
.jpeg)
A few months ago, Dr. Buch called me and asked “Hey Chris, you know cones are expensive. Should we really be using them?” And I thought “that’s a pretty easy question.” We’re using cones all the time! We want to optimize fixation, but did it get me thinking, when should we be using cones in metaphyseal fixation? And what is the evidence? What are the finances behind it? You know really break it down.
Then I started asking myself several questions: What are the options? We have cones. We have sleeves. We even have OptiStem(TM)® (Link, Hamburg, DE) now. What type of knees should be getting fixation? What kind of bone defects? What about level of constraint are we putting in a PS constrained insert or doing a hinge? When do we when do we want to add fixation to that? And then what are the outcomes? Where the outcomes? What are the outcomes of not using metaphyseal fixation? Or more standard techniques like hybrid techniques? Do they do just as good without cones or with cones? And then kind of look at, you know, how do we really define the value of metaphyseal fixation?
Is adding metaphyseal fixation to revision TKA a "value additive?
-
What are the metaphyseal fixation options?
-
What type of patients and revision TKAs should we consider for metaphyseal fixation?
-
What are the outcomes of metaphyseal fixation?
-
What are the outcomes of NOT using metaphyseal fixation?
-
What is the cost of re-revision TKA?
-
What is the cost of adding metaphyseal fixation?
-
How do we define “value” of metaphyseal fixation devices in revision TKA?
I want to start with the last question, determining what’s the value of metaphyseal fixation? Some of the things I thought about would be clinical outcomes. What are the outcomes of using cones and not using cones, or sleeves, or other options? What are the actual costs of the implants? What are the costs of revisions and complications? And how do you mitigate your risk over time? Therefore, to have that value, we can define when we should use cones and when we shouldn’t.
Defining value in metaphyseal fixation in revision TKA
-
Clinical Outcomes: Improve longevity, decrease aseptic loosening, reduce revision rates.
-
Economic Costs: Implant costs, operative time, downstream resources (hospital stay, reoperation).
-
Time Horizon: The number of cones does it take to prevent a single revision (risk ratio or number needed to treat).
-
Risk Mitigation: Lower complications, subsequent increase in revision complexity, high risk patients.
This is a summary of my value statement for cones:
“In revision arthroplasty, the value of metaphyseal fixation can you find is the balance of clinical benefit relative to their cost over time in comparison to non-metaphyseal constructs.”
We now need to define which knees need metaphyseal fixation? Of course, not all revision knees are the same. Some have a little bit of bone loss, some have a lot of bone loss, so you can see there’s quite a bit of variety in these cases. And there’s different types of constructs. We’ve got sleeves, we’ve got sleeves with cones, we’ve got cones and cones, we’ve got OptiStem®, OptiStem® and cones, DFRs with metaphyseal cones, so there’s a lot of different options when we’re using metaphyseal fixation or anchorage.
We’re going to go back to our classification systems to help us be a little academic with this. The Anderson Orthopedic classification, obviously we have type one, two, and three (Engh and Ammeen 1999). Type I, there’s no defect; maybe in that setting it’s more like a primary Knee, and you may not need to use any metaphyseal fixation, but if you have a Type II defect or Type III, you have more bone loss, you might be considering metaphyseal fixation. However, there are some limitations to this classification system. Certainly, some can have very mild metaphyseal bone loss, and some can have very severe metaphyseal bone loss. So, type 2 could be quite broad spectrum of cases.
Anderson Orthopedic Research Institute Classification (Engh and Ammeen 1999)
- Type I: Minimal metaphyseal bone loss and intact cortical rim.
- Type II: Damaged metaphyseal bone with one or both condyles affected
- Type III: Major bone loss often with incompetent soft tissue (collaterals or patellar ligament)
And there’s also the revision classification from HSS (Scuderi and Weinberg 2022). And again, Type 1 has no bone loss but Type 2 has significant metaphyseal bone loss and beyond. So really once we have Type 2 defects in the primary setting or primary revision or the multiply revised knee, we have enough bone loss we may want to consider metaphyseal fixation.
The Classification of Tibial and Femoral Bone Loss with Stemmed Components (Scuderi and Weinberg 2022)
Tibia
-
Type 1: No bone loss, metaphysis and diaphysis intact
-
Type 2: Metaphyseal bone loss, the diaphysis intact
-
Type 3A: Extensive metaphyseal bone loss beyond the tibial tubercle and proximal diaphyseal bone loss
-
Type 3B: Extensive metaphyseal bone loss beyond the tibial tubercle and diaphyseal bone loss along the length with thinning of the cortex
-
Type 4: Extensive metaphyseal and diaphyseal bone loss with thinning and expansion of the cortex
FEMUR
-
Type 1: No bone loss, metaphysis and diaphysis intact
-
Type 2: Metaphyseal bone loss, the diaphysis intact
-
Type 3A: Extensive metaphyseal bone loss beyond the metaphyseal flare and proximal diaphyseal bone loss
-
Type 3B: Extensive metaphyseal bone loss beyond the metaphyseal flare and diaphyseal bone loss along the length with thinning of the cortex
-
Type 4: Extensive metaphyseal and diaphyseal bone loss with thinning and expansion of the cortex
How about young patients?
Well, we know that studies of young patients have shown that they have a higher risk of failure and revision in the arthroplasty (Aggarwal et al. 2014). So, maybe we consider metaphyseal fixation in patients who have a lot of bone loss or in younger patients.
How about level of constraint?
This is a nice meta-analysis where they reviewed over 4 ,000 knees and they showed the survivorship of CCKs versus constraints are about the same (Stroobant et al. 2023). The challenge with this though is only five-year data, we don’t know the long term what the difference is.
How about zonal fixation and technique?
In a study published in the British Journal, the authors retrospectively reviewed 1,173 revision cases performed with the hybrid technique and reviewed the ones that failed (van Laarhoven et al. 2025). The ones that failed all had poor metaphyseal fixation and didn’t achieve zonal fixation. In this study, they suggested that we have high focus on metaphyseal fixation to optimize outcomes.
Therefore, patients who have:
-
At least an AORI Type 2 defect,
-
Who are younger,
-
Who may have a higher level of constraint,
-
Have been revised before and may have poor metaphyseal or joint line bone…
…Then metaphyseal fixation is something to consider.
How about techniques of fixation?
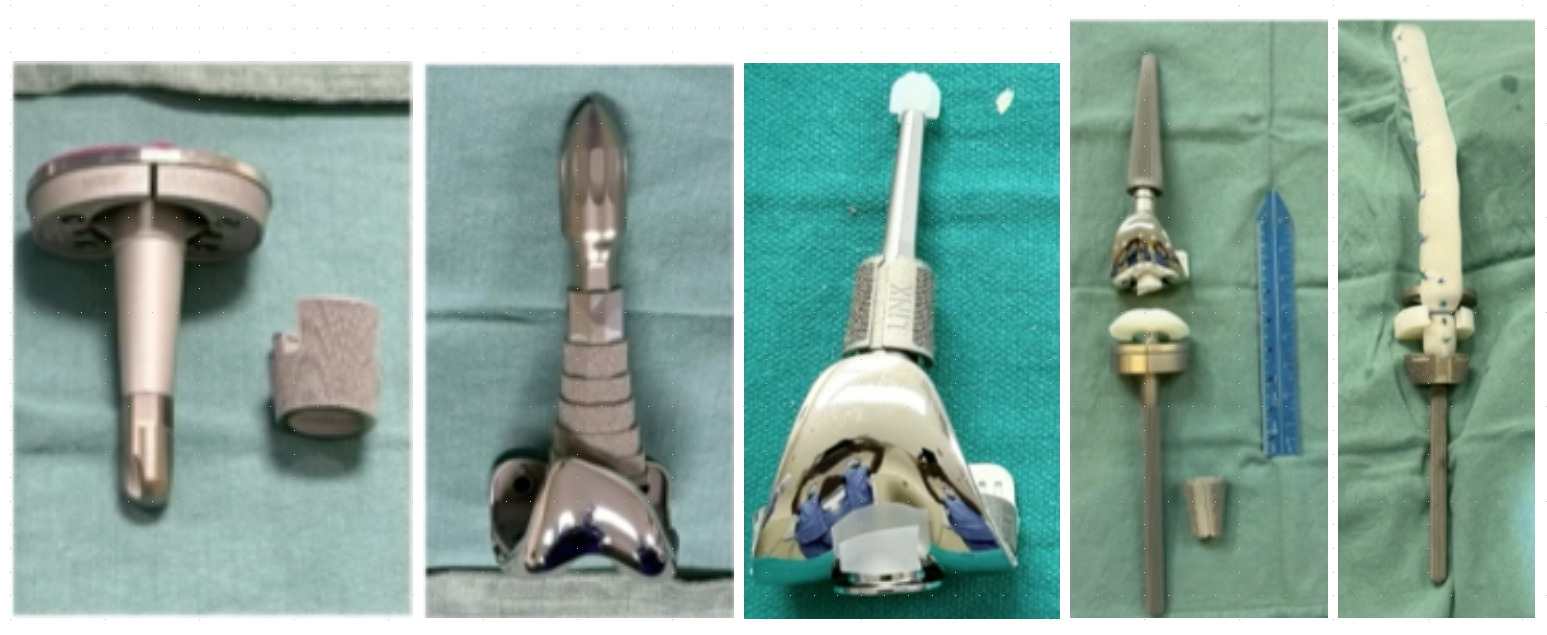
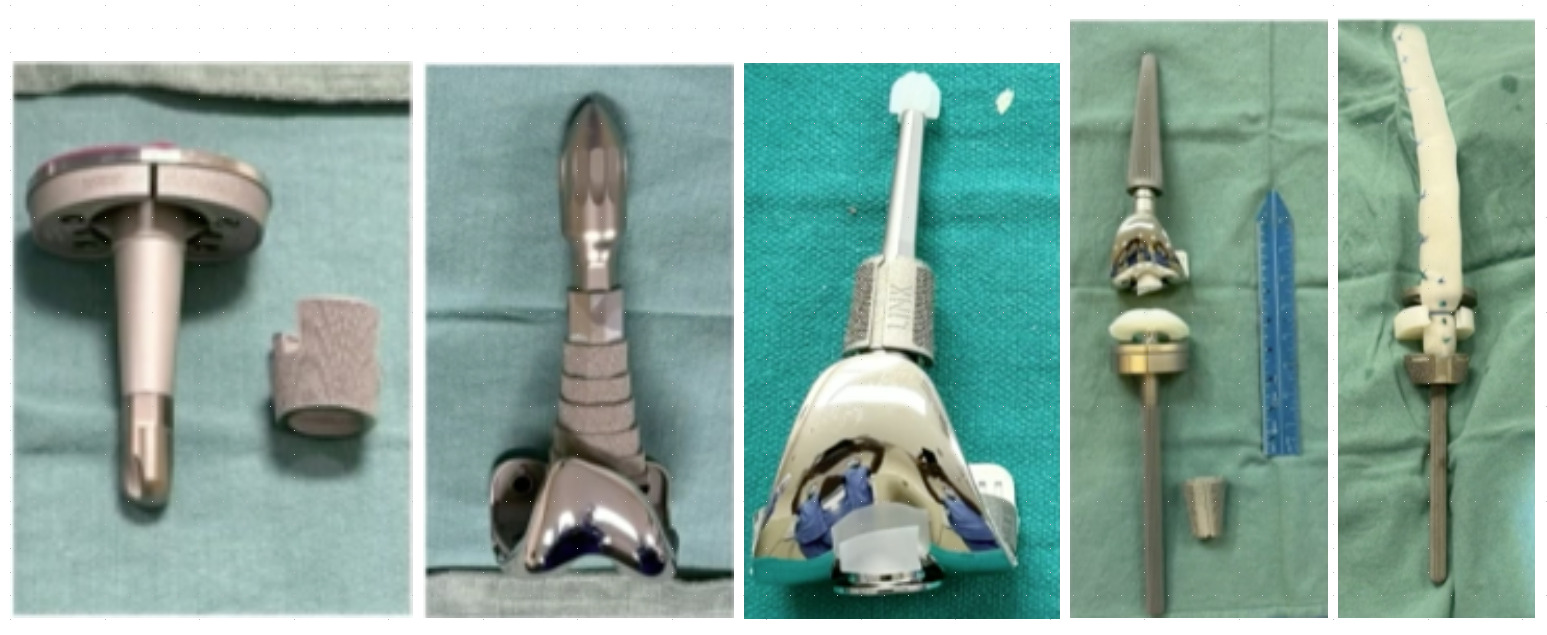
The techniques are different. We all know the “zone of fixation” is trying to get two zones of fixation in the revision setting (Morgan-Jones et al. 2015). A lot of times the joint line is gone, so we’re trying metaphyseal and diaphyseal fixation. We have all kinds of different techniques as we discussed, cone, sleeves, and let’s look at the data for some of these. (Figure 1)
How about sleeves?
Sleeves are kind of the first and have excellent data. This is probably the longest-term study I could find, 319 revision TKAs, 10-year survivorship, 97 .8 % survivorship with sleeves (Bloch et al. 2020). Another study of 152 revision TKAs at five-years follow-up, 99 % survivorship. Again, it’s more short-term data (Watters et al. 2017). And article from JAAOS reviewing all the studies for sleeves and again showing at least 95 % survivorship in sleeves from short-term to mid-term results (Siddiqi et al. 2021).
How about cones?
Cones have great biomechanical data. We know with finite element analysis the cones will decrease the bone force on the implant, or on the bone implant interface. By using a cone it can decrease that force to potentially improve the longevity of fixation, because you’re getting a biological fixation (Quevedo Gonzalez et al. 2021). And we’re also learning that short stems are equivalent. This is a nice biomechanical study done in JOA, and they basically compared all kinds of different scenarios, cemented stems, long, short, with and without cones (Guttowski et al. 2020). What they found was that for large defects cones with short, cemented stems have the largest pullout strength. Biomechanically we know that short, cemented stems with cones probably have the best pullout strength in biomechanical outcomes. This is another study reviewing long versus short stems (Xie et al. 2020). Adding a longer stem in these constructs doesn’t really help. It increases the chance of having pain at the end of the stem from the stress riser caused at the end of the stem. Therefore, short stems may be better in this setting. This is proven in this clinical study, although retrospective, this group compared short stems to long stems and they had equal survivorship (Batinica et al. 2022).
How about in the non-cone setting?
In this study, the authors retrospectively reviewed hybrid techniques with and without cones and they found no difference with cones (Bohl et al. 2018). The challenge here is that it’s only short-term follow up, two-year minimum, average three and a half years. The follow-up is too short. This is another study of 281 patients that underwent revision TKA with hybrid technique and 94 % survivorship at 10-years (Lim et al. 2023). This is another good study comparing hinged revisions, where they had fully cemented stems, hybrid technique, and then sporadically used cones with or without some of these (Lizcano et al. 2024). They retrospectively reviewed the data and found not much of a difference. However, the cones with a hybrid technique had the worst survivorship, while the rest were all somewhat similar.
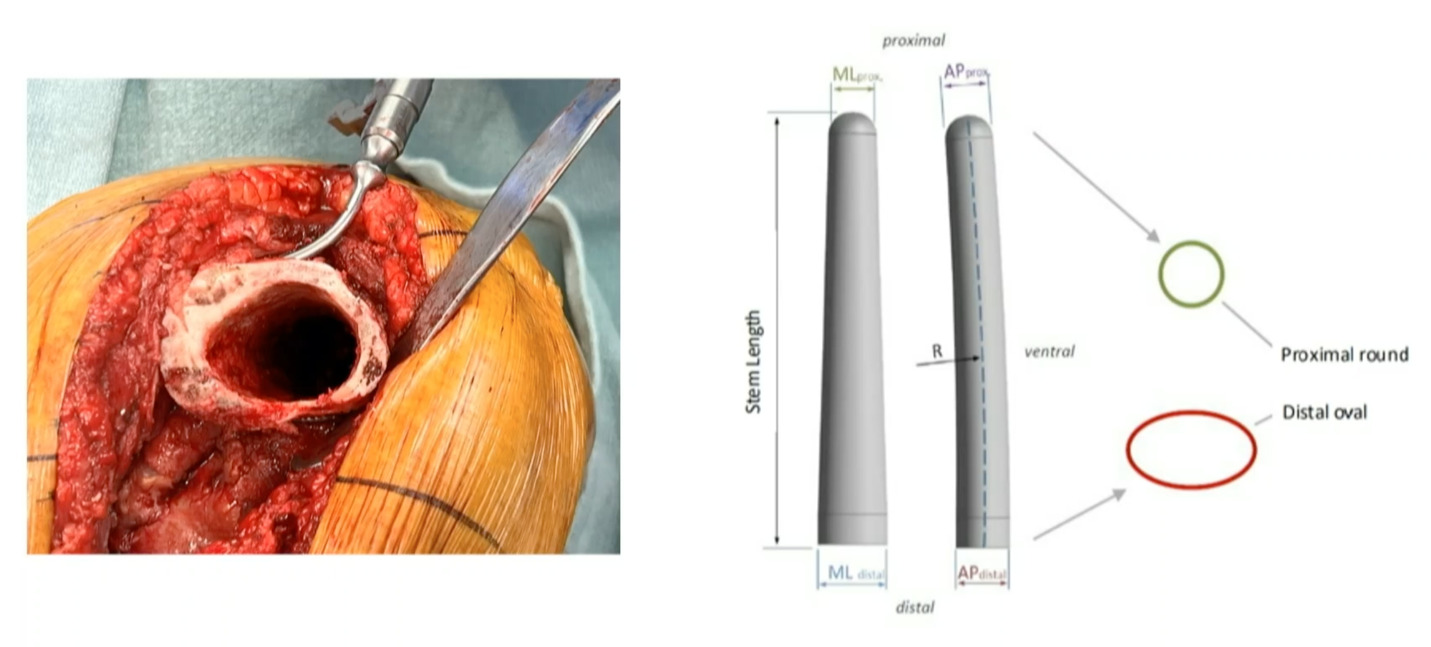
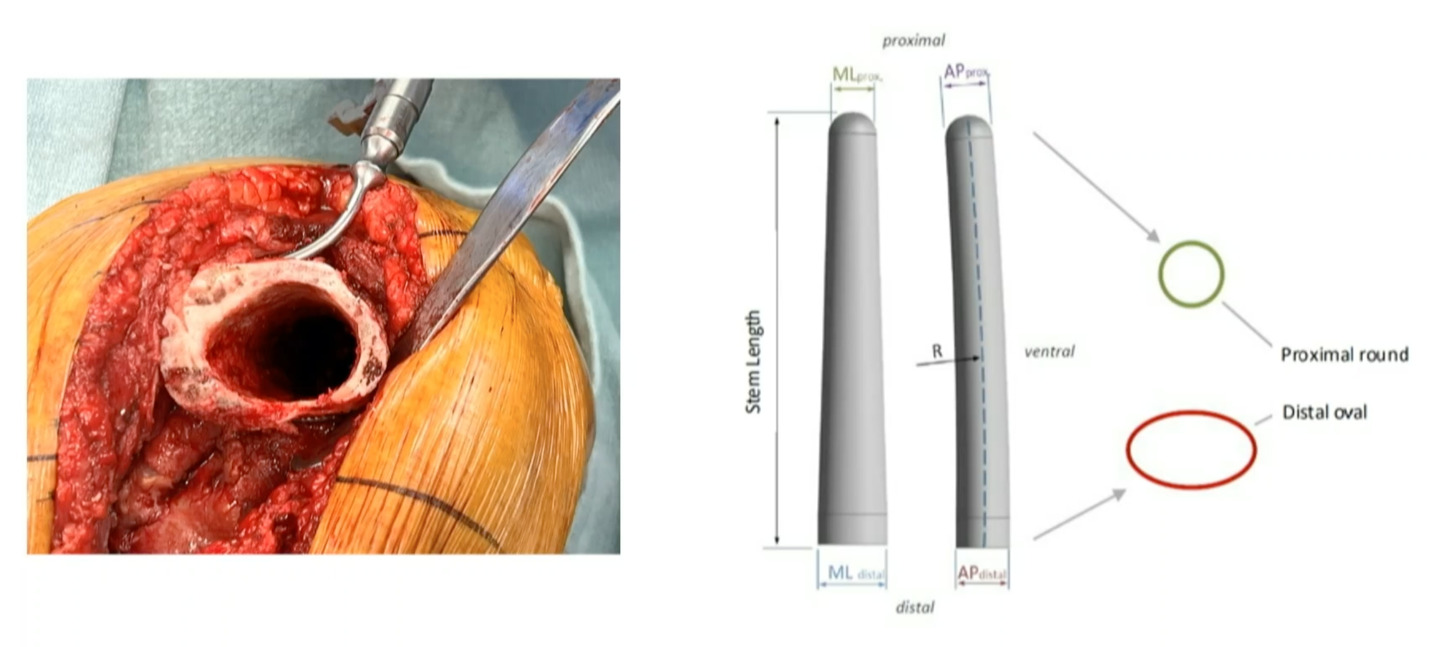
However, from our friends in Germany, Dr. Gehrke did a nice study reviewing 1,235 cases where they showed rotating-hinges and how they can fail (Levent et al. 2021). They found that a femoral diameter greater than 20 millimeters had higher loosening. When I spoke with Dr. Gehrke about this, he describes it as “it’s going to spin out.” You have a narrow-cemented stem and a big canal so it can create rotational forces in which the implant may loosen. We’ve learned with the OptiStem that having more rotational control can help improve fixation. This is a case from the distal femoral replacement (DFR) that we did, and you can see the shape of the bone. (Figure 2) So having a fluted stem that matches and marries the shape and morphology of the femur by improved fixation compared to a cylindrical cemented stem inside of a shell of cortical bone.
When we look back through the literature and what we see:
-
All retrospective
-
Lacks prospective RCTs
-
Institutional bias
-
Good clinical outcomes for BOTH metaphyseal and non-metaphyseal fixation
-
Majority of the information is short- and mid-term
-
Biomechanics studies favor metaphyseal fixation
However, I would say the biomechanical studies favor with short, cemented stems.
How about cost?
There’s not a lot of good data out there. This is the best study I could find, 2006, almost 20 years old, but the average cost of a revision surgery is about $74,000 (Lavernia et al. 2006). If you do a hinge, it goes up to $135,000. But, if you can prevent one of these, you’re probably saving money in the long run. Then this is another database study showing that by 2030, the cost of revision knee surgery is estimated to total $13-billion cost to the to our society (Bhandari et al. 2012). Again, preventing revisions and improving long-term fixation are important. How about the cost of adding a cone well? This is complicated. It’s institutionally based. Everyone’s got different costs that are “brand specific.” At our institution, when adding a cone to a standard revision construct, say a short cement stem and one cone, adds about 20% additional cost to the implant.
How about centralization of care?
Implants are expensive and they are institutionally based, but places that do high volume can probably get better pricing (Ramirez et al. 2022). So maybe centralization of care can improve the cost of metaphyseal fixation revisions in general.
Let’s revisit our value statement. Our question is, “is metaphyseal fixation worth it?” I think it’s very complicated. But I think in general, those who have bone loss, Type 2 defects, those who are high risk for loosening, like younger patients, more constrained implants, hinges, then you may want to consider metaphyseal fixation. We know that biomechanical studies show they have the best outcomes, but the clinical data is not perfect yet. We need better studies. “Is it wrong not to use metaphyseal fixation?” No. I think it’s very reasonable, and you can expect to get good mid- to long-term outcomes with a standard hybrid technique. And then, as a system, we probably need to figure out more cost-effective ways to improve access to revision the implants and improve the economic outcome with these.