 has expanded far more rapidly than scientific validation, with published studies overwhelmingly consisting of preclinical models and only sparse human data (Vasireddi et al. 2025; Mayfield et al. 2026; Matek et al. 2026).
The implications of this trend extend beyond sports medicine. Orthopaedic surgery is uniquely sensitive to small shifts in perioperative risk, particularly in implant-based procedures where complications carry disproportionate consequences. In total joint arthroplasty (TJA), wound complications, hematoma formation, and delayed drainage substantially increase susceptibility to periprosthetic joint infection (PJI), an outcome associated with revision surgery, prolonged antimicrobial therapy, and durable functional decline (Xiong et al. 2025; Almeida et al. 2021). In this context, even modest alterations in angiogenesis, inflammatory signaling, or coagulation balance, as well as contamination exposure, may be clinically meaningful. Unlike conventional supplements, many peptides are administered through subcutaneous or intramuscular injection, often obtained through nonregulated sources with uncertain sterility, concentration accuracy, and compositional reliability (Wang et al. 2022). Product integrity may therefore represent a dominant perioperative concern independent of pharmacologic effect.
The scientific literature describing BPC-157 and thymosin beta-4 has proposed mechanistic effects on angiogenesis, inflammatory signaling, fibroblast migration, and collagen remodeling (Vasireddi et al. 2025; Mayfield et al. 2026). Other peptide agents such as GHK-Cu are marketed for wound healing and connective tissue repair, while growth hormone secretagogues and IGF-1 analogs are increasingly used in performance settings and may plausibly influence recovery physiology through systemic endocrine pathways (Pickart and Margolina 2018). However, the available data remain heterogeneous, frequently reliant on surrogate endpoints, and rarely tested in clinical settings reflective of orthopaedic surgical care (Rahman et al. 2026). Existing reviews have further highlighted that pharmacokinetic and safety characterization in humans remains incomplete, complicating clinical counseling regarding timing of discontinuation, perioperative risk stratification, and postoperative resumption (Rahman et al. 2026).
As patient use accelerates, orthopaedic surgeons are increasingly asked to counsel individuals who view peptide exposure as responsible health optimization. The absence of clinical guidelines leaves surgeons navigating an evidence gap with potential medicolegal implications, particularly when patients undergo elective procedures where the acceptable tolerance for unmeasured risk is low. Therefore, the purpose of this scoping review is to characterize the current evidence base for peptide therapies relevant to musculoskeletal care, with emphasis on BPC-157, thymosin beta-4 derivatives, and related agents, and to define safety considerations and perioperative implications for orthopaedic surgical patients, including those undergoing TJA.
Materials and Methods
Study Design
A scoping review was performed to map the available evidence regarding peptide therapies relevant to musculoskeletal care, including agents not approved for musculoskeletal indications and orthopaedic surgery. A scoping approach was selected given the anticipated heterogeneity of study designs, the predominance of preclinical literature, and the limited volume of human clinical outcome data. Reporting followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) where applicable, with emphasis on transparent identification of available evidence rather than quantitative pooling.
Search Strategy
A comprehensive search of PubMed/MEDLINE and the Cochrane Central Register of Controlled Trials (CENTRAL) was performed from database inception through the final search date. ClinicalTrials.gov was queried to identify registered or ongoing trials. Search terms combined peptide agent names with musculoskeletal and perioperative keywords and included BPC-157, body protection compound, pentadecapeptide, thymosin beta-4, TB-500, TB500, GHK-Cu, copper tripeptide, growth hormone secretagogue, CJC-1295, ipamorelin, sermorelin, IGF-1, insulin-like growth factor, collagen peptide, tendon, ligament, cartilage, osteoarthritis, fracture healing, wound healing, perioperative, arthroplasty, total hip arthroplasty, total knee arthroplasty, and total joint arthroplasty. Reference lists of included articles and relevant reviews were manually screened to identify additional pertinent studies.
Study Identification and Selection Approach
The initial search yielded a large body of literature across peptide agents and clinical domains. After removal of clearly nonrelevant records based on title and abstract screening, approximately 40 to 70 studies were identified as potentially relevant to musculoskeletal biology, orthopaedic care, or perioperative considerations. Full-text review was subsequently performed, with approximately 20 to 35 studies informing the final narrative synthesis.
Screening was performed by the authors with an emphasis on translational relevance to orthopaedic surgery and perioperative decision-making. Given the scoping nature of the review and the heterogeneity of available evidence, study selection focused on identifying representative and clinically informative literature rather than exhaustive quantitative inclusion. Discrepancies in study relevance were resolved by consensus.
Eligibility Criteria
Studies were eligible if they evaluated BPC-157, thymosin beta-4 or marketed derivatives (including TB-500), GHK-Cu, or other peptide-based agents commonly promoted for musculoskeletal healing or recovery and reported outcomes relevant to musculoskeletal pathology, orthopaedic surgery, postoperative recovery, or perioperative risk domains. Preclinical animal studies, in vitro mechanistic investigations, and human clinical studies were eligible. Human evidence included randomized trials, cohort studies, case-control studies, case series, and case reports. Studies focused exclusively on non-musculoskeletal indications without clear translational relevance were excluded. Non-English publications were excluded if full-text translation was not available.
Data Extraction
Extracted variables included study design, peptide agent and formulation, dosing regimen and route of administration when reported, musculoskeletal indication, comparator group, outcome measures, efficacy findings, and adverse events. Mechanistic endpoints were recorded when available, including markers of inflammation, angiogenic activity, collagen organization, and bone remodeling. Human clinical evidence was prioritized for synthesis, with preclinical evidence used to contextualize biologic plausibility. Data extraction and synthesis were performed iteratively, with emphasis on clinical relevance and perioperative applicability.
Evidence Synthesis
Given heterogeneity in models, dosing, and outcome reporting, findings were summarized using structured narrative synthesis rather than quantitative pooling. Evidence was grouped by peptide agent and clinical domain, including tendon and ligament healing, cartilage and osteoarthritis, bone remodeling and fracture repair, wound healing, and postoperative recovery. Perioperative implications were evaluated with emphasis on orthopaedic surgical risk domains relevant to total joint arthroplasty (TJA), including wound complications, hematoma formation, immune modulation, infection susceptibility, heterotopic ossification, and implant fixation considerations. Commonly encountered agents were summarized by proposed mechanism, evidence tier, and perioperative considerations (Table 1).
Results
Search Results and Study Characteristics
The search identified a broad and heterogeneous body of literature spanning multiple peptide agents and a wide range of non-orthopaedic indications. Following relevance-based screening, approximately 20 to 35 studies were included in the final narrative synthesis. Consistent with the intent of an evidence-mapping scoping review, studies were selected based on translational relevance to musculoskeletal tissue healing, orthopaedic care, and perioperative decision-making. The evidence base was dominated by preclinical animal and mechanistic investigations, while human clinical outcome data were limited and largely observational. Across included studies, substantial variability existed in peptide formulation, dosing strategy, route of administration, and outcome reporting, limiting comparability and precluding quantitative synthesis.
BPC-157
BPC-157 was the most frequently represented peptide agent in musculoskeletal research. Preclinical studies have described effects on tendon healing, ligament repair, muscle regeneration, and inflammatory modulation (Vasireddi et al. 2025; Rahman et al. 2026). Multiple experimental models reported improved collagen organization, enhanced tensile strength, and pro-angiogenic signaling following injury. However, these findings were derived from heterogeneous models with inconsistent dosing regimens and variable outcome definitions (Cerovecki et al. 2010; Staresinic et al. 2003; Barisic et al. 2022). Few investigations incorporated clinically relevant comparators, standardized rehabilitation conditions, or endpoints directly translatable to postoperative recovery. Human evidence remains sparse, and no high-quality trials were identified evaluating BPC-157 in orthopaedic surgical populations. The current evidence base therefore does not support conclusions regarding efficacy in postoperative recovery or complication reduction. The limited available human clinical evidence evaluating BPC-157 and related peptide therapies in musculoskeletal settings is summarized in Table 2.
Thymosin Beta-4 and TB-500
Thymosin beta-4 has been investigated in a smaller but mechanistically consistent body of literature, with reported effects on angiogenesis, cell migration, cytoskeletal regulation, and inflammatory signaling (Gonzalez-Franquesa et al. 2021; Goldstein et al. 2012; Philp et al. 2004; Yarmola et al. 2007). These pathways have contributed to widespread marketing of TB-500 as a recovery-enhancing therapy (Gonzalez-Franquesa et al. 2021; Goldstein et al. 2012; Philp et al. 2004; Yarmola et al. 2007). However, evidence directly applicable to musculoskeletal clinical outcomes remains limited. Most available data are preclinical or derived from non-orthopaedic clinical contexts, and robust human orthopaedic trials were not identified. In addition, TB-500 represents a marketed formulation rather than a standardized pharmaceutical product, introducing uncertainty regarding composition, dosing equivalence, and biologic predictability (Rahman et al. 2026). As a result, translation to surgical recovery and perioperative decision-making remains unsupported by high-quality clinical evidence.
GHK-Cu
GHK-Cu is marketed for wound healing and connective tissue repair and has been described in mechanistic and dermatologic literature suggesting potential effects on collagen synthesis and extracellular matrix remodeling (Wang et al. 2017; Pickart 2008). While these pathways are theoretically relevant to soft-tissue recovery, orthopaedic-specific evidence remains minimal. No studies were identified evaluating GHK-Cu exposure in patients undergoing TJA or other major orthopaedic procedures. Accordingly, any inference regarding clinical benefit or perioperative risk is speculative.
Growth Hormone Secretagogues and IGF-1 Analogs
Growth hormone secretagogues, including CJC-1295, ipamorelin, and sermorelin, and IGF-1 analogs are increasingly used in wellness and optimization settings and are frequently co-administered with BPC-157 or TB-500 (Rahman et al. 2026). These agents are mechanistically distinct from tissue-targeted peptides and may influence recovery physiology through systemic endocrine pathways (Clemmons et al. 2017; Falutz et al. 2010; Raun et al. 1998; Stanley et al. 2014; Beck et al. 2014; Teichman et al. 2006). However, orthopaedic-specific clinical evidence supporting improved healing or postoperative recovery is lacking. In contrast, potential perioperative relevance may relate to metabolic instability, including glycemic effects, fluid retention, and blood pressure variability, particularly in older or comorbid surgical populations. The absence of surgical outcome data limits risk quantification, but the systemic endocrine activity of these agents warrants heightened perioperative caution. Regulatory and governance considerations relevant to orthopaedic patients, including athletes, are summarized in Table 3.
Perioperative and Arthroplasty-Specific Implications
Across all peptide categories, direct evidence evaluating perioperative outcomes was limited. No high-quality studies were identified assessing the impact of peptide exposure on wound complications, hematoma formation, infection rates, or implant outcomes following TJA. Nevertheless, pathways implicated in preclinical studies, including angiogenesis, inflammatory modulation, and collagen remodeling, intersect with biologic systems central to incision healing and complication avoidance, although these mechanistic signals have not been shown to translate into improved clinical outcomes. In TJA, where the consequences of wound failure and PJI are severe, the absence of validated safety data is clinically meaningful. Furthermore, sourcing introduces uncertainty in sterility and formulation integrity, which may represent a more immediate and clinically relevant risk than theoretical biologic effects, particularly given the potential for nonsterile preparation, contamination, or inconsistent formulation in nonregulated injectable products. Key perioperative risk domains relevant to TJA and implant-based surgery potentially affected by peptide exposure are summarized in Table 4.
Discussion
Interpretation of the Current Evidence
The central finding of this review is the imbalance between clinical uptake and clinical evidence. BPC-157 and thymosin beta-4 derivatives are increasingly used for musculoskeletal recovery, yet the available literature remains dominated by preclinical models with minimal human validation (Vasireddi et al. 2025; Mayfield et al. 2026; Rahman et al. 2026). Across multiple experimental settings, these agents demonstrate biologic activity involving angiogenesis, inflammatory modulation, fibroblast migration, and collagen remodeling. These signals support biologic plausibility and justify further translational investigation, but do not establish clinical benefit. However, mechanistic plausibility does not establish clinical benefit, and the current evidence base does not support claims of improved healing, accelerated recovery, or reduced complication rates following orthopaedic surgery.
Safety, Product Integrity, and the Problem of Unregulated Supply
The primary clinical concern is not simply uncertainty regarding biologic effects, but uncertainty regarding product composition, sterility, and manufacturing quality. Most peptide products used in real-world settings are obtained through nonregulated sources with unclear manufacturing standards, variable concentration, and uncertain sterility. Injectable administration further magnifies this risk by introducing the possibility of local tissue reaction, systemic inflammatory exposure, and contamination-related complications. This distinction is critical, as even a biologically promising compound may become clinically harmful when delivered through nonstandardized formulations. The absence of verified pharmacokinetics and product verification prevents evidence-based recommendations regarding discontinuation timing, perioperative safety, and postoperative resumption, leaving surgeons unable to quantify risk in elective operative settings. This is particularly relevant for injectable formulations obtained outside standard pharmaceutical channels, where risks of contamination, endotoxin exposure, or improper compounding may exceed any theoretical biologic effect. Many of these agents are not approved by the FDA for musculoskeletal indications and may be compounded or sourced outside regulated pharmaceutical manufacturing pathways.
Implications for Total Joint Arthroplasty
TJA represents a uniquely high-stakes setting for peptide exposure. Even modest increases in hematoma formation, persistent drainage, or delayed wound healing may amplify susceptibility to PJI, a complication with disproportionate morbidity and resource utilization. Potential mechanisms by which peptide exposure could influence surgical outcomes include dysregulated angiogenesis contributing to hematoma formation, altered inflammatory signaling affecting early wound healing, and perturbations in collagen organization that may influence soft-tissue integrity during the critical postoperative period.
While direct evidence linking peptide use to PJI or implant failure is lacking, the absence of high-quality safety data should not be interpreted as reassurance. The combination of unverified formulation, uncertain sterility, and unknown systemic effects creates a perioperative exposure that cannot be reliably risk-stratified. In elective TJA, where tolerance for biologic uncertainty is low, the most defensible approach remains risk minimization. At the same time, if verified peptide formulations were ultimately shown to enhance soft-tissue recovery without increasing infection risk, the clinical relevance for TJA would be substantial, underscoring the importance of rigorous clinical investigation rather than informal adoption.
Adjacent Agents and Real-World Stacking Behavior
Patients using BPC-157 or TB-500 frequently engage in broader self-directed health or recovery strategies, often combining multiple agents with overlapping physiologic effects. GHK-Cu is marketed for wound healing and connective tissue remodeling, while endocrine-active compounds such as growth hormone secretagogues and IGF-1 analogs are used to augment recovery and performance (Pickart and Margolina 2018; Rahman et al. 2026). NAD, while not a peptide, is frequently administered in the same longevity settings and reflects the broader ecosystem of perioperative supplementation (Gallagher and Emmanuel 2026). This stacking behavior complicates medication reconciliation and increases uncertainty surrounding glycemic stability, fluid shifts, and inflammatory response. In practice, counseling is most effective when focused on defining the specific agent, route of administration, source reliability, and timing relative to surgery rather than debating unproven efficacy claims. It is important to distinguish orally administered supplements, such as collagen peptides, from injectable biologics, as oral formulations generally have a different safety profile and do not introduce risks related to sterility or injection-related complications.
Clinical Counseling and Perioperative Management
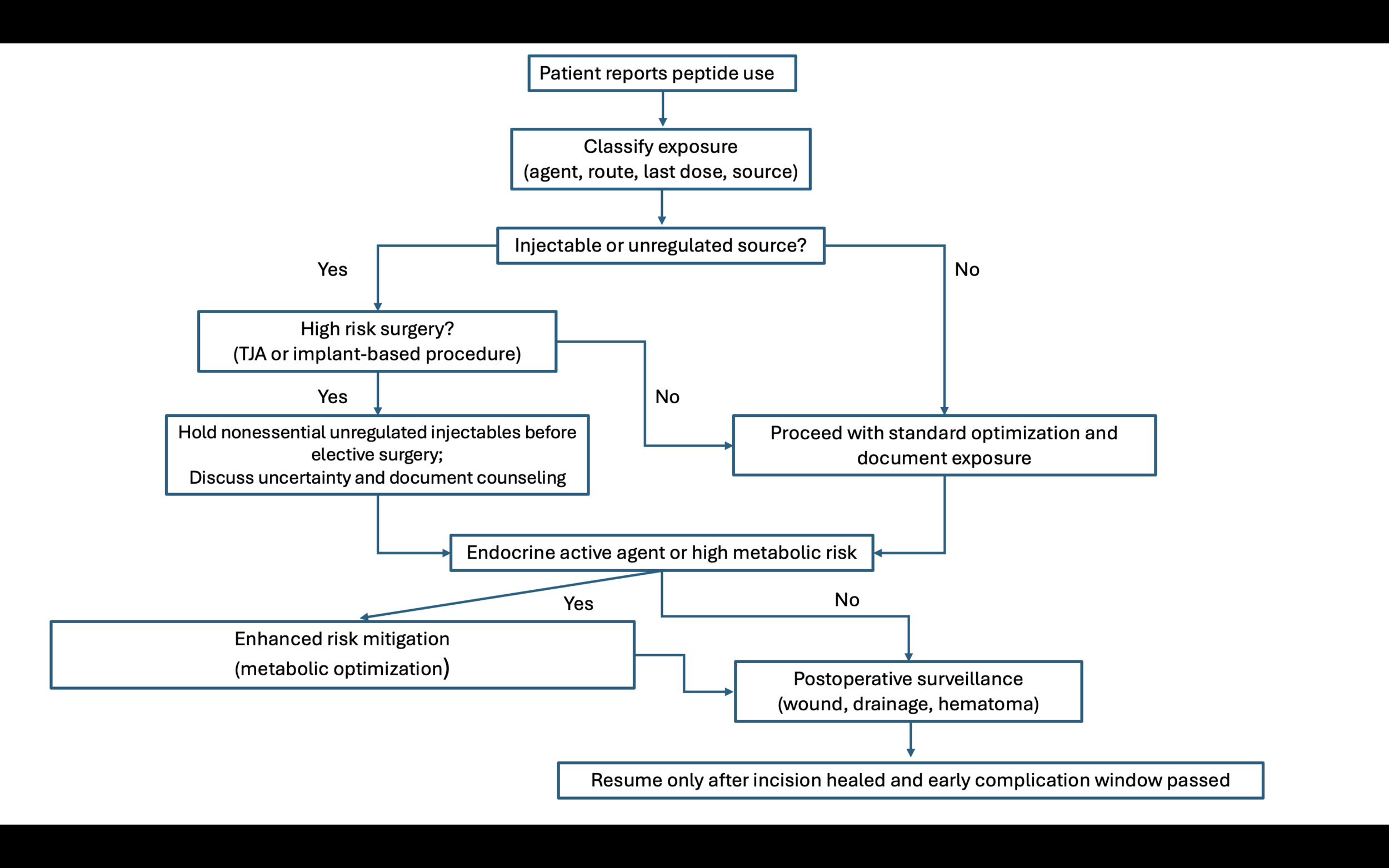
In the absence of validated efficacy and perioperative safety data, surgeons require a pragmatic framework. Patients should be counseled that current evidence supporting peptides is largely preclinical, that human surgical outcomes are poorly studied, and that product purity and sterility cannot be assumed. For procedures in which complications are catastrophic, including TJA, counseling should prioritize discontinuation of nonessential injectable biologics before surgery, explicit documentation of exposure, and heightened vigilance for early wound complications. These discussions should remain neutral and evidence-driven, recognizing that many patients interpret peptide use as proactive health optimization. A transparent explanation of evidence limitations and surgical risk priorities is more likely to preserve trust and compliance than confrontational dismissal. A pragmatic perioperative counseling and risk-minimization framework is proposed for orthopaedic surgical patients reporting peptide exposure (Figure 1).

Research Priorities and the Translational Opportunity
Despite limited clinical evidence, the biologic plausibility and widespread exposure base represent a translational opportunity for orthopaedics. Future investigations must prioritize product verification, dose characterization, and adverse event surveillance before efficacy can be responsibly evaluated. Prospective studies should incorporate clinically meaningful endpoints rather than surrogate mechanistic outcomes. For sports procedures, these include validated functional scores, return-to-sport timing, and complication surveillance. For TJA, priority endpoints include wound complications, prolonged drainage, hematoma requiring intervention, early readmission, and PJI, with follow-up sufficient to capture early revision risk. Without standardized formulations and defined perioperative protocols, clinical trials will remain vulnerable to confounding and irreproducibility.
Importantly, the current evidence gap should not be interpreted as evidence of ineffectiveness. Many therapies now considered foundational in perioperative medicine were initially adopted based on mechanistic plausibility and early observational signals before high-quality surgical outcome trials were performed. If standardized peptide formulations can be verified and administered within controlled protocols, these agents may represent a future adjunct to evidence-based perioperative care, particularly in populations undergoing TJA where wound healing, metabolic health, and inflammatory regulation strongly influence outcomes.
Future Direction and Call to Action
The current evidence gap presents an opportunity for orthopaedic investigators to establish high-quality prospective registries evaluating peptide exposure in real-world musculoskeletal populations. Systematic capture of dosing patterns, formulation source, route of administration, and standardized clinical outcomes may be more informative than continued reliance on heterogeneous mechanistic studies. In particular, elective procedures with high consequence complications, including TJA, warrant carefully designed observational cohorts with validated patient-reported outcomes, wound surveillance, and adverse event monitoring. Such registries, coupled with independent product verification and transparent conflict-of-interest disclosure, represent a critical step toward determining whether clinically meaningful benefit exists and whether perioperative risk can be quantified. Rather than allowing peptide use to remain confined to nonmedical distribution channels, orthopedics should lead the development of standardized perioperative registries and prospective trials using verified formulations, with the goal of determining whether peptide-based therapies can be safely integrated into evidence-based surgical optimization.
Limitations
This review is limited by the structure of the existing literature. Most studies evaluating BPC-157, thymosin beta-4 derivatives, and related peptide agents are preclinical, employ heterogeneous dosing regimens, and report surrogate endpoints that do not translate directly to operative recovery or implant-based outcomes. Human musculoskeletal evidence is sparse and rarely includes verified product composition, standardized exposure assessment, or perioperative endpoints relevant to TJA. In addition, real-world use is frequently confounded by co-administration of multiple agents and inconsistent sourcing, limiting external validity and complicating attribution of benefit or harm. Accordingly, conclusions should be interpreted as an evidence map and perioperative risk framework rather than confirmation of clinical efficacy or safety.
Conclusions
Peptide therapies are increasingly used among musculoskeletal patients, yet high-quality evidence supporting clinical efficacy and perioperative safety remains limited. Preclinical studies demonstrate biologic activity relevant to tissue repair, supporting biologic plausibility but not clinical effectiveness. The current combination of uncertain benefit and uncertain product integrity warrants a cautious and structured clinical approach. In total joint arthroplasty, where wound complications and periprosthetic joint infection carry substantial consequences, perioperative risk minimization should remain the priority. Future investigation using verified formulations and prospective clinical study designs is necessary to determine whether peptide-based therapies can be safely and meaningfully integrated into orthopedic care.