INTRODUCTION
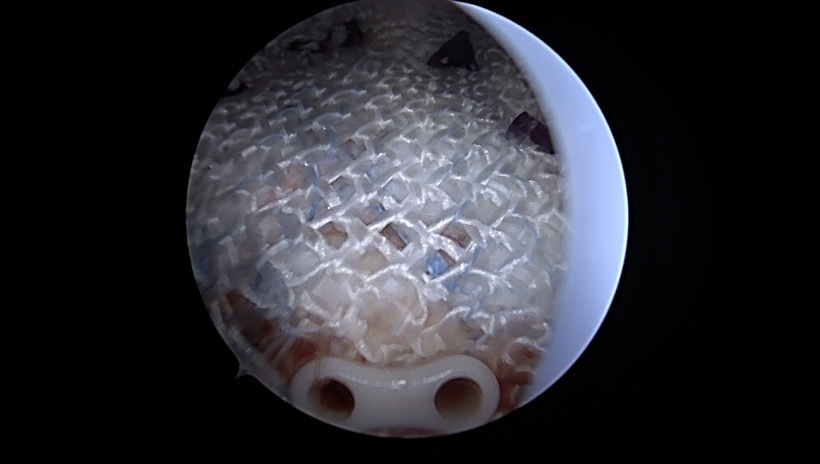
Arthroscopic rotator cuff repair outcomes continue to be static over decades in the orthopaedic literature as it relates to recurrent tears on postoperative imaging (Chona et al. 2017; Rashid et al. 2017; Hein et al. 2015; Galatz et al. 2004). Failure rates remain relatively high, ranging from 20-90% in some studies (Chona et al. 2017; Rashid et al. 2017; Hein et al. 2015; Galatz et al. 2004). Mode of failure can occur as a result of failure of anchor (displacement), tearing of the tendon through sutures (Type I tears) or new tears medial to the repair (Type II tears) (Cummins and Murrell 2003; Sugaya et al. 2007; 2005; Cho et al. 2010). Recent efforts have been made to reduce failures after RCR by introducing augmentation with a scaffold, matrix, graft, or patch that may improve the tendon’s healing potential and structural integrity, with specific focus on increasing rotator cuff thickness and restoring the native footprint (Bokor et al. 2016; Cheesman et al. 2022; Zhang et al. 2023; Romeo et al. 2022; Chalmers et al. 2013). Acellular allograft dermal matrix has the longest and most abundant literature to support its use and reduction in failure after rotator cuff repair but implantation is commonly felt to be a difficult procedure (Chalmers et al. 2013). Other implants utilize xenograft collagen for their patch, however, given historical data regarding xenograft use, this has deterred some surgeons from utilizing this in human patients (Bokor et al. 2016; Zhang et al. 2023; Iannotti et al. 2006; DeCarbo et al. 2010). In addition, two recent reports have identified foreign “rice body” reactions with these xenograft bovine collagen implants (Barad 2019; Root et al. 2023). Other implants have only shown benefit at the bone tendon junction and would not necessarily reduce the possibility of Type II tears (Romeo et al. 2022).
Hyaluronic Acid (HA) is a glycosaminoglycan (GAG) within the extracellular matrix that functions to lubricate and cushion synovial joints, but is also found through the body within the vitreous of the eye, dermis, and placenta/umbilical cord (Marinho et al. 2021). However, the biologic effects of endogenous HA may be even more important when considering therapeutic applications. At the molecular level, HA can mediate cell migration, proliferation, and differentiation via direct binding of cytokines (Shimpuku et al. 2007).
HA is primarily used for intra-articular injections within orthopaedics, however it has numerous current clinical applications including wound care, ophthalmology, and aesthetic dermatology (Huynh and Priefer 2020; Ferkel et al. 2023). The Integrity implant in our study is comprised of 20% polyethylene terephthalate (PET) (standard suture material) and 80% Hyaff, a solid form benzyl ester of HA that resorbs over a few months. Commonly used liquid HA rapidly degrades with a half-life ranging from minutes within the blood, to hours in skin, and several weeks within cartilage (Galatz et al. 2004; Cheesman et al. 2022). Hyaff has been used for more than two decades in cartilage restoration surgery, demonstrating safety and efficacy in human use (Gobbi et al. 2020; Marcacci et al. 2005). It has been shown in dermal wounds that HA grafts decrease average wound closure time by 85% compared to control groups and reduce TGF-β1 expression, thus reducing scar tissue formation (Hu et al. 2003).
The purpose of this study was to collect early safety and efficacy data as well as characterize early postoperative imaging in a small series of patients undergoing arthroscopic repair of partial or full-thickness rotator cuff tears augmented with the Integrity Implant System – a novel, resorbable, HA based patch. It was hypothesized that there would be incorporation of the graft with thickening of the tendon on MRI along with improvement in patient-reported outcomes (PROMs) without complications at 3 and 6 months postoperatively.
METHODS
Study Design/Participants/Setting: This retrospective, observational study included a series of 10 adult patients from a single surgeon’s practice. All patients underwent rotator cuff repair (RCR) with the use of a hyaluronic acid (HA) patch for either full-thickness rotator cuff tears (FT-RTC) or partial-thickness rotator cuff tears (PT-RTC) in an ambulatory surgical setting. Exclusion criteria included massive or irreparable cuff tears, previous shoulder surgery, claustrophobia, insufficient follow-up, and significant preoperative shoulder stiffness. Massive RTC tear was defined as tendon retraction to the glenoid rim, or over two-thirds of the greater tuberosity footprint exposed on the sagittal MRI (Schumaier et al. 2020). Stiffness was defined as glenohumeral abduction or forward flexion less than 90 degrees, or more than 25% decrease in external rotation relative to the contralateral side. PT-RTC patients underwent an “Onlay” repair, where the HA patch was secured directly over the injured tendon without formal suture repair. FT-RTC patients received standard rotator cuff repair (RTCR) according to the surgeon’s established technique (transosseous equivalent “double row repair”), followed by augmentation with the HA patch applied to the bursal side of the repair. The HA graft was carefully positioned over the greater tuberosity, lateral to the bone-tendon junction, and extended medially to the suture of the medial row anchors (Figure 1).
Surgical Technique: All surgeries were performed with the patient in the lateral decubitus position, with a hydraulic arm traction device (Spider Arm Holder, Smith & Nephew). Interscalene block anesthesia was administered preoperatively by the anesthesia staff using ultrasound guidance and bupivacaine. For PT-RTC repairs, the “Onlay” technique was utilized, with the HA patch placed directly over the injured tendon without formal suturing. FT-RTC patients underwent the standard double-row repair technique, with HA patch augmentation applied after the repair to the bursal aspect of the tendon.
Postoperative Rehabilitation: Postoperative physical therapy protocols were standardized for both PT-RTC and FT-RTC patients.
-
PT-RTC Tears (Onlay Repair): Patients were allowed to remove their sling on postoperative day (POD) 3 and begin hand, wrist, and elbow range of motion (ROM) exercises, including pendulum swings and table slides. Abduction and overhead elevation were restricted until 6 weeks postoperative. Resistance training in internal and external rotation with the arm at the side began at 6 weeks. At 3 months after achieving full ROM, gentle resistance exercises in all planes were allowed.
-
FT-RTC Tears (Augmentation): Postoperative rehabilitation for FT-RTC patients followed the surgeon’s standard protocol. Patients were instructed to wear a sling for 6 weeks during sleep and when leaving home. Hand, wrist, and elbow ROM exercises were initiated POD 3. Pendulum swings and table slides were started at 2 weeks. At 6 weeks, passive range of motion (PROM) progressed to active-assisted range of motion (AAROM), and then active range of motion (AROM) exercises were performed in a supine position. Normal activity with a 5 lb weight limit was allowed after 3 months. Resistance training was progressively increased at 3 months after achieving full ROM.
Variables
Outcome Measures: Preoperative and postoperative patient-reported outcome measures (PROMs), including the American Shoulder and Elbow Surgeons (ASES) score, Single Assessment Numeric Evaluation (SANE), and Patient-Reported Outcomes Measurement Information System (PROMIS) scores, were collected 3 and 6 months postoperatively.
MRI Assessments: MRI evaluations were conducted preoperatively and at 3 and 6 months postoperatively. The scans were performed on 3 Tesla MRI scanners at two institutions, using 2 mm slices, proton density (PD) and T2-weighted sequences, both with and without fat saturation. All images were reviewed by senior orthopaedic faculty and then independently confirmed by a fellowship trained sports and shoulder orthopaedic surgeon. The MRIs were used to assess the integrity of the repair, tendon thickness, and restoration of the rotator cuff footprint. The supraspinatus tendon thickness was measured on a modified coronal plane at the center of the tear (anterior-posterior), tilted slightly anteriorly, just lateral to the articular margin of the supraspinatus insertion (Bokor et al. 2016). Thickness measurements were compared to published ultrasound data for males and females to assess new tissue generation. Restoration of the rotator cuff footprint was assessed based on MRI findings at the 6-month mark. The footprint area was considered fully restored if the imaging demonstrated tendon-like tissue occupying the entire footprint.
Data Sources/Management/Statistical Methods: Descriptive statistics were used to summarize patient demographics and PROMs at each time point. Changes in tendon thickness and footprint restoration were analyzed using the preoperative and postoperative MRI data. T-tests were utilized to compare preoperative with 3 and 6 months postoperative cuff thickness and PROMs in order to evaluate the functional outcomes and healing response. Statistical significance was set at an alpha level of 0.05.
Ethical Approval and Patient Consent: This study was conducted in accordance with the ethical principles mentioned in the Declaration of Helsinski (2013). Retrospective chart review is IRB exempt at our institution. All patient data was studied and published in a deidentified manner. Dr. Baker obtained informed consent prior to performing surgery on all of the patients included in the study.
RESULTS
Participants/Descriptive Data
Between January 2024 and August 2024, 30 patients elected to undergo RCR with the use of the Integrity Implant System by the senior author for either “onlay” or “augmentation” repair. 15 had sufficient follow up and PROM data, and 10 patients agreed to postoperative MRI evaluation. Among these, 4 patients underwent “onlay” repair for partial-thickness rotator cuff (PT-RTC) tears or myotendinous tearing, and 6 patients underwent “augmentation” repair for full-thickness rotator cuff (FT-RTC) tears (Figure 1). There were 4 male and 6 female patients, with the average age and BMI of 52.8 years and 26.5 (n=6), respectively. Demographics and medical comorbidities are listed in Table 1.
MRI Findings
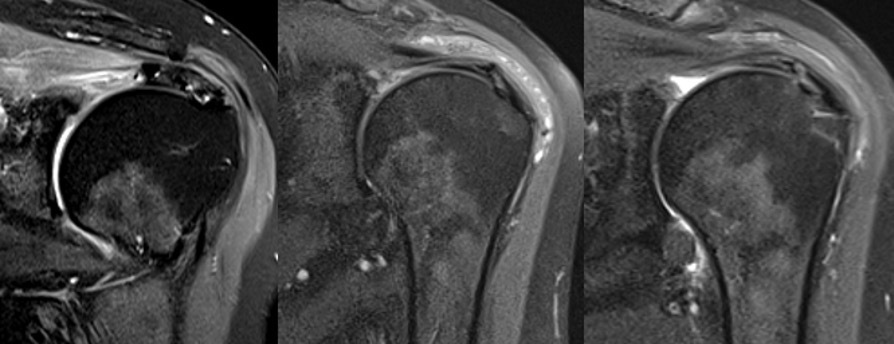
Preoperative RTC tear type and dimensions are listed in Table 2. At both 3 and 6 months postoperatively, each patient underwent MRI evaluation of the affected shoulder. No recurrent rotator cuff tears, failure of the repairs, or effusions were identified (Table 2). The rotator cuff footprint was restored in each case (Table 2). All patients showed early tissue reactions at the 3-month mark in the subacromial space, with thickened tissue corresponding to the area where the HA patch had been placed. By 6 months postoperatively, the amount of reactive bursal tissue and edema had decreased, and the tendon-like tissue continued to organize, maintaining its thickness. All full-thickness RTC tears (n=6) as well as all four “onlay” procedures (n=3 partial thickness, n=1 myotendinous) were healed by 6 months (Table 2). The average tendon thickness at 3 months postoperatively was 7.63 ± 1.30 mm, and by 6 months, it remained stable at 7.61 ± 1.03 mm, both significantly increased from preop thickness of 4.77 ± 0.67 (p<0.001) (Table 3). These findings suggest successful integration of the HA patch and healing of the repaired tendon.
Clinical Outcomes
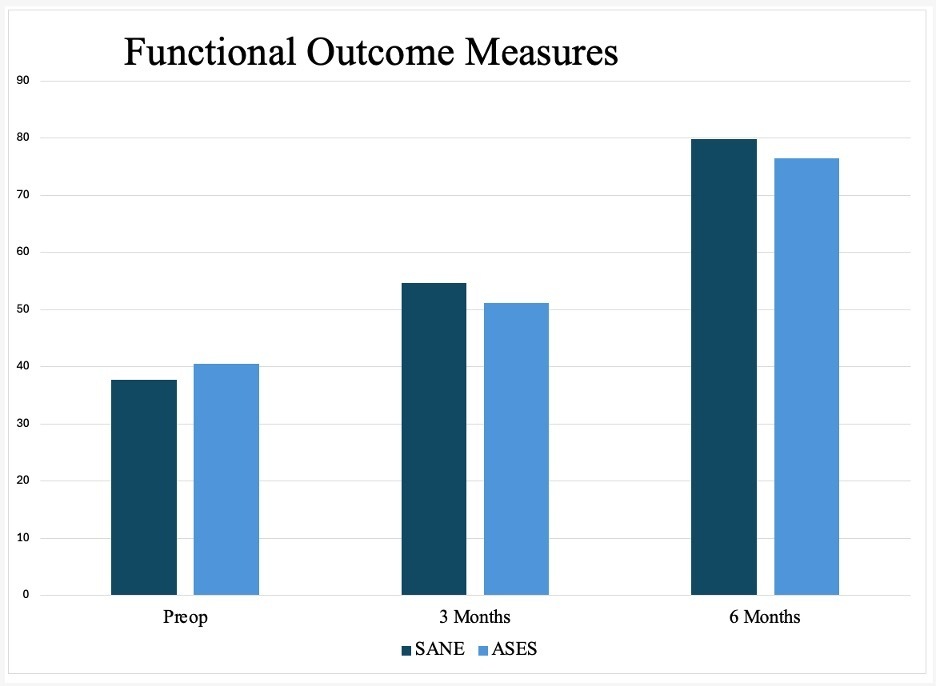
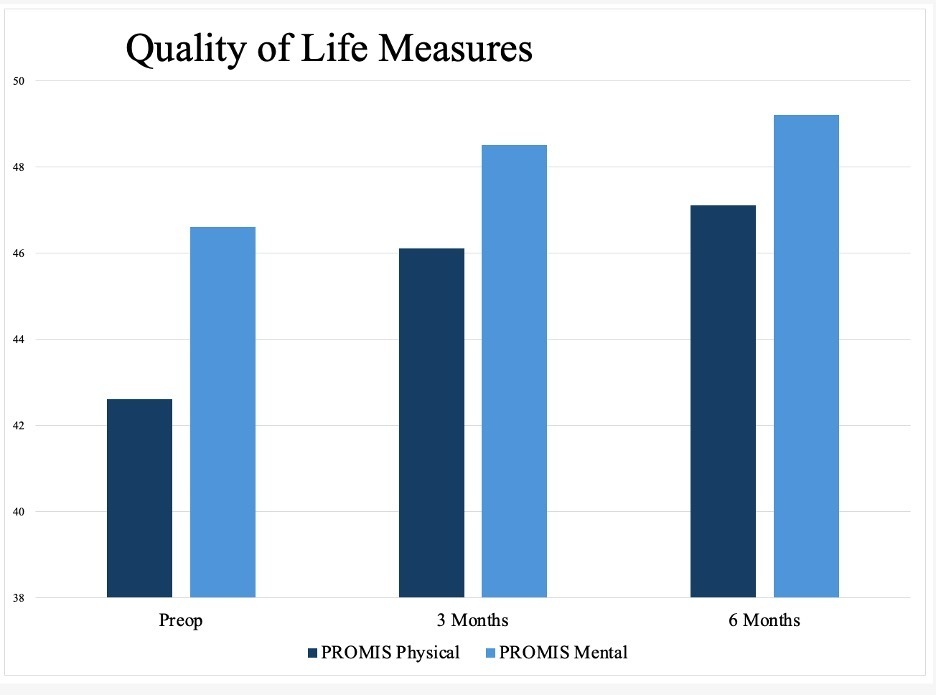
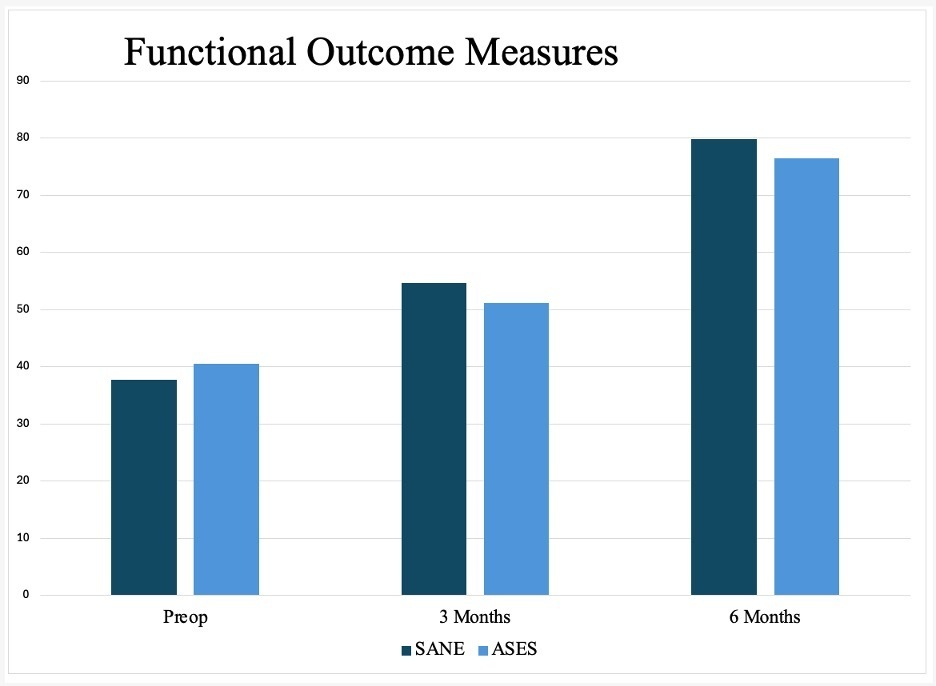
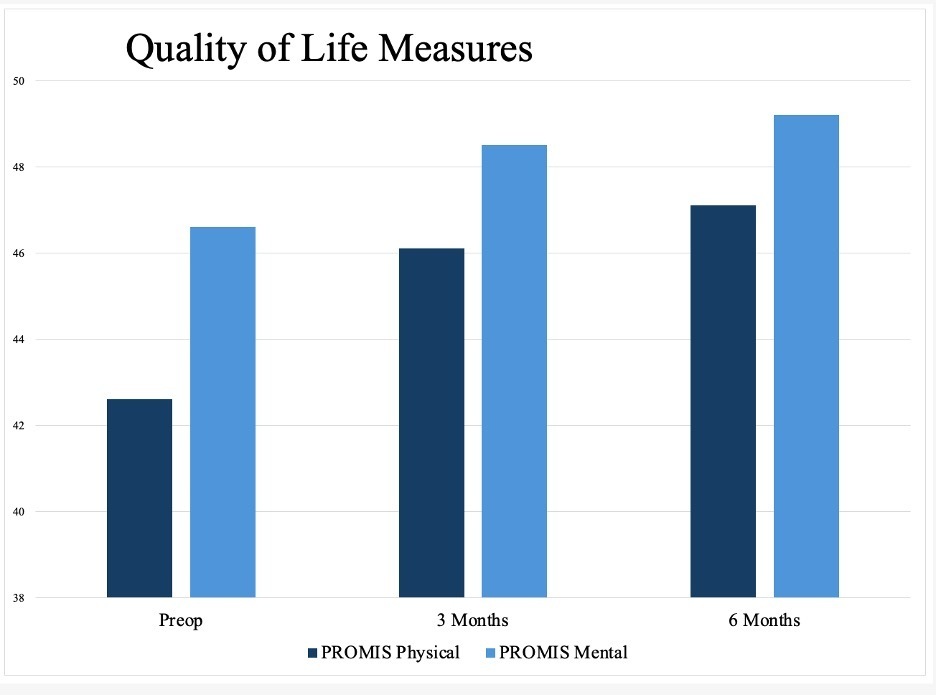
Consistent and statistically significant improvements were observed at 3 and 6 months postoperatively. The American Shoulder and Elbow Surgeons (ASES) score improved from a preoperative mean of 40.5 ± 10.6 to 76.5 ± 16.1 at 6 months (p<0.001). The Single Assessment Numeric Evaluation (SANE) score increased from 37.7 ± 15.2 preoperatively to 54.6 ± 11.9 at 3 months (p=0.013) and 79.8 ± 8.5 at 6 months (p<0.001). Additionally, PROMIS Global Physical Health scores increased from 42.6 ± 8.6 to 47.0 ± 7.6 at 6 months (p=0.004), and PROMIS Global Mental Health scores improved from 46.6 ± 14.0 to 49.2 ± 13.7 (p=0.156). These results indicate increased clinical benefit and functional recovery (Table 4, Figures 2 and 3).
Adverse Events and Complications
No patients experienced any adverse reactions during the study period. There were no complications or reoperations, indicating that the procedure with HA patch augmentation was safe and effective for the cohort studied for 6 months postoperatively.
DISCUSSION
Key Results
Our study demonstrated early safety and efficacy of the first HA based rotator cuff graft with improvement in all PROMs and no complications. Postoperative MRI showed healed RTC, footprint restoration, and significantly increased tendon thickness similar to a popular Bovine patch (Bokor et al. 2016; 2015). Subacromial reactive changes were seen in all patients at 3 months and resolved with tendinous incorporation and thickening by 6 months (Tables 2 and 3). Although this is very early follow-up, it is important to ensure this new technology is both safe and effective, as there have now been more than 1000 surgical implantations throughout the US (Baker 2025).
Early PROMs and imaging provide evidence that the implant is performing as expected in vivo. ASES scores in our study improved from a preoperative mean of 40.5 ± 10.6 to 76.5 ± 16.1 (p<0.001) at 6 months follow up, which is similar to PROMs documented for another mainstream bovine collagen patch that reported improvement from 44.6 to 87.8, albeit this was at 2 years postoperatively (Bokor et al. 2016). Similar functional improvements have been documented for both full thickness and partial thickness RTC tears (Bokor et al. 2016).
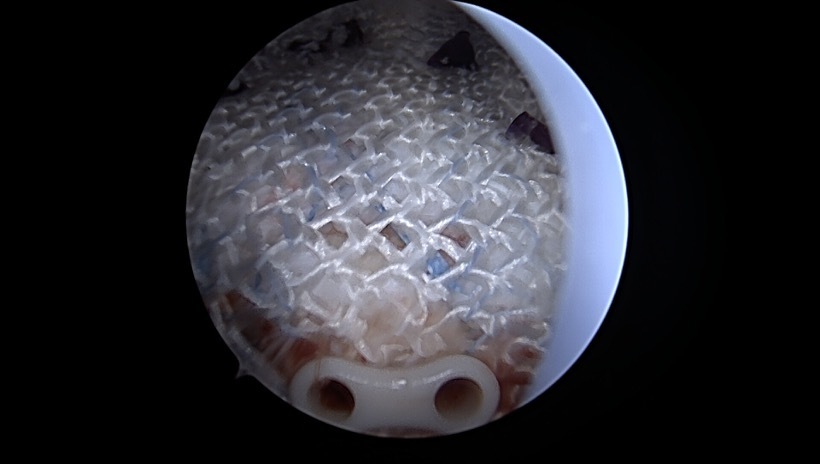
Thickening of the rotator cuff tendon either by healing of the tendon itself or by integration of tendon-like tissue is felt to be the main benefit of supplementing RTC repairs with a bursal sided patch (Bokor et al. 2016; 2015). It has been the senior author’s experience that the use of various synthetic and biologic graft augmentations in RTC repair leads to early postoperative reactive “inflammatory like reactions” in the subacromial space. A previous study on the Integrity Implant System in an Ovine model showed progressive implant degradation along with fibroblast neocollagen deposition, and fiber-like organization around the PET component within the RTC throughout the 26 week study (Badylak 2023).
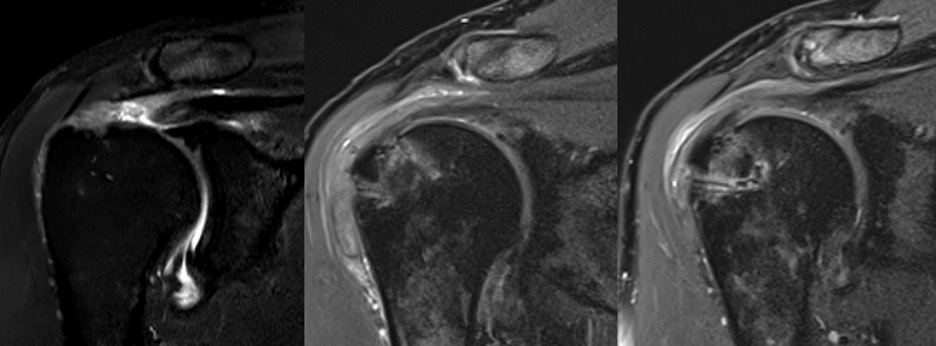
This study revealed similar reactive subacromial changes on postoperative MRI, which likely reflects the graft’s biodegradation and cell mediated immune response corresponding to T2 edema on MRI at 3 months postop (Figures 4 and 5). However, there was ultimate thickening and consolidation of this edematous area into low signal tendon-like tissue in the RTC at 6 months, which may indicate a completed healing response, and partial degradation and structural incorporation of the graft. This study also shows similar thickening and healing of both partial thickness and full thickness RTC tear patients, with ultimate consolidation into a single continuous tendon complex. Previous studies measuring RTC tendon thickness after repair in the absence of patch augmentation most commonly show reduced tendon thickness compared to preoperative ipsilateral as well as contralateral measurements (Kjaer et al. 2024; Crim et al. 2010; Tham et al. 2013). However, one study reported a small proportion of patients did undergo tendon thickening compared to preoperatively (Crim et al. 2010). It was felt important to characterize the expected imaging characteristics of the HA patch in short intervals of 3 and 6 months postop to inform physicians of the thickened subacromial appearance and investigate tendinous healing and graft incorporation radiologically. We reported significant increase in average tendon thickness from 4.77 ± 0.67 mm to 7.63 ± 1.30 mm at 3 months (p<0.001), and 7.61 ± 1.03 mm at 6 months (p<0.001), which is similar to published data for a commonly used bovine collagen patch that reported mean tendon thickness at 6 months postop as 7.6 mm for men and 7.0 mm for women (Bokor et al. 2015). This is noticeably thicker than ultrasound measured supraspinatus thickness at the same timepoint, being 5.6 mm for men and 4.9 mm for women on average (Karthikeyan et al. 2014).
_t2_coronal_mri_sequences_of_a_patient_w.jpg)
_t2_coronal_mri_sequences_of_a_patient_w.jpg)
The rotator cuff footprint on the greater tuberosity has been recently highlighted in the literature due to its impact on RCR outcomes. Research has shown that re-tear is associated with poor tendon quality and lack of footprint coverage (Ahmad et al. 2015). Both tension free repair and having an anatomic footprint is ideal for tendon-to-bone healing, however, this may not always be possible with massive or retracted tears, hence why these were excluded in our study (Xiao and Abrams 2025). Most recurrent tears and repair failures occur within 6 months postoperatively, underscoring the importance of optimizing biology and biomechanics to prevent complications. Restoring normal footprint architecture reduces insertional cuff strain during early healing, and our study shows augmenting such with a HA-based patch improve RCR integrity and potentially patient outcomes.
Limitations
There are multiple limitations in the current study, primary related to the small sample size and short follow-up time. The single surgeon nature may also limit external validity. Additionally, our statistical power is limited given 10 of the 30 available patients had inadequate follow up. Five of the remaining 15 patients did not consent to postoperative MRI without citing specific reason. Although anecdotally these five patients were clinically recovering well, their exclusion is a significant limitation. We felt it important to publish preliminary safety and efficacy data on this implant given that it is already being clinically implanted nationwide, and that there is a multicentered prospective cohort study enrolling to capture over 150 patients at 8 sites. This is the first HA patch used in human RCR and the information in our study can be built upon in future research to guide surgical decision making and improve patient care.
Another limitation is selection bias given that this was not a randomized study of all implant usages or RCR surgeries. However, surgeons may benefit from understanding the clinical outcomes and early MRI appearance for more common indications and RCR surgeries with higher likelihood of successful repair. Outlier cases may lead readers to draw inappropriate conclusions or make errant clinical decisions based off postoperative imaging that they feel is abnormal, potentially leading to unnecessary procedures and morbidity.
CONCLUSION
The Integrity HA based patch implant demonstrates both safety and efficacy in the surgical management of both partial and full-thickness rotator cuff tears at 6 months. Outcomes appear to be comparable for both partial and full-thickness injuries, showing thickening of the RTC without recurrent tearing. Consistent improvements in PROMs and footprint restoration on MRI was confirmed for all patients.
FUNDING
Anika Therapeutics, Inc. covered IRB fees and postoperative MRIs for patients.
DATA AVAILABILITY
All original data for this study are available upon request.
AUTHORS’ CONTRIBUTIONS
AM: data analysis, manuscript writing; RP: data analysis, manuscript writing; EC: manuscript writing; HC: data collection, data analysis; VS: data collection; CB: primary investigator, manuscript writing.