Introduction
The goal of spine surgery is to relieve pain, prevent further injury, and restore patients’ physical function and mobility. As many patients with spinal pathology are highly sedentary prior to surgery, improved ambulation can be a key indicator of surgical success, with walking tolerance as a commonly used metric (Norden et al. 2017; Yokota et al. 2025). Traditionally, surgical outcomes have been assessed with patient-reported outcome measures (PROMs) like pain scales, disability indices, and quality-of-life surveys. However, there is growing interest in leveraging wearable pedometers to objectively quantify postoperative recovery and outcomes through metrics like step counts and maximum walking distance (Bassett et al. 2017). This review explores the extent to which pedometer-derived metrics, particularly step counts, can serve as reliable indicators of functional recovery following spine surgery.
Pedometers and wearable activity monitors can objectively quantify several important aspects of physical activity and functional recovery following spinal surgery. Specifically, they have been used to measure daily step counts, distance traveled, gait speed, step length, cadence, and posture quality, all of which provide valuable insight into patients’ mobility and functional improvement postoperatively (Pryce et al. 2012; Angelucci et al. 2023). Additionally, trends in the step count data recorded from wearable pedometers can be used to assess the stages of recovery that patients are in, with rapid increases associated with acute healing and gradual plateauing with stabilization (Chaudhry et al. 2020; Ma et al. 2025). Pedometer data can be used to predict outcomes that traditional PROMs may not pick up: one study by Stienen et al. found that reduced activity level, as measured by step count, correlated with depression, suggesting that step counts may also reflect psychosocial dimensions of recovery not captured by traditional outcome measures. Notably, recent evidence suggests that objective measures like the 6-minute walk test can detect functional improvements even when PROMs plateau due to ceiling effects, highlighting the limitations of subjective metrics in well-performing patients (Ziga et al. 2023). Similarly, in a large prospective cohort following total joint arthroplasty, Crizer et al. found that postoperative step counts correlated only weakly with patient-reported outcomes, underscoring the value of objective activity monitoring as a complementary tool to gauge recovery trajectories (Crizer et al. 2017).
Over the past decade, interest in utilizing this data within spine surgery has grown, as evidenced by the increasing number of studies on the matter (Natarajan et al. 2023). Much of this enhanced interest has been fueled by advances in both technology and accessibility; as gyroscope and accelerometer designs have compacted, engineers have become increasingly capable of fitting pedometers into more devices than ever before, such as smartphones, smartwatches, and wearable fitness trackers, among others (Huhn et al. 2022). These innovations have made it possible to capture meaningful, objective activity data in spinal patients. For example, Maldaner et al. demonstrated that cervical spondylosis patients exhibit significantly reduced physical activity compared to general population norms, and proposed continuous wearable monitoring as a reliable, validated clinical outcome tool to assess functional impairment before and after spinal intervention (Maldaner et al. 2024). Similarly, Bahadori et al. found that objective physical activity measured via accelerometry correlated with both surgical invasiveness and PROMs, supporting its use as a surrogate for perioperative functional status and recovery trajectory (Bahadori et al. 2024). Below, we summarize the peer-reviewed literature on the utilization of pedometer data in guiding postoperative rehabilitation, assessing functional improvement, and gauging success in the context of spine surgery.
Methods
2.1. Search Strategy
We performed a literature search in the PubMed, Embase, and Scopus databases from inception through March 2025. The searches combined Medical Subject Headings (MeSH) terms and free-text keywords such as “Spinal Fusion,” “Spinal Stenosis,” “Spinal Surgery,” “Step Count,” “Accelerometry,” “pedometer,” “Gyroscope,” and “Wearable Sensor.” Full search terms for each database are listed in Supplementary Table 1.
2.2. Selection Criteria
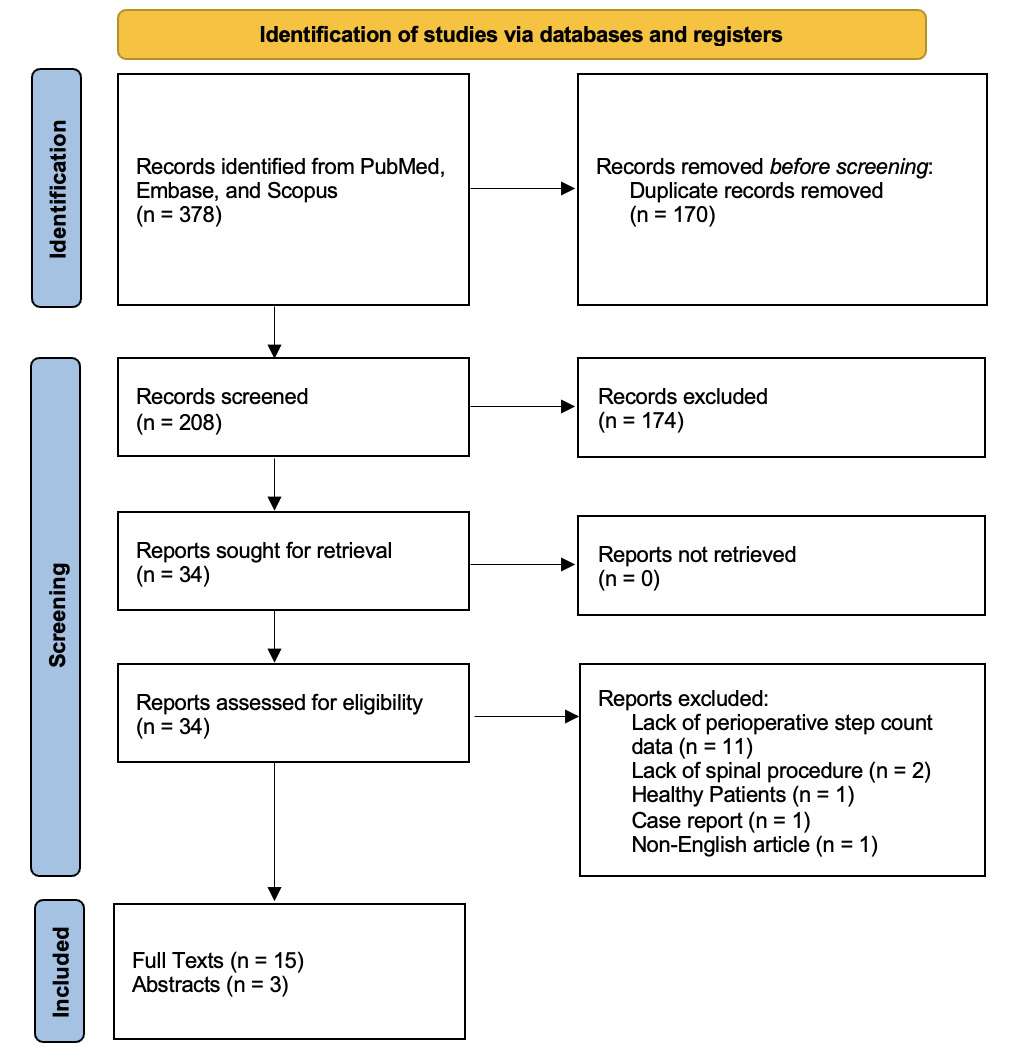
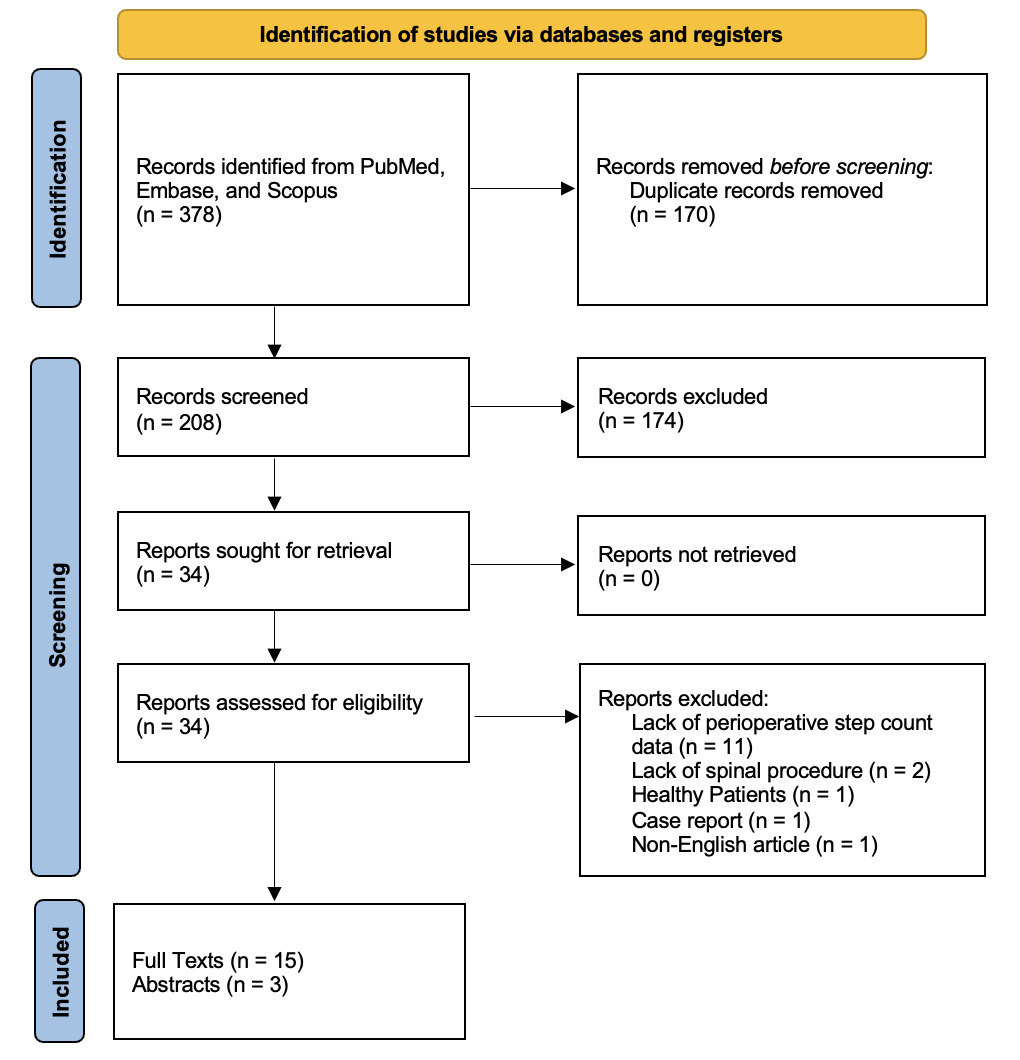
The screening process adhered to the PRISMA extension for scoping reviews (Tricco et al. 2018) and is visualized in Fig. 1. English-only articles must have discussed: (1) spinal surgery and (2) the use of a wearable sensor for tracking step count. Studies focusing on non-spine-related procedures and those where both pre- and post-step counts were not reported were excluded. Article types included randomized controlled trials, cohort and case-control studies, and observational studies. Case reports were excluded. Each identified article’s title, abstract, and full text were screened for relevance. After initial screening by three independent reviewers (SK, ND, NP), conflicts were resolved by discussion with a fourth reviewer (DP). Articles meeting the criteria were retained, and the final reference list was then generated. Only evidence of sufficient quality was included. Given the diverse nature of studies included, a formal risk-of-bias or quality scoring process was not feasible. However, all reviewed sources were thoroughly assessed for methodological rigor, clarity in outcome reporting, and level of evidence.
2.3. Data Extraction and Synthesis
Data extracted from the final references included procedure type, device used, timing of measurements, step count trajectories, adverse events, and correlations with clinical outcomes. We conducted a narrative synthesis of relevant studies to investigate current applications of perioperative step count monitoring in spine surgery, identify knowledge gaps, and highlight potential advancements in the field.
3. Results
3.1. Literature Review
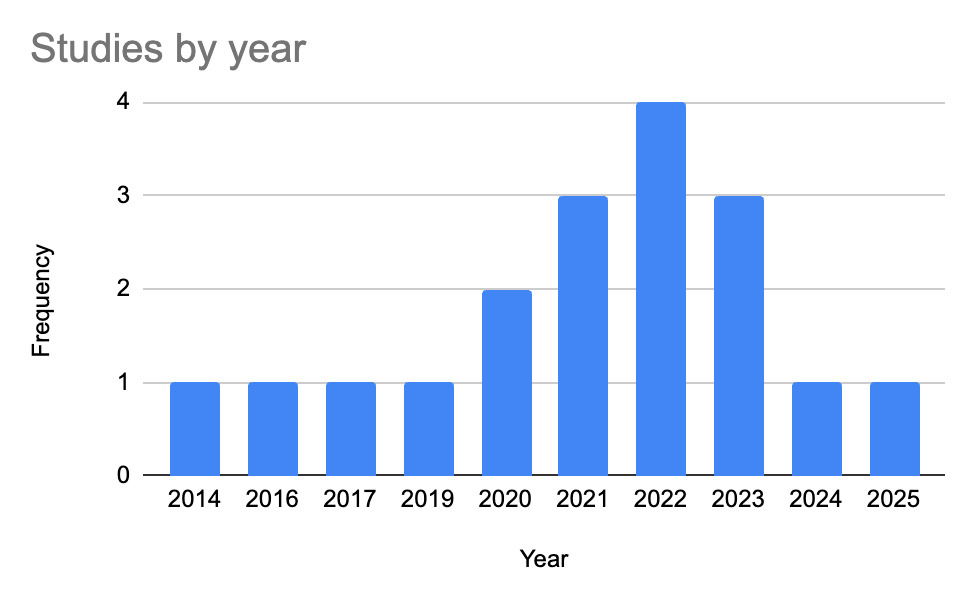
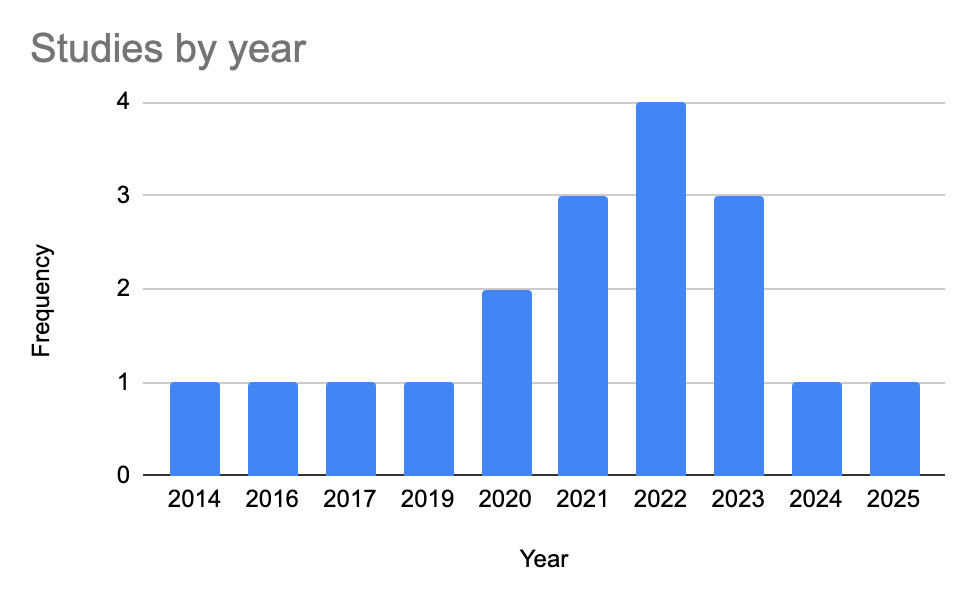
Our initial search produced 378 full-text articles and abstracts; 18 articles (n=677 patients) satisfied all inclusion criteria (Table 1). Eliminated papers included a lack of perioperative step count data (n=11), non-spinal surgery (n=2), a non-English article (n=1), healthy subjects (n=1), or a case report (n=1). Most studies were written in the United States, Australia, and Belgium, and published from 2014 to 2025 (Fig. 1).
Procedures included decompression (LD; n=10), fusions (LF; n=4), posterior spinal fusion (PSF) studies for adolescent idiopathic scoliosis (AIS; n=3), and complex, multi-level deformity surgeries (n=2), with one study involving both LD and LF. All studies targeted spine-related surgical interventions (McIlroy et al. 2025; Ahmad et al. 2022; Aubry et al. 2021; Ohtaki and Mamizuka 2014; Mobbs et al. 2019; Bienstock et al. 2022; Archer et al. 2024; Chauhan et al. 2023; Maharaj et al. 2022; Stienen et al. 2020; Mobbs et al. 2022; Basil et al. 2021; Tileston et al. 2023; Ackermans et al. 2023; German Spine Society 2021; Scheer et al. 2017; Mobbs et al. 2016; Ghent et al. 2020). Comprehensive data extraction of all studies can be found in Supplementary Table 1.
3.2. Decompression
Ten studies involved ambulation assessments before and after lumbar decompression surgeries in 269 total patients (McIlroy et al. 2025; Ahmad et al. 2022; Aubry et al. 2021; Ohtaki and Mamizuka 2014; Mobbs et al. 2019; Bienstock et al. 2022; Archer et al. 2024; Chauhan et al. 2023; Maharaj et al. 2022; Stienen et al. 2020). Most surgeries investigated effects after lumbar operations exclusively (n=7), while Chauhan et al. involved a combination of operations on the lumbar, lumbar-sacral, and cervical areas of the spine. Common metrics to represent functional recovery included daily step counts from worn or smartphone devices, the 6-minute walking test (6MWT), and specific gait components, including sway range. Correlations with this functional data were made with PROMs, visual analog scale (VAS), and Oswestry Disability Index (ODI) score, with varying degrees of significance. In most patients, step counts tended to decrease immediately after surgery but then increased significantly by 12 weeks post-surgery.
Neurogenic claudication, where spinal nerves are compressed and lead to pain, is a common indication that leads to spinal surgeries. With the most comprehensive patient sample, McIlroy et al. (2025) prospectively studied 97 adults (ages >50 yrs) with neurogenic claudication post-laminectomy (McIlroy et al. 2025). Ambulation was captured objectively with a thigh-mounted ActivPAL3 accelerometer (PAL Technologies Ltd, Glasgow, UK) and functionally with a 6MWT plus self-rated maximum walking distance. Step counts, 6MWT, and a self-rated maximum walking distance all rose significantly at 12 weeks (steps: +582; 6MWT: +61.4 m, 25% compared to baseline; self-rated distance: +400 m; all p<0.001). Despite promising results, only 49% (6MWT), 40% (steps, MCID ≥ 558 steps), and 58% (self-rated distance, MCID ≥ 250 m) achieved clinically meaningful gains. Preoperative walking ability (lower-limb performance, prior falls, and fear) predicted most outcome gain, explaining variance in 67% of 6MWT change, 75% of step count change, and 38% of self-rated distance change. Psychological barriers (fear of falling/movement and illness) at 6 weeks predicted reduced gains. The authors argue that effective protocols should couple pre-habilitation with early postoperative interventions that mitigate fear and other modifiable psychosocial barriers. These findings support a promising though nuanced role of pedometer data utility in spine surgery outcome prediction (McIlroy et al. 2025). This impact is reinforced by Ahmad et al. (2022), who conducted a two-year retrospective observational study of 14 patients undergoing lumbar decompression for spinal stenosis (n=10) or disc herniation (n=4) using step counts from 2-year Apple smartphone data (Apple, Cupertino, California, USA) ± 365 days. Eleven patients regained or exceeded preoperative activity within a year, with a mean daily step increase of 551 (p=0.002), suggesting meaningful functional recovery (Ahmad et al. 2022). This shows that these effects are not limited to stenosis or compression, which suggests wide applicability for monitoring ambulation to track recovery.
Improvements in step counts over time are also seen in Aubry et al. (2021), who observed 26 patients undergoing lumbar decompression for stenosis and/or disc herniation using a three-dimensional waist-worn GT3X+ accelerometer (ActiGraph LLC, Pensacola, FL, USA) (Aubry et al. 2021). Daily steps increased from preoperative baseline by 1,058 at 6 weeks and 610 at 12 weeks postoperatively, but not significantly or within the ideal range of 7,000+ daily steps per day (Tudor-Locke et al. 2011). However, step count strongly correlated with moderate-to-vigorous activity (r = 0.837 at 6 weeks; r = 0.775 at 12 weeks; both p < 0.001) (Aubry et al. 2021).
Furthermore, gait metrics beyond just step count can be assessed, including step length and sway range, as seen in Ohtaki & Mamizuka (2014). They examined 18 patients with lumbar spinal stenosis (LSS) undergoing lumbar decompression using a miniature inertial measurement unit (ZMP Inc., Japan) (Ohtaki and Mamizuka 2014). While there was an insignificant increase in daily step counts (558 ± 215 preoperative to 648 ± 124 postoperative), there was a significant step length increase by 0.07 m three months post-operation, which demonstrates greater gait efficacy and reduced compensatory shortening of stride due to pain or instability (p<0.01). Spatial analysis showed that the mean sway range in pitch rotation was reduced significantly by 0.69° (p<0.05). Spatial analysis showed that the mean sway range in LSS patient-pitch rotation was reduced significantly by 0.69° (p < 0.05), suggesting better spinal alignment (Ohtaki and Mamizuka 2014). The use of adjunct measurements to step counts is seen in Mobbs et al. (2019), who assessed 13 patients post-unilateral laminectomy for spinal stenosis decompression using a wrist-based accelerometer to generate the Gait Posture Index (GPi) (Mobbs et al. 2019). GPi is a combination of four metrics: step counts, gait velocity, step length, and posture with ambulation. At 3-month follow-up, daily step count increased by 1,977; GPi scores for step count, gait velocity, step length, and posture demonstrated improvements (p<0.01 for each), and Oswestry Disability Index (ODI) scores improved by 18.615 points (p=0.002). This suggests a correlation between stenosis severity and GPi changes (Mobbs et al. 2019).
A comparison in early versus late postoperative ambulation variability between decompression and lumbar fusion can be seen in Bienstock et al. (2022), which tracked 20 patients in a cohort study undergoing lumbar laminectomy, with/without fusion, using a wrist-worn Fitbit accelerometer (Fitbit, Fremont, CA, USA) (Bienstock et al. 2022). Median daily step counts significantly decreased in early recovery (first 130 days after surgery, p ≤ 0.002) than the preoperative baseline (30 days before surgery). The greatest rate of increase (β = 66, p<0.001) and variability in step count (CV = 0.42) occurred around postoperative day 40. Postoperative days 130-184 saw minimal variability (CV = 0.14) and no significant rate of increase. Fusion patients showed greater increases (p<0.001), although neither group returned to baseline at 6 months. Still, ODI and 2-Item Short Form Health Survey (SF-12) scores significantly improved compared to baseline (p<0.01), implying that step count reflects acute recovery but not long-term improvements (Bienstock et al. 2022). This is reinforced by Archer et al. (2024), who conducted an RCT of 60 patients with lumbar degeneration undergoing laminectomy with/without fusion and with/without telehealth follow-up using a wrist-worn Fitbit device. No significant difference was found in daily step counts. However, the study’s quantification of step counts did not begin until 2 weeks postoperative, which potentially misses a notable early recovery window, as step count variability may be more sensitive to differences in healing rates between groups (Archer et al. 2024).
To enhance this focus to include clinically meaningful results and subsequent correlations with pain, Chauhan et al. (2023) analyzed 21 laminectomy patients using smartphone data collected via Apple Health over 5 years (Chauhan et al. 2023). Changes in steps at 6 weeks inversely correlated with Patient Reported Outcomes Measurement Information System Physical Intensity (PROMIS-PI) and VAS pain (r=-0.46, p=0.032), suggesting that greater improvements in mobility correlated with greater reductions in pain interference. At 12 weeks, those meeting minimal clinically important differences (MCIDs) for pain showed step increases (+34% for VAS; +56.5% for PROMIS-PI), while others declined. Patients who met MCID thresholds in VAS pain or PROMIS-PI demonstrated greater recovery of mobility, as measured through step counts, than those who demonstrated no MCIDs (p<10-10 in VAS pain; p<10-17 in PROMIS-PI). However, conclusions drawn for lumbar decompression-specific effects are limited due to conditions being aggregated (Chauhan et al. 2023). These results suggest that patients who felt less pain were also more mobile, implying that step count is a potential objective marker of clinical recovery. Maharaj et al. (2022) provide an objective comparison in 24 patients undergoing lumbar fusion (LF) for degenerative spondylolisthesis (n=12) or lumbar decompression for spinal stenosis (n=12) using a wrist-worn Mi Band 2 smartwatch (Xiaomi, China) (Maharaj et al. 2022). At 12 weeks postoperatively, mean daily step count improved in the fusion group (+2,300) and the decompression group (+3,700). Daily distance also improved in the fusion group (+2,000 m; p=0.01) and decompression group (+2,100; p=0.02). ODI scores declined by 17 and 10 points in the fusion and decompression groups, respectively, suggesting that functional mobility gains accompanied meaningful reductions in disability (Maharaj et al. 2022).
A comparison between outcomes for cervical or lumbar spine surgeries can be made with Stienen et al. (2020), who tracked 30 patients undergoing cervical or lumbar spine surgery using a low-cost consumer-grade Mi Band accelerometer (Xiaomi, China) (Stienen et al. 2020). 30-day preoperative activity averaged 5,624 steps/day, decreasing by 71% in postoperative week 1 (p<0.001) followed by 37% and 23% lower at weeks 2 and 4, respectively. Gradual returns were seen in 8-12 weeks but generally failed to surpass pre-op averages at 1 year. Patients with cervical spine disease showed higher step counts at both baseline and follow-up than lumbar disease patients. Fusion procedures were associated with 48% lower activity one week post-operation (p=0.032). No significant correlation with ODI/NDI, but activity inversely correlated with depression scores at 3 months (r=-0.739, p=0.003). However, a comparison cannot be made between decompression-only and the combination of decompression and fusion due to the study aggregating each intervention between the lumbar and cervical cohorts (Stienen et al. 2020). Overall, this suggests that while functional recovery gains were limited, step tracking proved feasible and informative for physical and psychological outcome monitoring.
3.3. Fusion
Four studies assessed ambulation before and after lumbar fusion surgeries in 132 total patients (Chauhan et al. 2023; Maharaj et al. 2022; Mobbs et al. 2022; Basil et al. 2021). Common metrics used to gauge functional recovery include step count, gait velocity, walking distance, ODI, and VAS. All four studies exhibited a common trend: initial post-operative reductions in step count followed by a gradual return to or exceeding of baseline mobility usually by 6-12 weeks. Additionally, there was a moderate correlation between increased step counts and improvements in pain (VAS) and function (ODI, PROMIS-PI).
Across Chauhan et al. and Maharaj et al. in lumbar fusion patients, postoperative increases in step count consistently showed correlation with functional gains and pain reductions. Although decompression patients tended to recover earlier, fusion patients were able to achieve greater functional gains by 12 weeks (Chauhan et al. 2023; Maharaj et al. 2022)
Following a similar trend of inverse correlation between step count improvement and pain scores in a fusion-only cohort, Mobbs et al. (2022) analyzed 87 Anterior Lumbar Interbody Fusion (ALIF) patients (Mobbs et al. 2022). Improvements were seen in step count (+27%) and gait velocity (+0.21 m/s) at 3 months postoperative. By 6 months, fusion rates reached 87%, VAS pain decreased (-5.3, p<0.0001), and 88% of patients reported good/excellent outcomes. Together, these studies suggest that improvement in step metrics as measured by an accelerometer correlates with decreased pain in patients (Mobbs et al. 2022).
Separately, long-term assessments add evidence that activity naturally recovers and can be tracked remotely. Basil et al. (2021) analyzed 23 LF patients who had their pre- and postoperative step counts, flights climbed, and distance traveled tracked using smartphone-based accelerometry data from the Apple Health app (Apple, Cupertino, CA, USA) (Basil et al. 2021). Activity levels significantly declined from 6 months preoperatively through the immediate 2-week postoperative recovery period, but gradually recovered over time. Patients surpassed pre-op averages for flights climbed, step count, and distance by 7.6 ± 21.1, 8.0 ± 9.9, and 10.3 ± 14 weeks, respectively. The study supports the feasibility of tracking the objective progress of recovering spine surgery patients using smartphone-based step count and distance (Basil et al. 2021).
3.4. Adolescent Idiopathic Scoliosis and Posterior Spinal Fusion
Three studies involved ambulation assessments in adolescent idiopathic scoliosis (AIS) patients before and after posterior spinal surgery in 148 total patients (Tileston et al. 2023; Ackermans et al. 2023; German Spine Society 2021). The common objective assessments in these studies are step count and return to baseline, while the common subjective assessments include the functional disability inventory and PROMIS. Each study found a sharp reduction in activity levels (steps/day) in the early postoperative period.
Tileston et al. (2023) examined 17 adolescents (mean age: 14 years) with idiopathic scoliosis (AIS) undergoing PSF using a tracker worn for several weeks preoperatively and for 3 months postoperatively (Tileston et al. 2023). On average, patients returned to baseline mobility within 28 days post-surgery (range: 14–32 days) and to maximum preoperative daily step count within 48 days (range: 33–66 days). 88% of patients returned to their baseline mobility by 3 months. The number of fused levels didn’t affect recovery time, and PROMs didn’t significantly correlate with mobility, except for improvements in step count and PROMIS scores (p = 0.03). Despite recovery variability, most patients resumed baseline mobility within 3 months, offering guidance for recovery expectations (Tileston et al. 2023).
Ackermans et al. (2023) retrospectively analyzed 48 AIS patients undergoing spinal fusion using an ActiGraph accelerometer (GT3X+, ActiGraph LLC, Pensacola, FL, USA) worn at the waist (Ackermans et al. 2023). Patients were grouped by lowest instrumented vertebra (LIV: thoracic vs. lumbar) and fusion length. Compared to preoperative baseline (13,049 steps/day), step counts dropped significantly post-surgery at 3 (6,486 steps/day) and 6 weeks (8,723 steps/day; both p < 0.001). The thoracic fusion group consistently showed higher step counts than the lumbar group at both postoperative time points (3 weeks: p = 0.002; 6 weeks: p = 0.033). Similar to Tileson et al., fusion length did not impact early postoperative step counts. Regression analysis demonstrated that the Functional Disability Inventory (FDI) scores at 3 weeks were the only significant predictor (17.6% of variance; p=0.011) of early recovery. This suggests that LIV placement affects early functional recovery, while traditional PROMs don’t predict step count improvements, highlighting the value of objective activity tracking in early rehabilitation (Ackermans et al. 2023).
Ackermans et al. (2021) followed 83 AIS patients (mean age 15.4 years) undergoing PSF using accelerometers (GT3X+, ActiGraph LLC, Pensacola, FL, USA) at preoperative (T0), 3 weeks post-op (T1), and 6 weeks post-op (T2) (Ackermans et al. 2023; German Spine Society 2021). Pain intensity was assessed using an 11-point numerical scale, and fusion levels were quantified based on UIV and LIV vertebral positions. Step count improved between T1 and T2 but remained below baseline. No correlation was found between mobility, pain scores (UIV/LIV), and long-term outcomes (FDI and Pediatric Quality of Life Inventory (PedsQL) (German Spine Society 2021).
Together, the findings of these three studies suggest that early postoperative mobility is poorly predicted by surgical extent or pain and is not indicative of long-term functional outcomes. This is a starkly different finding from the four studies in the lumbar fusion section. If true, this would point to a gap in the surgeon’s ability to forecast early recovery trajectories.
3.5. Spinal Deformity with Complex Multilevel Surgery
Two studies involved ambulation assessments in 62 patients with spinal deformity requiring complex multilevel surgery. Scheer et al. (2017) tracked 32 patients post-thoracolumbar spinal deformity surgery using personal 3D accelerometers to monitor daily activity continuously (Scheer et al. 2017). Of 22 completing the study (preoperative step counts range: 1,278 ± 767 to 17,800 ± 6,464; postoperative range: 891 ± 587 to 12,655 ± 7,038), 11 improved step counts at 6 months, and 2 showed statistically significant gains (p<0.05). The cohort showed significant improvement in ODI, SF-36 Physical Component Summary (SF-36 PCS), and all SRS domains (p<0.05). Preoperative daily steps correlated significantly with ODI (r=-0.61, p=0.0058) and SF-36 PCS (r=0.60, p=0.0114), suggesting that pre-op activity moderately predicts functional status (Scheer et al. 2017).
Mobbs et al. (2016) tracked 30 patients undergoing complex lumbar spine surgery–including ALIF, fusion, diskectomy, and laminectomy–using accelerometers to assess daily step count, distance traveled, and calories burned (Mobbs et al. 2016). Of 28 compliant patients, mean step counts increased from 5,255 ± 2,883 (preoperative) to 7,135 ± 3,112 (2 months postoperative; p=0.002) and 8,312 ± 4,218 (3 months postoperative; +58.2%; p=0.008). Distance traveled increased from 3.8 ± 2.2 km to 5.3 ± 2.5 km per day (2 months; +39.5%; p=0.002) and 6.2 ± 3.6 km (3 months; +63%; p=0.0004). However, no significant correlation was found between objective metrics and VAS, ODI, or SF-12 scores. This disconnect highlights the limitations of subjective PROMs and supports the use of step count and distance traveled to monitor functional recovery (Mobbs et al. 2016).
3.6. Microdiscectomy
To date, one study has investigated pre-/postoperative ambulation in microdiscectomy patients. This study focuses on objective gait metrics, including but not limited to step count, related to functional recovery and disability scores before and after operation (Ghent et al. 2020). Ghent et al. (2020) assessed 24 patients post-lumbar microdiscectomy using GPi using one of three different wearable accelerometers (Apple, San Francisco, California, USA; Garmin Ltd., Lenexa, Kansas, USA; Xiaomi, Beijing, China). At 3-month follow-up, GPi scores (+26.5), step count (+4,029), gait velocity (0.36 m/s), step length (0.15 m), and ODI (-38.2) improved (p<0.001 for each)–with a moderate correlation between changes in GPi and ODI (r=0.56, p=0.005). from 59.3 to 85.8 (p<0.001). This supports GPi as a complementary objective mobility metric and supports wearable gait analysis in assessing functional recovery (Ghent et al. 2020).
4. Discussion
4.1. Objective Step Counts vs. Patient-Reported Outcomes
All studies included wearable-derived metrics and patient-reported outcomes (PROMs). Objective data reflect movement, while PROMs capture subjective experience. The two measures may align or diverge. Across spinal surgery types, accelerometer data showed a recovery pattern: an initial postoperative decline in step counts followed by return to baseline within 6–12 weeks. Several studies reported disconnects between objective and subjective measures. Objective mobility does not always align with subjective recovery; wearable tracking provides insight when PROMs are limited by under- or overreporting. The methods are complementary. PROMs reflect pain and quality of life, while pedometer data measure functional recovery in daily settings. Combined, they inform care plans, support ERAS protocols, and identify outlier recovery trajectories (Mittal et al. 2025).
4.2. Clinical Utility of Wearable Activity Monitoring
Accelerometers may support preoperative planning and postoperative care, as many patients carry smartphones or fitness trackers. For clinicians, accelerometer data supplements PROMs by tracking changes in activity. For patients, self-tracking may improve adherence to rehabilitation routines (Alfieri et al. 2022).
Further, it is reasonable to expect that wearable accelerometers might reduce costs by better-targeting care (Sharan and Prasad 2019). These devices may produce postoperative risk metrics, allowing physicians to better stratify patients and flag those who might need further follow-up care. This tool can be useful for chronic patients or patients with traumatic identifications, such as TBI (Mischler et al. 2023). Paired with biological biomarkers that provide complementary signals of neuroinflammatory and neuronal damage processes, wearable data can augment recovery tracking (Kaniuk et al. 2025). Additionally, in an era of spine surgery where robotics are becoming increasingly popular, wearable accelerometer data might be used to inform preoperative trajectory planning and otherwise provide intraoperative technology with more data points (Sadagopan et al. 2024; Prasad et al. 2025).
Beyond spinal surgery, the utility of objective mobility monitoring may be applied to other orthopaedic populations, including total knee and total hip arthroplasty patients whose recovery is associated with ambulation (Lei et al. 2021; Bristol 2021). In such patient populations, step count and other gait metrics may create a marker for tracking functional recovery and detecting early deviations from predicted recovery trajectories. Furthermore, smartphones, such as the Apple iPhone, Samsung Galaxy, and Google Pixel, have built-in accelerometers that are capable of measuring step count and ambulation to offer greater accessibility for patients, with preliminary findings showing potential for their usage (Ghaffari et al. 2023). However, this form of monitoring depends on patient adherence to wearing the device, which may result in less consistent data. Further studies should compare mobility metrics derived from smartphones and wearables in postoperative populations.
4.3. Predictive Value of Pre- and Postoperative Step Count
Preoperative activity may have prognostic value for postoperative recovery. Several studies suggest that patients with higher preoperative activity recover faster. Preoperative ambulation may translate to improved postoperative function and aligns with frailty as a modifiable risk factor. Further research is needed. If validated, prehabilitation protocols may increase ambulation and improve outcomes.
Postoperatively, early functional data might hold predictive potential. Chauhan et al. (2023) showed that lumbar surgery patients who achieved MCID improvements in pain and function demonstrated early postoperative step count increases (34–56% by 6 weeks) and faster mobility recovery, suggesting that early gains in activity may predict superior patient-reported outcomes. There is potential for activity metrics to assist as a risk-stratification tool: a low preoperative step count or a slow ramp-up in mobility post-op might identify patients who need more intensive rehab or closer follow-up. If validated, clinicians could use pre-operative step count as one factor in counseling patients, and early postoperative step trends might help facilitate timely interventions for patients deviating from the expected recovery path.
However, there are limitations: the variability in devices and monitoring protocols hinders the predictive power of step counts. This includes device variability (wristbands, smartphones, waist/thigh mounted accelerometers); placement, algorithms, and user compliance; data collection windows–pre- and postoperative tracking ranged from 3 weeks to 12 months, all varied (Ahmad et al. 2022; Stienen et al. 2020; Ackermans et al. 2023). This variability is further compounded by the fact that step count, despite its widespread use, remains poorly validated in this population, with very low-quality evidence supporting its use as a physical outcome measure (Kowalski et al. 2024; Maganja et al. 2020). For example, Gilmore et al. found that wrist-worn commercial devices like Fitbit and Jawbone severely underreported steps in post-lumbar fusion patients—particularly those using gait aids—highlighting the significant impact of both placement and postoperative gait alterations on monitor validity (Gilmore et al. 2020). Some reported raw values, others normalized to baseline. This heterogeneity limits comparability. Standardization of devices, data windows, and outcome reporting is needed to improve data interpretation and enable more personalized care planning (Wijndaele et al. 2015). Furthermore, nearly half of the studies had patient populations less than 30 (8/18); these small sample sizes make it difficult to generalize to a larger patient population, as these cohorts may be more susceptible to selection bias and outlier effects. Overall, these factors contribute to the variance in significance when comparing step counts with patient recovery in the literature.
5. Conclusion
This scoping review found that step count monitoring provides an objective complement to traditional patient-reported outcomes in assessing postoperative recovery after spinal surgery. Across lumbar decompression, fusion, scoliosis correction, and complex deformity cases, a consistent pattern of initial postoperative decline followed by gradual return to baseline within 6 to 12 weeks was observed. Objective step counts moderately correlated with subjective improvements in pain and function, though discrepancies were common. Early postoperative mobility and higher preoperative activity levels showed predictive value for recovery outcomes. Variability in device type and monitoring protocols highlights the need for standardization. Step count tracking holds promise for personalizing rehabilitation, enhancing postoperative surveillance, and improving clinical decision-making.
Ethical Considerations
The authors declare no competing interests to declare that are relevant to the content of this article.
Funding
No funding was received for conducting this study.
Data Availability
No datasets were generated or analyzed during the current study.
Supplementary Information (SI)
Supplementary Table 1 provides an overview of the studies that incorporate metrics of perioperative pedometer data in patients who undergo spinal surgeries. The table includes each respective author of the study, publication years, experimental design, subject parameters, outcome measures, key findings, presence of adverse effects, type of clinical indication, and significance of improvement.
Abbreviations Used in Supplementary Table 1: Oswestry Disability Index (ODI); EuroQOL 5-Dimension Health Questionnaire (EQ-5D); Patient Health Questionnaire-4 (PHQ-4); Short Falls Efficacy Scale–International (SFESI); Brief Illness Perception Questionnaire (B-IPQ); Patient-Reported Outcomes Measurement Information System (PROMIS); Visual Analog Scale (VAS); Patient-Reported Outcome Measures (PROMs); 12-Item Short Form Health Survey (SF-12); 36-Item Short Form Health Survey (SF-36); Scoliosis Research Society-30 Questionnaire (SRS-30); Functional Disability Inventory (FDI); Pediatric Quality of Life Inventory (PedsQL); Zurich Claudication Questionnaire (ZCQ); Patient Satisfaction Index (PSI); Neck Disability Index (NDI); Health-Related Quality of Life (HRQoL); Physical Component Summary (PCS); Mental Component Summary (MCS); 6-Minute Walk Test (6MWT); Moderate-to-Vigorous Physical Activity (MVPA); Gait Posture Index (GPi); Gait Velocity (GV); Upper Instrumented Vertebra (UIV); Lower Instrumented Vertebra (LIV); Minimal Clinically Important Difference (MCID); Randomized Controlled Trial (RCT); Pearson correlation coefficient (r); Probability value (p).