Introduction
End-stage degenerative disease of the hip and knee remains a leading cause of global disability (Steinmetz et al. 2023). Osteoarthritis affects more than 500 million individuals worldwide and is a major contributor to years lived with disability, particularly in aging populations (Steinmetz et al. 2023). Total hip arthroplasty (THA) and total knee arthroplasty (TKA) are among the most effective and cost-efficient interventions in modern medicine, providing durable pain relief, functional restoration, and sustained improvements in quality of life (Wilson et al. 2021). In high-income countries, access to total joint arthroplasty (TJA) has expanded steadily, with procedural volumes rising in parallel with increased life expectancy and expectations for prolonged mobility (Stubnya et al. 2025).
In contrast, access to TJA remains profoundly limited in low- and middle-income countries (LMICs) (Nham et al. 2024a; Rudisill et al. 2023; Amen et al. 2022; Nham et al. 2024b; Woolley et al. 2025; Goodman et al. 2023; Farias et al. 2025). More than five billion people worldwide lack access to safe and affordable surgical care, with musculoskeletal disease representing a substantial source of untreated morbidity (Meara et al. 2015). The Lancet Commission on Global Surgery identified surgical disease as a critical yet under-addressed component of global health, emphasizing that inadequate operative access directly contributes to preventable disability and long-term socioeconomic dependence (Meara et al. 2015). Within this context, TJA remains disproportionately unavailable because of implant cost, supply-chain dependence, infrastructure requirements, and limited financial access to care (Pearl and Saleh 2024).
Disparities in arthroplasty access are particularly pronounced in South Asia, where patients frequently present at younger ages with advanced deformity and severe functional impairment. Delayed presentation reflects limited nonsurgical treatment options, restricted subspecialty availability, and the absence of reliable pathways to definitive operative management. Even within tertiary referral centers, arthroplasty capacity is often constrained by system limitations rather than patient demand. At the Indus Hospital and Health Network in Pakistan, one of the largest fully charitable healthcare systems in the region, the wait time for primary TJA exceeds ten years, driven by persistent implant shortages, prohibitive procurement costs, and limited infrastructure capable of supporting sustained high-volume arthroplasty.
Despite these constraints, TJA performed in resource-limited settings has demonstrated substantial clinical value. Prior studies report marked improvements in pain, function, and patient-reported outcomes, with results approaching those achieved in high-income environments.¹ Economic analyses further support TJA as a cost-effective intervention when durability and restoration of functional independence are considered, reinforcing both ethical and health-system imperatives to expand access (Wilson et al. 2021).
International orthopaedic outreach initiatives have emerged to address this unmet need (Meara et al. 2015). Existing literature has emphasized ethical considerations, logistical challenges, and sustainability concerns, with particular focus on follow-up, implant logistics, and infrastructure variability (Bido et al. 2018). However, most published efforts describe low procedural volumes or generalized mission structures rather than adult reconstructive surgery delivered at scale (Bido et al. 2018; “Progress - Operation Walk,” n.d.). Large-scale TJA introduces distinct challenges, including dependence on predictable implant supply chains, extensive instrumentation, standardized perioperative pathways, blood management protocols, and coordinated operating room workflows; demands that are further amplified when operative volume is concentrated within short timeframes or bilateral procedures are performed.
Despite the growing global burden of degenerative joint disease, there remains limited published guidance describing how high-volume TJA can be delivered safely, efficiently, and reproducibly in resource-limited environments. Current literature inadequately addresses critical systems such as preoperative imaging acquisition, implant forecasting, operating room efficiency optimization, multidisciplinary alignment, and integration of surgical education within high-throughput care models. Few reports describe longitudinal partnerships capable of supporting continuity of care and progressive institutional capacity development.
The purpose of this review is to describe a systems-based framework for high-volume TJA delivery in a resource-limited setting through international surgical collaboration. Drawing on experience developed through the Gift of Disability Alleviation (GODA) in partnership with the Indus Hospital and Health Network in Pakistan, this manuscript outlines the organizational structure, logistical planning strategies, and collaborative principles required to perform large numbers of THA and TKA safely within a condensed operative period. Emphasis is placed on reproducible systems including preoperative planning, implant and instrumentation management, operating room efficiency, multidisciplinary coordination, anesthesia strategy, and integrated education, rather than isolated clinical outcomes.
This manuscript represents a narrative, practice-based implementation analysis derived from longitudinal program experience between 2018 and 2026, contextualized within existing global orthopaedic and systems literature. It is not intended as a systematic review, but rather as a structured description of a scalable TJA delivery framework supported by aggregate program-level outcome data.
Program Overview and Institutional Partnership
The development of sustainable high-volume TJA programs in resource-limited environments requires close alignment between international organizations and host institutions capable of supporting complex perioperative care. The framework described in this review is based on a long-standing collaboration between the Gift of Disability Alleviation (GODA), a United States–based 501(c)(3) nonprofit organization, and the Indus Hospital and Health Network in Pakistan. This partnership was established to address the substantial unmet burden of degenerative joint disease through structured surgical delivery and longitudinal capacity development rather than episodic intervention.
GODA is a physician-led organization focused on expanding access to orthopaedic care through international collaboration, surgical education, and infrastructure support. Its multidisciplinary teams include fellowship-trained adult reconstruction surgeons, anesthesiologists, physical therapists, and operational personnel. Program design emphasizes standardized surgical systems, reproducible workflows, and integration with local providers to ensure continuity of care beyond visiting operative periods.
The Indus Hospital and Health Network is among the largest fully charitable healthcare systems in Pakistan and serves as a national referral center for complex orthopaedic conditions. Despite established operating rooms, inpatient wards, and rehabilitation services, access to elective arthroplasty remains severely constrained. Demand far exceeds capacity, with wait times for primary TJA exceeding ten years, reflecting systemic limitations rather than lack of surgical expertise.
The collaborative arthroplasty program operates annually across multiple sites, including Karachi, Lahore, and Muzaffargarh. Each mission is conducted over a six-day operative period and delivers high volumes of primary THA and TKA within a compressed timeframe, typically ranging from 250 to 300 procedures. Concentrated surgical delivery during a single operative week results in a meaningful reduction in institutional arthroplasty waitlists. A substantial proportion of cases involve bilateral TJA performed under standardized selection criteria and unified perioperative protocols.
A defining feature of the program is the limited number of visiting surgeons relative to operative volume. Surgical throughput is achieved through meticulous preoperative planning, parallel operating room utilization, standardized instrumentation, and coordinated multidisciplinary workflows. Visiting surgeons operate alongside Pakistani attending surgeons, fellows, and residents, facilitating technical exchange while maintaining a consistent operative philosophy.
Shared ownership of patient care is central to the partnership. Local surgeons participate in patient evaluation, intraoperative decision-making, and postoperative management, ensuring continuity of care following mission completion. Integration of trainees across all phases of care supports education while strengthening institutional capacity for sustained arthroplasty delivery.
Through longitudinal collaboration, GODA and the Indus Hospital and Health Network have developed a scalable operative framework capable of delivering complex adult reconstructive surgery within the constraints of a resource-limited environment. The following sections outline the challenges inherent to high-volume TJA and the systems-based strategies used to address them.
Program Performance and Safety Metrics
Between 2018 and 2026, approximately 1,500 primary THA and TKA procedures were performed within this collaborative framework. Aggregate program-level outcome tracking demonstrates low early complication rates. Over this period, eight deep periprosthetic joint infections were identified (0.53%). No perioperative mortality events were recorded, and no early unplanned readmissions were documented. Ten cases of aseptic loosening have been observed to date (0.67%).
During concentrated operative periods, approximately 45 to 60 primary THA and TKA procedures are performed daily across three centers, reflecting coordinated high-throughput delivery supported by standardized systems.
Although this manuscript focuses on implementation rather than formal comparative outcomes analysis, these aggregate data suggest that TJA delivered within this structured framework demonstrates low observed complication rates within this program in low-income settings. Length of stay, transfusion rates, and formal patient-reported outcomes were not systematically collected during the early years of program development and represent areas for future prospective data capture. Development of a prospective registry is underway to enable more granular reporting of perioperative metrics and long-term outcomes
Unique Challenges of High-Volume Arthroplasty in Resource-Limited Settings
Although international orthopaedic outreach programs have expanded surgical access in low- and middle-income countries, most published efforts describe limited procedural volumes delivered over short operative periods. While effective for isolated musculoskeletal conditions, these models are insufficient to address the burden of end-stage degenerative joint disease. Delivery of TJA introduces logistical, clinical, and systems-level challenges that differ fundamentally from traditional outreach care.
TJA is uniquely infrastructure dependent. Unlike fracture fixation or soft-tissue procedures, THA and TKA require predictable implant supply, multiple instrumentation sets, power equipment, sterile processing capacity, and standardized perioperative protocols. In resource-limited environments, disruption of any component can compromise efficiency or patient safety, particularly when operative volume is concentrated within a limited timeframe.
Implant availability represents a primary constraint to scalability. Accurate component selection requires advance knowledge of size distribution, polyethylene options, constraint availability, and revision backup components. Without preoperative forecasting, programs risk inventory mismatch, intraoperative delays, and case cancellation. Even minor discrepancies in implant supply can affect a large number of patients when case volume is high.
Operating room throughput presents an additional challenge. Efficient delivery depends on parallel room utilization, standardized tray layouts, predictable turnover, and consistent staffing. Many low-resource facilities lack THA- and TKA-specific workflows, and unfamiliarity among personnel can substantially limit daily case capacity without deliberate system optimization.
Anesthesia resources further constrain delivery. Patients undergoing THA and TKA frequently present with advanced disease and limited physiologic reserve, while bilateral procedures increase anesthetic complexity and postoperative monitoring demands. Variability in access to neuraxial techniques, regional anesthesia, and perioperative monitoring may restrict the number of cases that can be performed safely.
Sterile processing capacity is often rate limiting. THA and TKA instrumentation sets are extensive and require meticulous reprocessing. Inadequate turnaround capability may disrupt case sequencing or necessitate additional tray redundancy, increasing logistical burden and limiting throughput.
Surgeon-to-volume mismatch represents another defining challenge. When operative demand exceeds the number of available surgeons, success depends on standardized technique, a consistent operative philosophy, and close integration with host-nation surgical teams. Without alignment, variability increases and efficiency declines.
Postoperative care and continuity also pose challenges at scale. High inpatient census places substantial demand on nursing, rehabilitation services, and discharge coordination. Safe recovery requires standardized rehabilitation pathways and reliable transition of care to local providers following completion of the operative period.
Collectively, these constraints underscore that TJA in resource-limited settings cannot be approached as an extension of traditional outreach models. Effective delivery requires deliberate systems-based planning integrating preoperative imaging, implant forecasting, operating room optimization, anesthesia coordination, and multidisciplinary alignment. The principal barriers distinguishing TJA from conventional orthopaedic outreach are summarized in Table 1.
Systems Required for High-Volume Arthroplasty Delivery
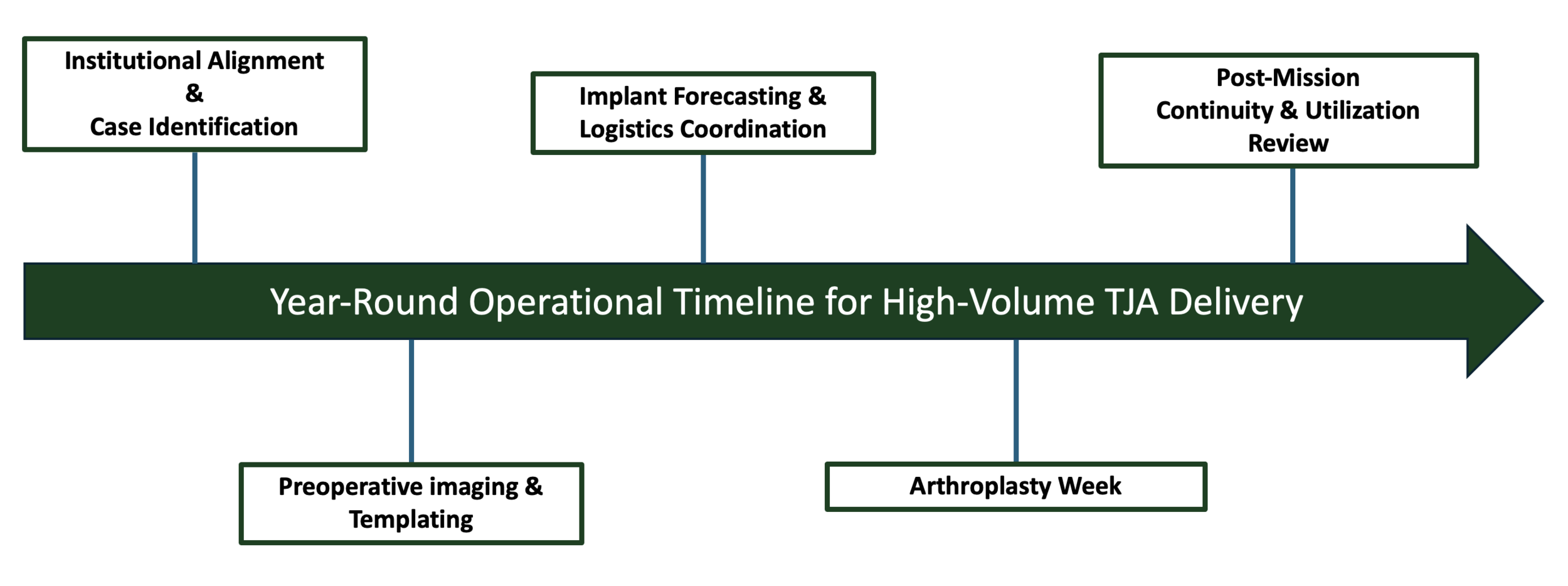
Successful delivery of TJA in resource-limited environments requires integrated systems that address the logistical and clinical demands of adult reconstruction. Unlike lower-volume outreach models, scalable TJA depends on coordinated planning across the full continuum of care, beginning months before the operative period and extending through postoperative management. The framework outlined below defines the essential system components required to achieve predictable throughput, maintain patient safety, and support long-term sustainability (Table 2, Figure 1).

Preoperative Imaging Acquisition and Case Planning
Preoperative planning is a primary determinant of success in TJA delivery. Accurate implant selection and operative efficiency depend on advance access to diagnostic imaging. Standardized radiographs of the pelvis, hip, and knee are obtained several weeks before the operative period and reviewed jointly by visiting and host-nation surgeons.
Early image acquisition enables digital templating, assessment of deformity severity, estimation of component size distribution, and identification of cases requiring stems, augments, or increased constraint. This process supports appropriate patient selection, including candidates for bilateral THA or TKA, and facilitates risk stratification for complex pathology. Systematic templating reduces intraoperative uncertainty and limits unnecessary implant inventory, mitigating delays and case cancellation in high-throughput settings.
Implant Forecasting and Inventory Coordination
Implant procurement represents one of the most complex logistical barriers to scalable TJA delivery and requires planning well in advance of the operative period. For international programs, implant acquisition is frequently dependent on donation-based supply chains with extended coordination timelines.
Following each annual operative period, implant utilization data and templating distributions are reviewed jointly by local and visiting surgical teams to forecast requirements for the subsequent year. This process typically begins approximately six months in advance and includes estimation of component size distribution, polyethylene thickness, fixation preference, and anticipated need for stems, augments, and constraint options. Delays in implant confirmation can significantly limit achievable surgical volume.
Industry participation is coordinated through nonexclusive charitable donation agreements. Primary implant systems have been provided by Zimmer Biomet (Warsaw, Indiana, USA), Stryker Orthopaedics (Mahwah, New Jersey, USA), and Total Joint Orthopedics (Salt Lake City, Utah, USA), with modular revision components donated when available, including additional support from United Orthopedic Corporation (New Taipei City, Taiwan) in 2024. Implant selection is guided by surgical familiarity, instrumentation compatibility, and logistical feasibility rather than local market presence.
Sustained access to a consistent implant platform supports longitudinal continuity of care. At select sites, use of a standardized primary knee system across multiple years has improved instrumentation availability, streamlined inventory planning, and enhanced operating room familiarity among local surgical teams. These experiences underscore the importance of durable relationships between charitable organizations and industry partners when delivering TJA at scale.
Instrumentation Standardization and Sterile Processing Considerations
THA and TKA instrumentation impose substantial logistical demands due to the number of trays required and the time-intensive nature of reprocessing. Scalable TJA delivery therefore requires deliberate assessment of sterile processing capacity to ensure reliable instrument turnaround between cases. Instrumentation is standardized across operating rooms with uniform tray composition and consistent setup to reduce variability and improve staff familiarity. Adequate tray redundancy is essential when multiple operating rooms operate concurrently, allowing uninterrupted case flow. Close coordination between surgical teams and sterile processing personnel enables predictable case sequencing and minimizes workflow disruption, particularly in environments where THA and TKA instrumentation is not routinely utilized.
Operating Room Efficiency and Throughput Optimization
Efficient operating room utilization is essential for achieving high procedural volume within a limited operative window. Parallel operating room models are employed, with dedicated THA and TKA teams assigned to each room. Standardized room configuration, consistent instrument positioning, and predetermined case sequencing reduce variability and improve turnover.
Surgeon workflows are aligned in advance to promote uniform operative technique and limit intraoperative decision variability. This standardization allows anesthesia teams, nursing staff, and technologists to anticipate procedural steps, improving coordination and safety. In high-throughput environments, incremental reductions in turnover time translate into meaningful increases in daily case capacity.
Alignment Between Visiting and Local Surgical Teams
Close integration between visiting surgeons and host-nation orthopaedic teams is essential for efficiency and sustainability. Alignment in surgical approach, implant selection, alignment principles, and postoperative protocols minimizes variability and supports predictable outcomes. Local attending surgeons participate directly in preoperative planning and intraoperative decision-making, while fellows and residents are integrated throughout all phases of care. This collaborative structure promotes bidirectional knowledge exchange and ensures continuity of care following completion of the operative period, with postoperative recovery, complication management, and rehabilitation remaining under the supervision of established local providers.
Perioperative and Anesthesia Coordination
Anesthesia delivery is a critical determinant of safety, efficiency, and recovery in TJA. Fellowship-trained anesthesiologists from the visiting team participate directly in patient care and collaborate closely with host-nation anesthesia providers to implement standardized perioperative pathways for THA and TKA. These protocols emphasize neuraxial anesthesia, multimodal regional techniques, and evidence-based fluid management to minimize physiologic stress and facilitate early mobilization. Routine use of spinal anesthesia and peripheral nerve blocks improves hemodynamic stability, reduces opioid requirements, and enhances postoperative pain control.
Collaboration between visiting and local anesthesia teams supports both clinical consistency and skills transfer. Shared protocols are reviewed before the operative period, and intraoperative discussions reinforce best practices commonly employed in high-volume arthroplasty settings. Emphasis is placed on patient selection, anesthetic management of bilateral procedures, intravascular volume optimization, and postoperative monitoring aligned with accelerated recovery pathways.
Standardized anesthetic techniques also enhance operating room efficiency. Reduced variability in induction and emergence times allows predictable case sequencing and turnover, while consistent postoperative pain protocols facilitate early ambulation and discharge readiness. Through longitudinal collaboration, host-nation anesthesia providers progressively integrate these perioperative principles into routine practice, strengthening institutional capability beyond the operative period and supporting sustainable TJA delivery.
Postoperative Care Integration and Discharge Planning
High-volume TJA places substantial demand on inpatient nursing, rehabilitation services, and discharge coordination. Standardized postoperative pathways are implemented to support early mobilization, multimodal pain control, and predictable discharge planning. GODA physical therapists collaborate directly with local therapy teams to initiate ambulation on postoperative day 0, representing a departure from prior practice patterns characterized by prolonged epidural analgesia and delayed mobilization.
This structured approach enables earlier functional recovery and improved inpatient throughput. Uniform physical therapy protocols across sites reduce variability and support consistent progression of care. Local surgical teams maintain primary responsibility for inpatient management and outpatient follow-up following completion of the operative period, with focused education on recognition and management of early postoperative complications, including wound issues, infection, and thromboembolic events.
To support continuity of care, supplemental implant inventory is maintained locally to facilitate irrigation and debridement procedures or component exchange when necessary. This integrated postoperative framework reinforces institutional ownership, maintains patient safety, and supports durable TJA care beyond the operative period.
Education, Training, and Capacity Building
Sustainable impact in global TJA initiatives depends not solely on procedural volume but on development of durable local expertise capable of maintaining care beyond the presence of visiting teams. Education and skills transfer are therefore integral components of international arthroplasty programs. The collaborative model emphasizes side-by-side operative participation between visiting surgeons and host-nation orthopaedic teams. Local attending surgeons, fellows, and residents are integrated throughout all phases of care, including preoperative evaluation, templating review, intraoperative execution, and postoperative management.
Training extends beyond surgical technique to perioperative systems management. Local teams receive instruction in operating room organization, instrumentation logistics, case sequencing, and turnover optimization, skills essential for scalable TJA delivery. Anesthesia education represents an additional pillar of capacity building, with visiting anesthesiologists collaborating with host-nation providers to reinforce evidence-based neuraxial techniques, regional analgesia, multimodal pain management, and perioperative fluid optimization.
Nursing staff and technologists are incorporated into standardized workflow training. Repeated annual collaboration enables progressive refinement of these practices and strengthens institutional familiarity with arthroplasty-specific requirements. Through longitudinal engagement, local teams progressively expand independent TJA capability, allowing programs to evolve from episodic service initiatives into sustainable partnerships.
Ethical Considerations and Sustainability
Ethical delivery of surgical care in resource-limited environments requires prioritization of patient safety, continuity of care, and institutional accountability. International TJA initiatives must avoid episodic intervention that places undue burden on host institutions or exposes patients to risk without reliable follow-up.
Host-institution leadership is central to this framework. Patient identification, clinical evaluation, and final operative selection are performed collaboratively with local orthopaedic teams to ensure that surgical indications align with available infrastructure, rehabilitation resources, and long-term follow-up capacity.
Continuity of care represents a core ethical obligation in TJA. Because joint replacement requires longitudinal monitoring, rehabilitation, and complication management, postoperative care remains under the direction of host-nation surgeons familiar with institutional protocols and resource constraints.
Transparency in patient selection is essential when surgical demand exceeds capacity. Standardized inclusion and exclusion criteria are defined in advance and applied uniformly, incorporating medical comorbidities, functional status, rehabilitation feasibility, and follow-up reliability to promote equitable access.
Visiting surgeons operate exclusively within established hospital systems under local credentialing processes. Care is delivered in coordination with host institutions, without parallel clinical pathways or independent postoperative structures, ensuring alignment with local governance and regulatory standards.
Sustainability is reinforced through longitudinal partnership rather than isolated mission activity. Recurrent collaboration supports refinement of perioperative systems, continuity of implant platforms, and responsible resource utilization.
Lessons Learned and Recommendations
Experience delivering TJA in a resource-limited environment underscores that surgical volume alone does not define program success. Rather, durability depends on systems integration, institutional alignment, and longitudinal partnership.
First, TJA delivery must function as a continuous operational process rather than a time-limited surgical event. Effective programs require year-round engagement, including post-mission utilization review, implant forecasting, and early coordination with supply partners to accommodate procurement timelines. Concentrated operative weeks represent the culmination of sustained planning rather than isolated activity.
Second, structured preoperative imaging and templating are indispensable. Advance radiographic acquisition enables accurate implant forecasting, identification of complex deformity, and appropriate selection of bilateral candidates. Programs lacking systematic preoperative planning are unlikely to achieve predictable throughput or safe case volume.
Third, standardization is foundational. Limiting implant platforms, instrumentation sets, anesthetic pathways, and postoperative protocols reduces variability, improves efficiency, and mitigates the impact of constrained resources. In high-throughput environments, reproducibility enhances both safety and capacity.
Fourth, multidisciplinary integration is essential. Alignment among surgeons, anesthesiologists, nursing staff, surgical technologists, and rehabilitation teams supports perioperative stability and coordinated recovery. Operating room efficiency, anesthesia standardization, and early mobilization depend on shared protocols and clearly defined roles.
Finally, sustainability requires host-institution ownership. Postoperative management, complication surveillance, and longitudinal follow-up must remain under local provider leadership. Educational engagement and progressive skill transfer allow programs to evolve beyond visiting-team dependence toward locally sustained arthroplasty capacity.
Together, these principles define a structured approach to scalable TJA delivery in environments traditionally considered unsuitable for complex elective reconstruction. Key distinctions between conventional mission-based care and a systems-driven arthroplasty model are summarized in Table 3.
Recommendations for Implementation
Based on these principles, organizations seeking to establish scalable TJA programs in resource-limited settings should prioritize the following:
-
Establish longitudinal institutional partnerships anchored in host-system leadership, shared accountability, and year-round engagement.
-
Implement structured preoperative imaging acquisition and digital templating well in advance of operative periods to enable accurate forecasting and case selection.
-
Standardize implant platforms, instrumentation, and perioperative pathways to reduce variability and improve throughput.
-
Integrate multidisciplinary perioperative teams to support anesthesia optimization, operating room efficiency, and coordinated rehabilitation.
-
Maintain local ownership of postoperative care and longitudinal follow-up to ensure continuity, ethical accountability, and long-term sustainability.
Future Directions
Continued expansion of TJA in resource-limited environments will depend on advancement of collaborative infrastructure, outcome measurement, and sustainable supply models. As institutional experience grows, opportunities exist to refine patient selection, optimize perioperative pathways, and expand locally led surgical capacity.
Development of prospective arthroplasty registries focused on low-resource settings represents a critical next step. Standardized collection of demographic data, implant utilization, complications, and patient-reported outcomes would enable objective performance assessment, support quality improvement initiatives, and inform data-driven resource planning.
Telemedicine and remote collaboration platforms may further enhance postoperative surveillance, multidisciplinary case review, and longitudinal education between operative periods, strengthening continuity of care while reducing geographic barriers.
Long-term sustainability will require transformation of implant supply strategies. While donated implants remain essential during early program development, reliance on international donation pipelines does not represent a permanent solution. Development of domestically produced implants tailored to native Pakistani anatomy may improve implant fit, simplify instrumentation, and enhance surgical reproducibility. Such initiatives could reduce dependence on external supply chains, stimulate domestic manufacturing, and generate economic benefit through workforce development. Procurement of locally produced implants for charitable surgical programs would further allow reinvestment of philanthropic resources directly into the host nation’s healthcare economy, creating a closed-loop model linking surgical access, education, and economic growth.
Finally, expansion of structured training pathways for surgeons, anesthesiologists, and perioperative staff remains essential. Progressive transition toward locally led TJA programs, supported by standardized systems and sustainable implant access, may ultimately enable independent large-scale arthroplasty delivery with selective international collaboration.
Conclusion
The global burden of end-stage degenerative joint disease continues to rise while access to TJA remains severely limited in many low- and middle-income countries. Although TJA has historically been viewed as impractical in resource-constrained environments, accumulated experience demonstrates that large-scale joint replacement can be delivered with low complication rates comparable to published benchmarks when supported by deliberate systems design and durable institutional partnership.
This review describes a scalable framework centered on preoperative planning, implant forecasting, operating room efficiency, multidisciplinary perioperative coordination, education, and ethical sustainability, with close alignment between visiting and host-nation teams and shared ownership of patient care. By prioritizing reproducible infrastructure over episodic intervention, international collaboration can extend the benefits of modern adult reconstruction to populations with longstanding unmet need while maintaining patient safety, surgical quality, and long-term sustainability.
Conflict of interest
Implants were provided through nonexclusive charitable donation agreements. No authors received personal financial compensation related to implant support. The authors report no conflicts of interest relevant to this work.