INTRODUCTION
Reverse shoulder arthroplasty (RSA) is an effective treatment option for a variety of patient pathology, most commonly rotator cuff tear arthropathy and glenohumeral arthritis (Bonnevialle et al. 2020). Glenoid implant positioning is a difficult aspect of shoulder arthroplasty, and malpositioning of the glenosphere has been shown to be linked to inferior patient outcomes and increased rates of revisions (Gates et al. 2020; Guery et al. 2006). These unfavorable patient outcomes can be caused by scapular notching, reduced range of motion with impingement, instability, and aseptic loosening, all of which may occur in part due to poor implant positioning of the glenoid baseplate and subsequently the glenosphere (Favre et al. 2010; Gutiérrez et al. 2008). As RSA is increasingly performed (Farley et al. 2021), it becomes evermore essential to determine optimal implant positioning parameters for each patient and identify methods of accurately executing surgeon’s preoperative plans.
Prior studies have found improved precision and accuracy of implant placement with the use of three-dimensional (3D) planning software (Iannotti et al. 2019), demonstrating high levels of concordance in screw angle, screw length, and glenosphere size (Lilley et al. 2022). Most studies assessing accuracy of preoperative planning have assessed glenoid version and inclination (Berton et al. 2022; Friedman et al. 1992). However, the RSA angle is another useful metric for consideration when planning RSA. This angle was described by Boileau in 2019 (Boileau et al. 2019) and is significant in that it provides a reliable measure of the inclination of the inferior glenoid, where the baseplate for an RSA is ideally placed. The surgeon should aim to correct this angle to near zero degrees to obtain neutral inclination of the glenospehere (Boileau et al. 2019). There is little literature currently assessing the accuracy of preoperative planning for the RSA angle, despite its theoretical benefits over global glenoid inclination measurements in RSA (Werthel et al. 2023).
Preoperative 3D modeling with a virtually planned RSA construct is increasingly used to prepare for shoulder arthroplasty. While the rationale behind this software is that preoperative planning may help improve glenoid component positioning, more studies are needed to determine how accurate implant inclination and implant version planned measurements are to postoperative measurements. Commercially available planning platforms do not directly compute a true RSA angle for the final implant, but it is possible to compare native RSA angle of a radiograph to implant inclination. The aim of this study was to evaluate radiographic measurements such as version, inclination, and RSA angle using preoperative x-ray imaging, preoperative 3D models with virtually planned RSA constructs, and postoperative x-ray imaging. Our hypothesis is that the implant version and implant inclination measurements will be similar between the planned and postoperative cohorts, indicating accurate placement of implants according to the preoperative plan.
MATERIALS AND METHODS
Institutional review board approval (STUDY00005986) was obtained for this study. Ninety-two consecutive patients underwent preoperative planning for RSA with a commercially available 3D planning software program (Blueprint, Wright Medical Technologies Inc., Memphis, TN, USA) between October 2019 and January 2023. The patients all underwent primary RSA with standard instrumentation for any pre-operative indication. 19 patients were excluded because they did not have true anteroposterior and axillary view radiographs completed both preoperatively and within the first 12 weeks postoperatively. In the other 73 patients, glenoid version and RSA angle were measured on preoperative plain radiographs to assess the native glenoid anatomy. Implant version and implant inclination were measured on preoperative 3D models with virtually planned RSA constructs with a goal of neutral inclination and neutral to 10° of retroversion. Implant version and implant inclination were measured on postoperative plain radiographs. All measurements were carried out by two fellowship trained orthopedic shoulder and elbow surgeons. Preoperative planning measurements were performed manually using the plan PDF guide and goniometer software (GeoGebra, BYJU’S, Bangalore, India), while preoperative and postoperative radiographic measurements were performed manually using the goniometer function on the Visage imaging viewer program (Visage 7, Pro Medicus Ltd., San Diego, CA, USA). All angles were measured twice to ensure accuracy. Post-operative patient outcomes were retrospectively taken from the EHR system.
Measurements
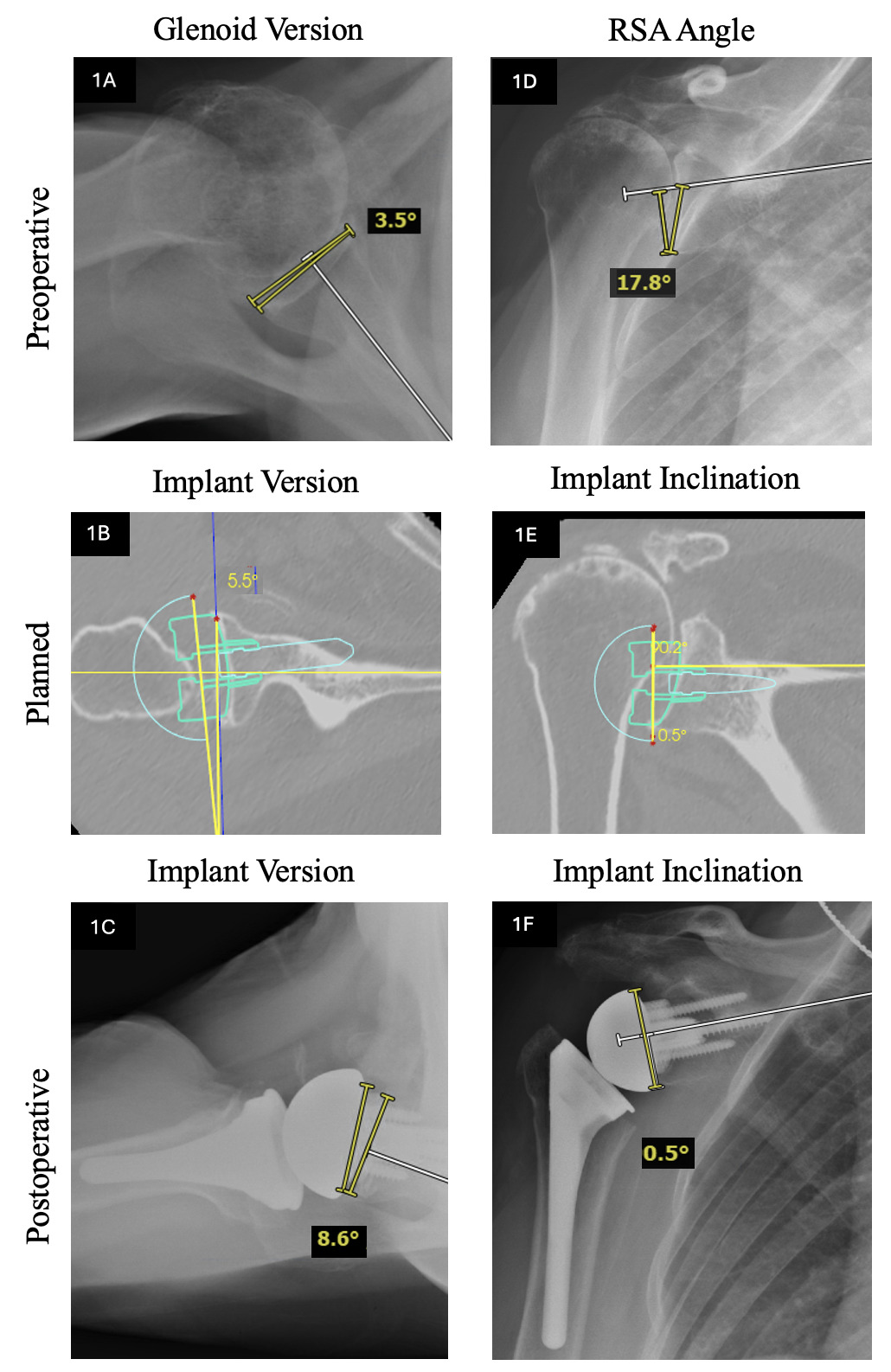
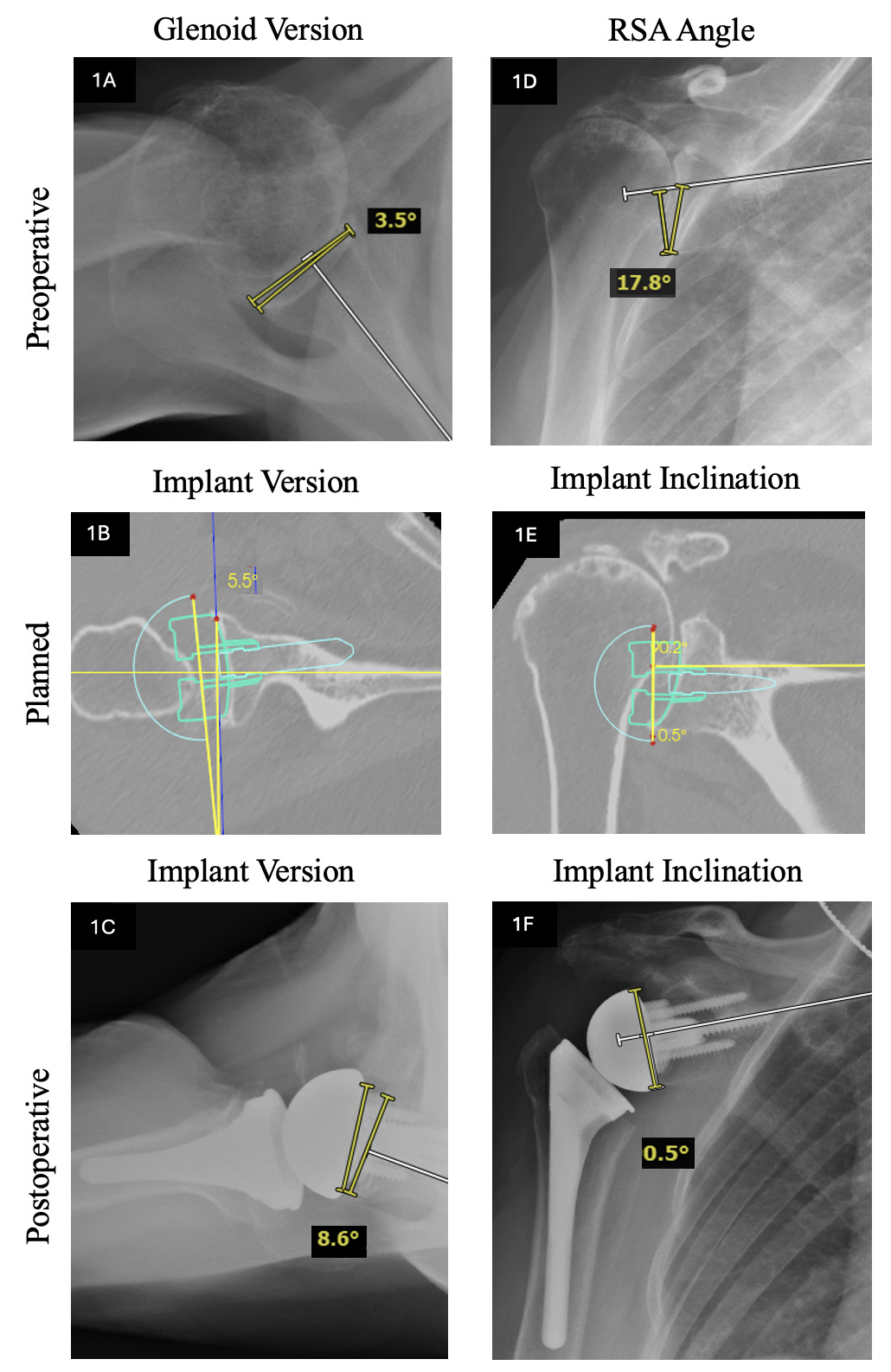
Preoperative glenoid, planned implant, and postoperative implant version were measured using the technique described by Friedman et al (Friedman et al. 1992). On an axillary radiograph of the shoulder, a line perpendicular to a line connecting the medial border of the scapula and the midportion of the glenoid was used. The angle between the perpendicular line and a line connecting the anterior and posterior rim of the glenoid produced the measurement of version (Figure 1A, 1B, 1C). The preoperative RSA angle was measured using the technique described by Boileau et al (Boileau et al. 2019). On a true anteroposterior radiograph of the shoulder, a line perpendicular to a line drawn along the supraspinatus fossa was used. The angle produced between that perpendicular line and a line connecting the inferior glenoid to the intersection point between the line along the floor of the supraspinatus and glenoid surface produced the RSA angle (Figure 1D). Planned implant and postoperative implant glenoid inclination was measured using the technique described by Werner et al (Chalmers et al. 2017; Werner et al. 2021). On a true anteroposterior radiograph of the shoulder, a line perpendicular to a line drawn along the supraspinatus fossa was used. The angle between that perpendicular line and a line parallel to the glenosphere is glenoid produced the measurement of inclination (Figure 1E, 1F). For version, anteversion was recorded as a positive number and retroversion was recorded as a negative number. For inclination, superior inclination was recorded as a positive number and inferior inclination was recorded as a negative number.
Statistical Analysis
Descriptive statistics were used to calculate mean, standard deviation, and 95% confidence intervals from the four measurements taken for each angle. Paired t-tests were performed for pairwise comparisons regarding version, inclination, and RSA angle among preoperative, planned, and postoperative values. P-values were adjusted using the Benjamini & Hochberg method with significance set at p<0.05 (Iannotti et al. 2019). Statistical analyses were conducted with R software (Version 4.2.1, R Core Team, Vienna, Austria). No statistical analysis regarding inter-observer or intra-observer reliability were performed.
RESULTS
The mean and standard deviation for the preoperative glenoid version and RSA angle, planned implant version and inclination, and postoperative implant version and inclination are shown in Table 1.
Comparisons of the preoperative, planned, and postoperative parameters of version and inclination are shown in Table 2. In comparing the preoperative measurements to the surgical plan, there was a significant difference between the preoperative glenoid version and the planned implant version (-4.46°, 95% CI [-6.16°, -2.76°], P<0.001) as well as the preoperative RSA angle and the planned implant inclination (16.07°, 95% CI [14.77°, 17.35°], P<0.001), reflecting the planned correction of native anatomy to the surgeon’s plan of ideal implant placement. In comparing the surgical plan to the postoperative implant position, there was a significant difference between the planned implant version and the postoperative implant version (1.17°, 95% CI [1.03°, 2.39°], P<0.001) as well as a significant difference between the planned implant inclination and the postoperative implant inclination (1.03°, 95% CI [0.4°, 1.67°], P=0.002). While these parameters reached statistical significance, a difference of less than 2° between the surgical plan and the postoperative implant position does not demonstrate clinical significance. In comparing the preoperative glenoid anatomy to the postoperative implant position to evaluate the overall correction, there was a significant difference between the preoperative RSA angle and the postoperative implant inclination (15.03°, 95% CI [13.61°, 16.45°], P<0.001) as well as a significant difference between the preoperative glenoid version and the postoperative implant version (-6.17°, 95% CI [-7.93°, -4.41°], P<0.001).
Out of the 73 patients who underwent RSA with pre-operative planning, four did not continue to follow-up in clinic for at least 6 months. Of those that had 6-month follow-ups, four underwent revisions (2 for periprosthetic infections, 2 for post-operative implant trauma). Three other patients had a different postoperative complication (stem rotational instability (1), coracoid impingement (1), scapular spine fracture (1)). No scapular notching was noted on any of the 6-month postoperative X-rays.
DISCUSSION
In this study of 73 shoulders utilizing preoperative planning for RSA with a commercially available 3D planning software program, differences between preoperative and postoperative measurements were significant when comparing glenoid version with implant version and RSA angle with implant inclination, indicating correction in all shoulders. Postoperative measurements of implant version and implant inclination more closely matched the planned measurements with a mean difference between 1° and 2°, indicating intraoperative recreation of the planned parameters. These results suggest that using a 3D planning software program leads to an accurate recreation of planned implant version and inclination.
Precise positioning of the glenoid baseplate in RSA remains technically challenging, but incorporation of a preoperative 3D planning software program has shown improved accuracy with implant placement. Venne et al (Venne et al. 2019). analyzed imaging for 18 patients that underwent RSA and demonstrated that the use of a preoperative 3D planning software program showed excellent interobserver reliability in measuring baseplate version and inclination compared to conventional two-dimensional methods. Berhouet et al (Berhouet et al. 2017). investigated how accurately surgeons can virtually position glenoid components in 30 shoulders when they could visualize the entire scapula compared to restricted visual access to only the exposed glenoid on a virtual 3D model. Their results demonstrated that full visibility of the scapula lead to significantly improved mean glenoid version (+1.4° vs. +0.3°) and mean glenoid tilt (+7.6° vs. +0.1°). Lilley et al (Lilley et al. 2022). performed a recent systematic review on the concordance between 3D preoperative planning with software and final implant placement in RSA. Four (79 patients) out of nine studies, showed minimal mean deviation from planned version (range: <1° to 4.4°) and planned inclination (range: 1.6° to 5°). Although our study did find significant differences between planned and postoperative measurements for implant version (1.71°) and implant inclination (1.03°), the differences were minimal and likely not clinically relevant. Additionally, the differences between planned and postoperative measurements were significantly smaller than between preoperative and postoperative measurements for version (-6.17°) and inclination (15.03°). These results align with previous studies in that preoperative planning leads to good accuracy of glenoid implant placement.
RSA angle is newer measurement used in preoperative planning of the glenoid baseplate, which is why we chose to include in our study. It was developed to measure the inclination of the inferior glenoid, which corresponds to where the glenoid component of the RSA is placed. It is crucial to avoid superior inclination in RSA. Multiple studies have shown that superior inclination is associated with negative clinical outcomes like scapular notching (Falaise et al. 2011), increased glenoid baseplate loosening, and postoperative instability (Bries et al. 2012; Tashjian et al. 2018). Previously, there was concern between studies on how inclination is defined and measured consistently (Gutiérrez et al. 2011), but the RSA angle has been shown to better estimate the inferior glenoid inclination as opposed to the β-angle (Lilley et al. 2022) or overall glenoid inclination and is a useful tool in preoperative planning to ensure a neutral tilt of the glenoid component for RSA (Boileau et al. 2019). Boileau et al (Boileau et al. 2019). analyzed RSA angle measurements for 47 shoulders that underwent RSA and found that the mean RSA angle was 25° ± 8° on plain radiographs, 20° ± 6° on two-dimensional CT scans, and 21° ± 5° on a 3D planning software program. Our results showed a significant difference between preoperative RSA angle and postoperative implant inclination (15.03°, 95% CI [13.61°, 16.45°]), with mean planned implant inclination of -2.5° and postoperative implant inclination of -1.5°, indicating that the use of a preoperative 3D planning software program allowed for accurate placement of the glenoid implants to correct the RSA angle and thus correct the glenoid inclination and avoid superior tilt of the component. RSA angle is a promising development for pre-operative planning, but not all platforms currently directly calculate RSA angle so potential software updates, regulation, and future studies are needed to properly utilize and investigate the accuracy of preoperative planning for the RSA angle.
While the use of a preoperative 3D planning software program for RSA has improved implant positioning, intraoperative computer-assisted navigation serves as another tool to improve precision and accuracy. Garcia et al (Velasquez et al. 2023). performed a systematic review of 10 articles comparing computer navigation that utilizes a CT scan-based preoperative planning software and conventional instrumentation for RSA. The pooled outcome analysis revealed a statistically significant lower baseplate deviation in the navigation group compared with the conventional group for planned inclination (−8.8°), but not for planned version (−0.4°). In a retrospective review of 16,723 anatomic and reverse total shoulder arthroplasties, Larose et al (Larose et al. 2023). demonstrated minimal deviation in the final intraoperative glenoid implant position for version (0.6° ± 1.96°) and inclination (0.2° ± 2.04°) compared to the preoperative plan. Although not evaluated in our study, computer-assisted navigation offers real-time intraoperative guidance to improve accuracy of glenoid component implantation.
Our results demonstrated good accuracy with the use of a preoperative 3D planning software program for RSA, but other studies have shown discrepancies. Erikson et al showed that pre-operative planning software had low levels of inter-reliability of angle measurement compared to surgeons, so continued studies that compare the accuracy of commercially available software are necessary (Erickson et al. 2021). Furthermore, future studies could delve deeper into the lower costs and increased efficiency in the operating room that result from incorporating preoperative planning. Raiss et al (Raiss et al. 2020). reported complete concordance between the preoperative plan and final implant selection in 90% of RSA cases, which will help with surgeon preparedness, implant stocks, and possibly future implant production. Sheth et al (Sheth et al. 2022). retrospectively compared patients who underwent shoulder arthroplasty with and without a preoperative 3D planning software program and found that preoperative planning did not reduce time in the operating room, but it was correlated to a significant decrease in the number and cost of sterilized trays.
Studies have shown that the average revision rate for rTSA due to surgical complications within the first two years is between 2.5-5.0% (Kolakowski et al. 2025). 2.7% of our patients underwent revisions due to periprosthetic joint infection, which is on the lower end of this range. There were also two patients who underwent revision due to trauma to the original implant, but we did not include these due to their surgical indication. Other post-operative complications of our patients within the first six months included scapular spine fracture (1), coracoid impingement (1), and stem rotational instability (1). Rates of complications among our patients were lower than have been seen in previous studies (Galvin et al. 2022; Parada et al. 2021). All patients at 6 month follow up showed good positioning of the implant on x-ray with no obvious signs of scapular notching. While longer follow-up and higher patient numbers are needed, these findings suggest that the use of pre-operative planning resulted in beneficial clinical outcomes for our patients.
This study does have limitations. There is potential for variability in the goniometer measurement of angles on radiographs and CT scans, however measurements of the radiographic values were repeated to improve accuracy. There may be limitations in comparing angles measured from preoperative 3D planning software to postoperative radiographs as they are two different imaging modalities. This could be overcome by obtaining postoperative CTs to compare corresponding measurements, however this may pose an additional risk to patient health due to radiation exposure and may be affected by metal artifact. Furthermore, we were unable to perform a statistical analysis of inter-observer or intra-observer reliability. Generalizability of findings may be limited by the small sample size of patients included as well as surgeon-specific factors that may affect the reproducibility of the surgical plan in the operating room.
CONCLUSION
Significant differences between preoperative and postoperative measurements were observed when comparing native glenoid version with implant version and native RSA angle with implant inclination, demonstrating the value of utilizing preoperative planning software to improve RSA implant positioning. Postoperative measurements of implant version and implant inclination also closely matched the planned measurements, showing that the surgical plan is adequately reproduceable intraoperatively. Continued study of the accuracy in preoperative planning is paramount to understanding its influence on patient outcomes and implant survival in RSA.