





Patellar tendon rupture is a devastating injury and occurs in approximately one per 100,000 knees (for any reason). (Figure 1) Following primary total knee arthroplasty (TKA), patellar tendon rupture approaches an incidence of 2.5%, and > 5.0% following revision TKA (Vaishya et al. 2016).

Generally, a patellar tendon rupture is classified by the time from injury. Acute ruptures are treated less than six weeks s/p injury:
-
The tissues aren’t contracted,
-
The tissues aren’t scarred down
-
The tissues are more mobile
-
All three allow for a primary repair
Chronic ruptures involve those that occurred at least two or three months and longer. These are the most difficult since:
-
The patella can be damaged
-
The soft tissues are usually contracted
-
Potential for avascular tissue scarring and ossification
-
The patellar tendon may have migrated
How do we fix this and believe it’s going to work? Unfortunately, the failure rates of patellar tendon repairs throughout the literature are poor for both acute and chronic repairs (Vaishya et al. 2016; Belhaj et al. 2017; Courtney et al. 2018; Hsu and Siwiec 2025). It’s commonly reported that most patients will have either failure of the repair, or significant extension lags with weakness, and require use of ambulatory aids. Therefore, the patient satisfaction rate is terrible.
How can that be? Why are we not improving these results?
Many small studies report the use of different constructs (mesh, allograph, autograph), they combine results of both acute (early) and chronic repairs (late with insufficient tissue), and include a wide variety of post-operative protocols, making the results even more difficult to interpret! Commonly, failure rates of primary repair strategies on chronic tendon tears were over 70 percent and include extension lags greater than 10 degrees (Courtney et al. 2018; Li et al. 2022; Nam et al. 2014).
Now what do we need to do to correct these poor outcomes?
While training under Dr. Donald Shelbourne of Purdue University, I saw that he developed a wire technique to protect the patellar tendon repair (Shelbourne et al. 2001). He threaded a wire through the patella, down each “gutter,” and through the tibia behind the tibial tubercle and leave it in place for six to eight weeks before a simple removal. Additionally, he had patients moving right away following surgery, because the adjunctive wire dampened the tension from the repaired tendon (with increasingly good results). However, one common adverse outcome was that in some cases, the wire would pull through the patella like a Gigli saw.
PROCEDURE
The patellar tendon repair protection technique that I use is a modification of the Shelbourne technique where a 1.7mm cable is used. The cable is not threaded through the patella but rather weaved through the quad above the superior boarder of the patella, allowing for greater tension over time, without pulling through the patella.
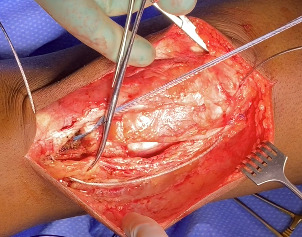
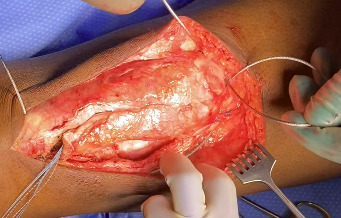
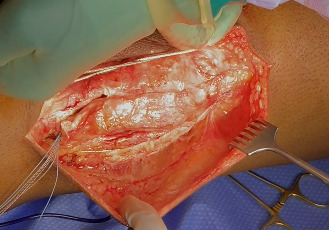
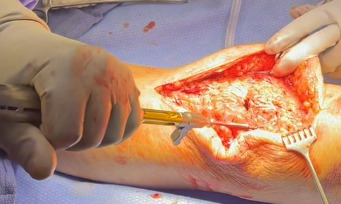
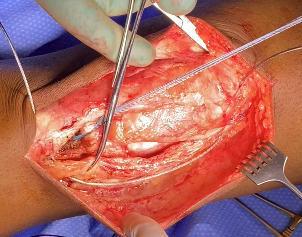
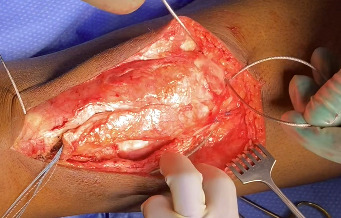
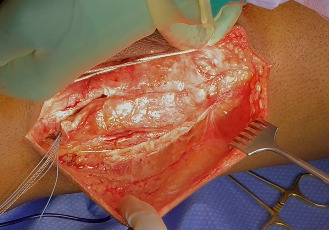
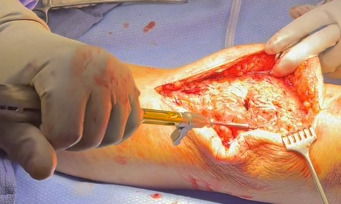
Following extensile exposure of the knee, an anchor suture is placed in the proximal tibia for the primary tendon repair. Next, a hole is drilled below the tibial tubercle through the diaphyseal bone, and the cable is passed through the tibia. Once passed through, the wire is laid within the gutters. (Figure 2) Before the cable is weaved through the quad, feel underneath to avoid passing the cable into the joint. (Figure 3) The cable is then weaved through the quad above the patella. (Figure 4) This technique allows for increased early tensile strength to that quad over time. Then, tighten and crimp the cable (Figures 5 & 6) and you bring the tendon together and then perform the repair. When tightening the cable
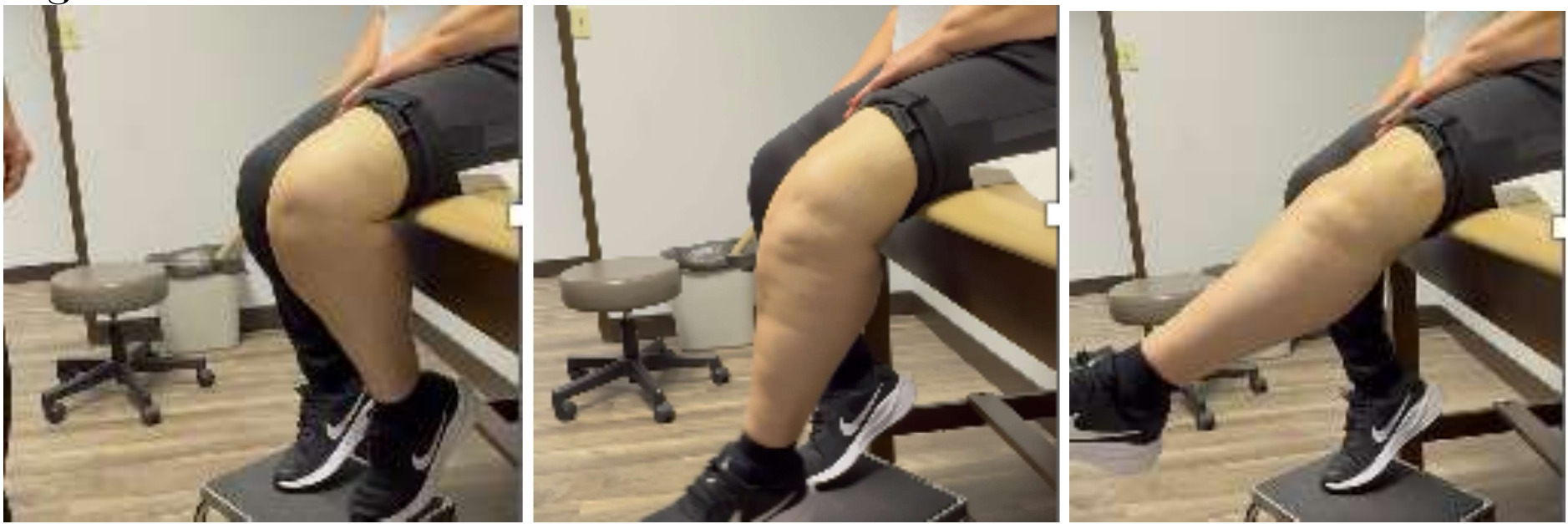
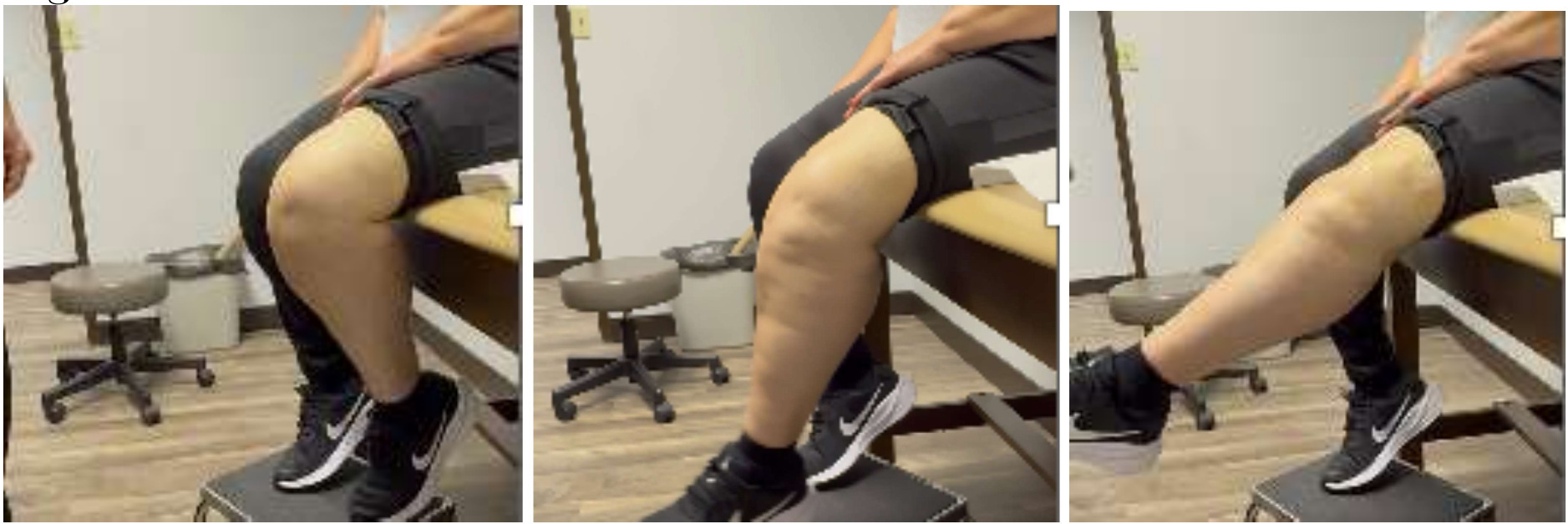
But how much do you tighten it? Tighten enough when let go against gravity the knee bends between 30 to 45 degrees. (Figure 7) This will allow good tendon repair protection so that they will stretch the quad out over time, and most of them achieve 90 degrees or more.


As for the patellar tendon repair, use whatever technique you’re familiar with. The purpose of this presentation is to teach the procedure to protect the repair. Unfortunately, the issue with the literature is that the repairs were never protected beyond a brace or a cast. Remember, if you protect the repairs, maybe we have something and the outcomes will be better.
POST-OPERATIVE ROM PROTOCOL (Table 1)
Besides the importance of the technique to repair the ruptured patellar tendon, protecting the repair post-operatively will yield successful outcomes. Initially, the repair needs to be fully protected for three to four weeks (you may need place the potentially non-compliant patients in a cast so they cannot bend knee and ruin the repair). Note that the soft tissues need time to scar down, so allow full extension only through 3 to 4 weeks post-op. Thereafter, the patient is allowed to bend the knee from zero to 30 degrees, and every two weeks, progress the patient in 15 degree increments up to 60 degrees. It’s necessary to keep them at 60 degrees for three months. If you want to remove the cable early, then the problem is continuing protection of tendon repair. Remember, repaired tendons take longer to mature than bone. However, the cable is easily removed as a simple outpatient procedure under fluoroscopy; find the crimp, make a tiny incision, cut the cable, and it almost always pulls right out without any resistance.
CASE EXAMPLE 1
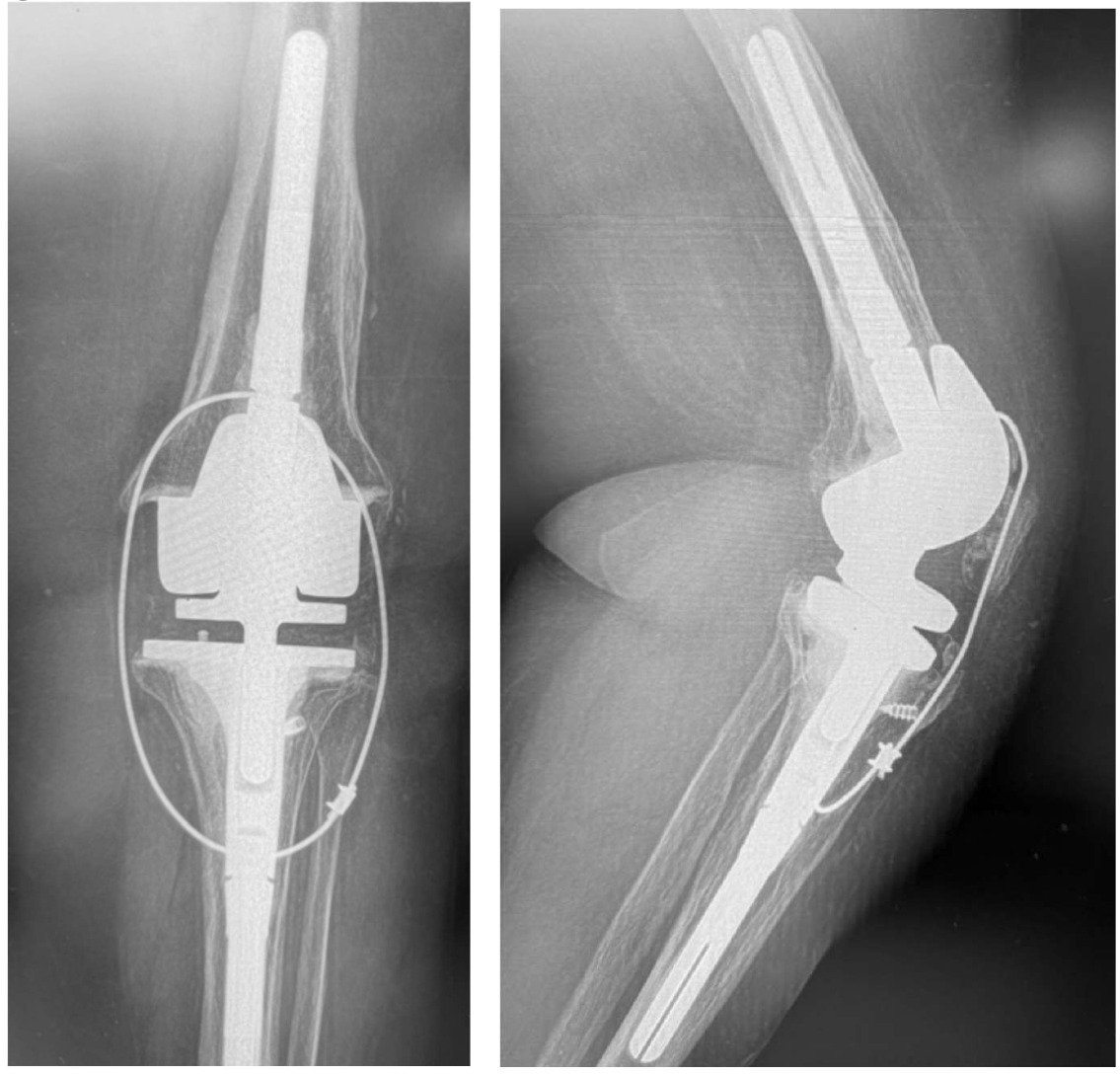
This is 74-year-old female, with a BMI of 33 kg/cm2, and multiple comorbidities (CHF, Arrhythmia, anxiety, 3 previous surgeries of the knee). She presented three months status post patellar tendon rupture, patellar fracture and dislocation. The patellar fracture was fixed with a wire, and in the radiograph you can see the anchor suture in the tibial tubercle area, the wire below the tubercle, within the gutters, and threaded above the patella. (Figure 8)

We removed the wire about six months following repair. At that time, she had ROM for 0-95 degrees. At six years out following repair she walks with no ambulatory aids and has full extension. (Figures 9, 10A-C)

CASE EXAMPLE 2
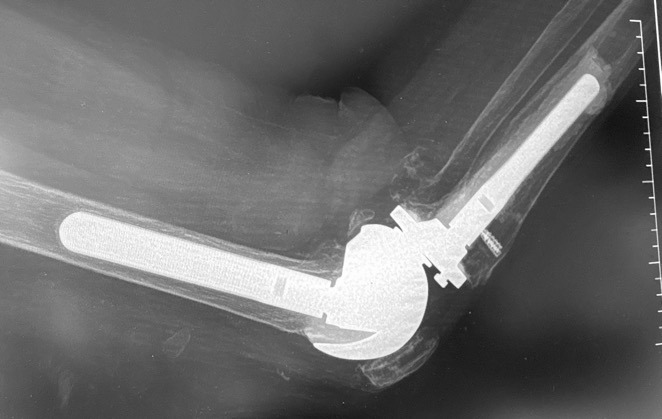
Case 2 is a 65-year-old woman with a previous oncological history and implantation with a TKA. Her knee became infected and required component removal and reimplantation with a rotating hinge. In 2013 she fell and tore patellar tendon and dislocated the patella. The patella was relocated, tear was repaired, and the protection technique used. (Figure 11A-B)
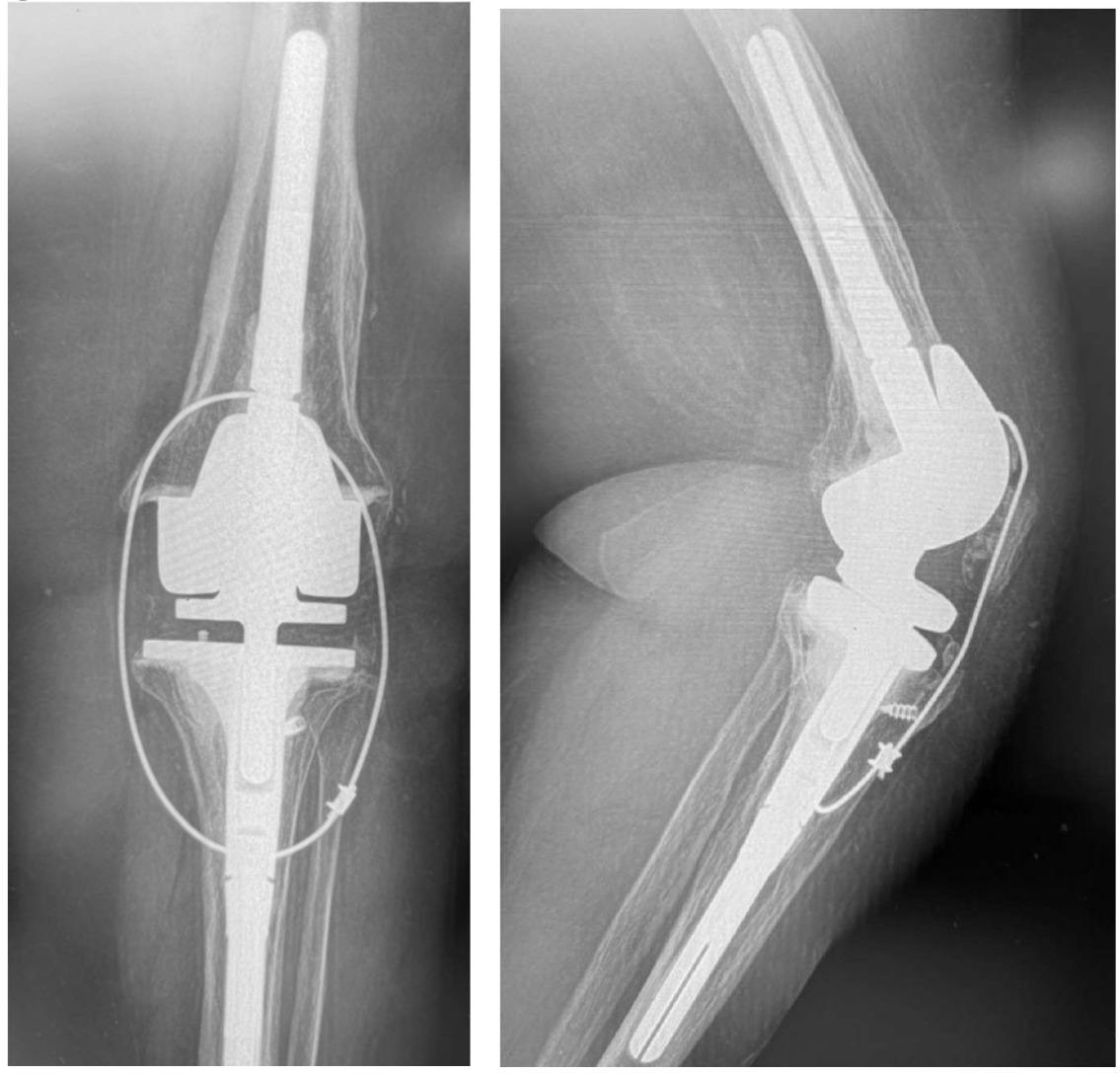
Her recovery was uneventful and was “doing great!” In 2015 (2-years following repair), she requested that the cable removed. Unfortunately, in 2016, she fell again and re-ruptured her patellar tendon. The rotating hinge was retained in place and the patellar repair / protection technique performed. She was recently seen in September of 2025 (9.5 years post second repair) and reports full independent activities of daily living (ADL) without ambulatory aids. She has a slight “lag” and weakness, so I requested that she use a cain when outside. She has ROM through 104 degrees, but that is due to the mechanical limits built into the rotating hinge device.
She did mention that she could feel the cable “a little bit.” But urprisingly, when I offered to remove it, she said to leave it as is.
After about 45 cable repair protection procedures performed, only 25% have had their wires removed. They usually say, “it doesn’t bother me, so leave it alone, I don’t want to do it.” And they maintain full ADL without issues. In addition, most all patients achieve 104-120 degrees extension (104 due to their rotating hinge), and 5 degrees or less lag. Which is far better than the unprotected repairs in the literature. We are currently reviewing all out cases and will prepare an article for peer-review publication consideration.
CONCLUSION
With this novel technique, we have a:
-
Reliable and reproduceable wire procedure for protecting patellar tendon repair efforts.
-
Rehabilitation schedule that avoids undo rapid tensioning of the tendon repair area.
Incorporating controlled ROM rehabilitation allows for protected and controlled stretching of the repaired tendon, allowing for complete healing, restoration of leg strength, and return to function.
The wire technique for protecting the patellar tendon rupture repair yields:
In my opinion, in “my hands” the use of the wire technique, with an extended and controlled post-operative period to protect the patellar rupture repair will result in increased outcomes independent of the repair method selected.