

Introduction
Medial patellar instability is a clinically significant condition that can be associated with disabling pain and mechanical symptoms (Moatshe, Cram, et al. 2017; Hughston and Deese 1988). Lateral subluxation due to medial patellofemoral ligament (MPFL) injury or insufficiency is far more common and has been thoroughly reported and described in the literature. The soft tissue constraints of the lateral knee are less understood, with the current conception highlighting a lateral patellofemoral complex comprised of numerous soft tissue structures (Kerzner et al. 2023). Of these structures, the lateral patellofemoral ligament (LPFL) and iliotibial band extension to the patella are considered the primary restraints to medial patellar subluxation, especially within the first 30 degrees of knee flexion (Kerzner et al. 2023; Shah et al. 2017). The predominant cause of medial patellar instability reported in the literature is iatrogenic compromise of these ligaments following surgical lateral retinacular release. Other less common iatrogenic causes can include detachment of the vastus lateralis muscle from its patella insertion, previous medial tibial tubercle osteotomy, or an overtightened MPFL graft (McCarthy and Bollier 2015). While most medial patellar instability cases are iatrogenic, there are a few case reports describing traumatic cases, and even fewer describing idiopathic cases (McCarthy and Bollier 2015; Shannon and Keene 2007; Borbas et al. 2014; Saper and Shneider 2014; Richman and Scheller 1998; Hughston et al. 1996). We report a case of a 32-year-old woman who presented with medial patellar instability without prior surgery or traumatic injury.
Presentation of Case and Surgical Technique
History
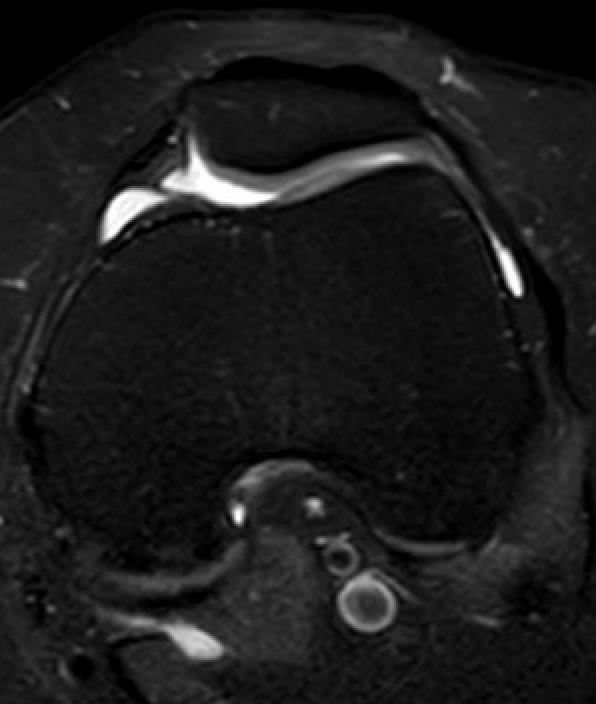
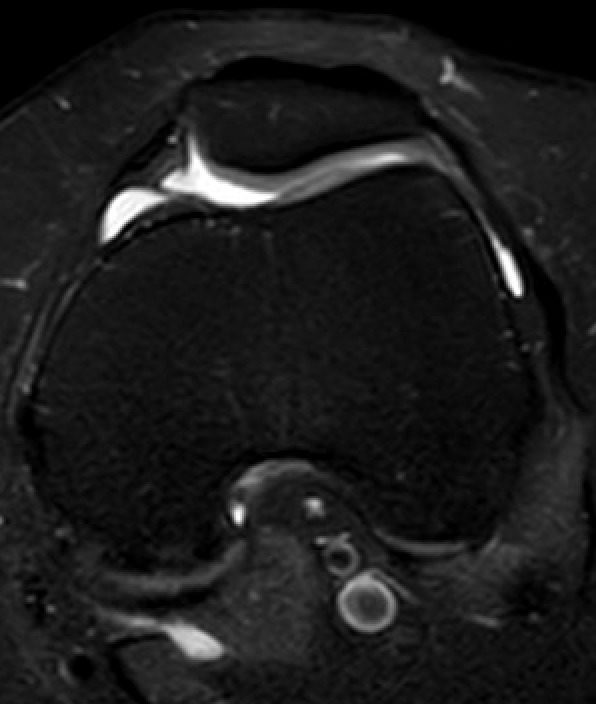
Our patient is a 32-year-old woman with a long-standing history of patellar instability. She had reported medial patellar dislocations for almost 20 years and initially discussed surgical management as a child but never followed up. At the time of evaluation, she was having daily dislocations with walking, lying in bed, and slight twisting of her leg, which she was self-reducing for several years. The patient experienced pain for a short period of time after dislocations. Her instability was unresponsive to conservative measures with physical therapy and reverse J bracing. Radiographs of the knee did not demonstrate any trochlear dysplasia, degenerative changes, or patella malalignment. Magnetic resonance imaging (MRI) of the knee revealed slight lateral patellar mal-tracking without any trochlear dysplasia (Figure 2). Her past medical history was notable for polycystic ovarian syndrome (PCOS), post-traumatic stress disorder (PTSD), and fibromyalgia. She had no prior orthopedic surgeries.
_anterior-posterior__b)_merchant_and_c)_lateral_radiographs_of_the_patient_s_left_knee__.png)
Examination under anesthesia
The patient’s full range of motion was -8 of hyperextension to 130 degrees of flexion. She demonstrated 3 quadrants of medial patellar translation versus 2 quadrants laterally in 30 degrees of knee flexion. The patella was able to be dislocated medially from full extension to full flexion (Supplemental Video 1).
Procedure
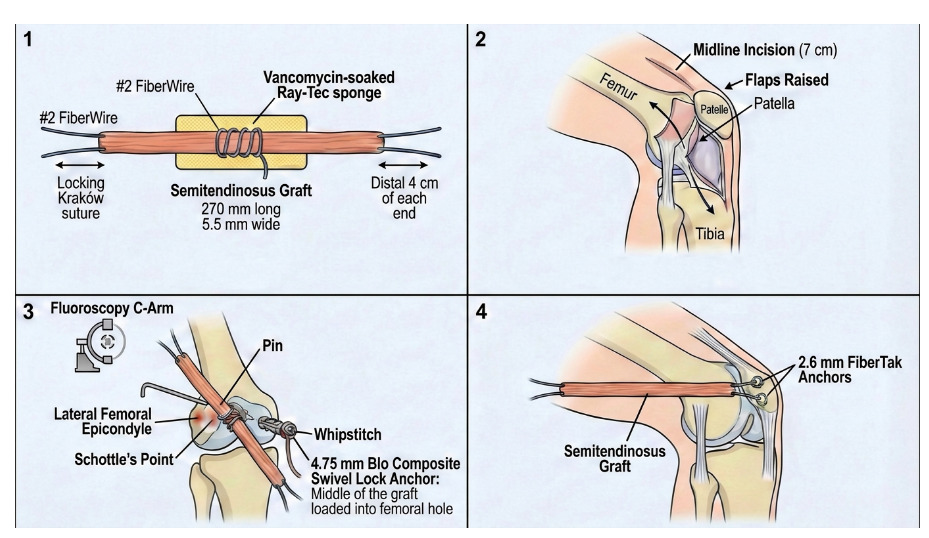
The semitendinosus allograft was first prepared on the back table. A locking Kraków suture was placed at its midway point and at the distal 4 cm of each end with a #2 FiberWire. It was then tensioned and covered with a vancomycin-soaked Ray-Tec sponge. It was measured to be 270 mm long and 5.5 mm wide
The leg was then exsanguinated and the tourniquet inflated. A midline incision was made that was 7 cm in length over the patella starting just proximal to the patella. A flap was raised over the lateral retinaculum, and this was then incised until the synovial layer was identified. The joint was not entered. Small flaps were raised just above layer 3 of the lateral knee, identifying the retinaculum and deep layer underneath using Metzenbaum scissors. The retinaculum was dissected out for later repair.
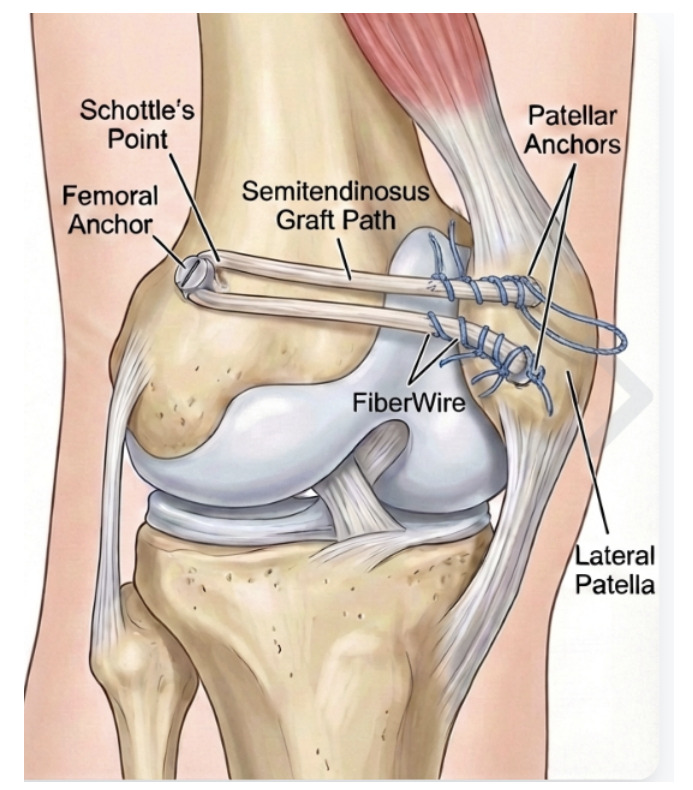
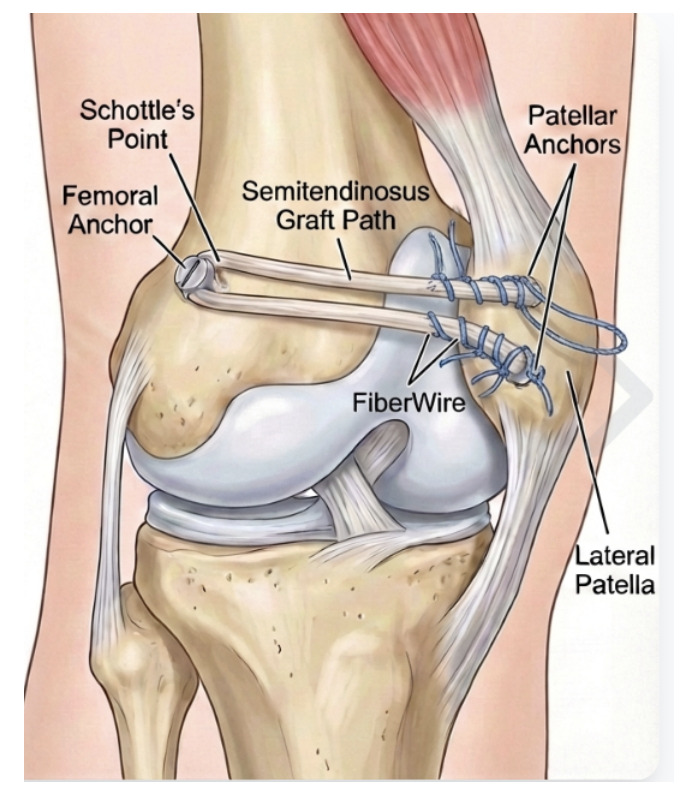
At this point, fluoroscopy was used to identify the lateral correlate of Schottle’s point, frequently used to identify the anatomic origin of the MPFL. A small longitudinal incision about 4 cm in length was made in this region over the lateral femur and after dissection through subcutaneous tissues, a pin was placed under fluoroscopic guidance as previously discussed in Beckert et al (Beckert et al. 2016). (Figure 3). The isometric point was then determined using a suture placed around the pin and up to the lateral patella, between layers 2 and 3 of the lateral knee. This pin was then over drilled and tapped. The 4.75 mm bio composite swivel lock was loaded onto the whipstitch in the middle of the allograft. This anchor was then placed into the prior drilled hole. (Figure 4).

_graft_preparation_2)_general_overview_of_surgic.png)
From the midline incision, a tonsil was used to dissect just superficial to layer 3 to grasp both ends of the graft and pull them up into the midline incision, deep to layer 2.
The lateral patella was then rongeured about its lateral edge to promote healing of the allograft. Two 2.6 mm hybrid knee fiber-tack anchors were then drilled and placed, with the first being at the most proximal aspect of the patella and the second being just distal to the midportion of the patella. The patella was then centered in the knee placed in about 30 degrees of flexion. Using the knotless mechanism, both limbs of the graft were then secured down to their respective anchors. Range of motion was checked to ensure it was full and that there was no mal-tracking of the patella. There was about 1-1/2 quadrants of medial translation with the knee in her natural hyperextension and about 2 quadrants of medial and lateral translation with the knee in 30 degrees of flexion. There was neutral patellar tilt. Each graft was then sutured to its respective anchor using the second set of sutures, again using a locking whipstitch (Figure 5). The knee was again ranged with similar findings.
A layered closure was then performed with the knee still in 30 degrees of flexion. #2 FiberWire was used to stitch the remnant LPFL over top of the graft back to remnant tissue on the patella. The most superficial layer of retinaculum was closed with a running 0 Vicryl suture. Range of motion and patellar translation were checked after this final closure, again found to be stable. Wounds were again irrigated and closed with deep 0 Vicryl, superficial 2-0 Vicryl and staples for the skin. A sterile dressing and knee immobilizer were then applied, and the tourniquet was let down.
Post-Operative Care
Postoperatively she was made touchdown weightbearing for 2 weeks. She was then started with physical therapy after the staples were removed with full range of motion and progressive weightbearing as quadriceps function allowed. She was fitted for a patellar stabilizing brace that would normally be utilized on the opposite knee for someone with lateral patellar instability.
Discussion
Medial patellar instability is a potentially disabling knee condition which occurs when lateral soft tissue constraints are injured or insufficient. Previous studies have demonstrated this condition can result in severe anterior knee pain, functional disability, and psychological problems, and that up to 85% of patients may not be able to perform light recreational activities (Hughston and Deese 1988; Sanchis-Alfonso and Merchant 2015). In comparison to the more well-defined lateral patellar instability, the predominant cause of medial patellar instability is iatrogenic following lateral retinacular release. Lateral release includes releasing part of the lateral stabilizing structures of the patella, which historically was commonly used for patellofemoral pain, lateral patellar compression syndrome, and improvement of patellar tracking (Tanaka 2022). One systematic review reported that up to 57% of patients develop medial patellar instability following lateral release (Song et al. 2016). Although the indications have certainly evolved with studies demonstrating its lack of clinical improvement and improved outcomes with retinacular lengthening versus lateral release, the latter is still performed and surgeons should be aware of the potential resultant complications (Song et al. 2016; Pagenstert et al. 2012). This case describes the rare occurrence of idiopathic medial patellar instability. Several surgical techniques have been described to address medial patellar instability, including LPFL reconstruction, lateral retinaculum imbrication, direct lateral retinacular repair, and lateral soft tissue augmentation with the iliotibial band, TFL, or patellar tendon (Hughston and Deese 1988; Hughston et al. 1996; Teitge and Torga Spak 2004; Huddleston et al. 2023; Chahla et al. 2019; Nonweiler and DeLee 1994). Although large high-powered studies are lacking, LPFL reconstruction is seen as a successful procedure for medial patellar subluxation, while direct repair or imbrication of the lateral retinaculum may be more likely to result in recurrence of instability (Hughston and Deese 1988; Shah et al. 2017; Saper and Shneider 2014; Hughston et al. 1996; Teitge and Torga Spak 2004; Kerzner et al. 2022).
The complex anatomy of the lateral knee is comprised of several ligamentous and tendinous structures that contribute to patellar stability (Kerzner et al. 2022). The contemporary understanding of the lateral knee anatomy is described as the lateral patellofemoral complex as described by Kerzner et al., which includes the iliotibial band extension to the patella (ITB-patella), the vastus lateralis tendon, the LPFL, the lateral patellomeniscal ligament (LPML), and the lateral patellotibial ligament (LPTL) (Kerzner et al. 2023). Multiple biomechanical studies have analyzed the role of the LPFL, solidifying the important of this structure in medial patellar stability (Kerzner et al. 2023; Shah et al. 2017; Saper and Shneider 2014; Sawyer et al. 2014; DeFroda et al. 2018; Vieira et al. 2007; Christian et al. 2020; Merican et al. 2009). Vieria et al. assessed the LPFL’s role in stability in a cadaveric study, and determined that resection of the LPFL increased medial patella subluxation (Vieira et al. 2007). Another anatomic study performed by Merican et al. sought to specify the role of the LPFL, and concluded that the LPFL was the main restraint to medial patellar translation between 0 and 20 degrees of flexion and at 90 degrees of flexion, and that the largest loss of stability occurs after LPFL and LPML release (Merican et al. 2009). While the LPFL’s role in medial stability is crucial, it has also been described as have an important role in preventing lateral patellar instability acting as a “bumper”, owing to its importance in overall patellofemoral stability (Christian et al. 2020).
Most surgical interventions are aimed at stabilizing the lateral structures of the knee. Various techniques have been described, including lateral repair and imbrication, and reconstructive options. The primary repair and imbrication option requires both sufficient tissue quantity and quality for an appropriate functional repair and has been found to be less reliable than ligament reconstruction options, with the concern of loss of imbrication strength over time (Hughston and Deese 1988; Kerzner et al. 2023; McCarthy and Bollier 2015; Hughston et al. 1996; Kerzner et al. 2022). Previous studies and case reports have demonstrated LPFL reconstruction improves pain and functionality in patients with medial patellar instability, both from iatrogenic and traumatic causes (Moatshe, Cram, et al. 2017; Hughston and Deese 1988; Hughston et al. 1996; Sanchis-Alfonso and Merchant 2015; Sanchis-Alfonso et al. 2015; Moatshe, Cinque, et al. 2017). There have been several reconstructive techniques described, including quadriceps tendon autograft with or without a bone block, gracilis allograft or autograft, patellar tendon graft, and semitendinosus allograft (Saper and Shneider 2014; Beckert et al. 2016; Teitge and Torga Spak 2004). In addition to a variety of graft options, there has also been mixed fixation strategies. With regards to the femoral insertion site, options include suture anchors, bone block graft fixation using lag screws, and interference screw fixation of the graft within transosseous tunnels (Saper and Shneider 2014; Tanaka 2022; Sanchis-Alfonso et al. 2015; Arora et al. 2024). The patella fixation techniques described include trans osseous tunnels, suture anchors, interference screws and isolated suture fixation to the anterior patella (Beckert et al. 2016; Kerzner et al. 2022). Given the overall low incidence of these reports, there is no high level evidence supporting one defined technique over another.
The procedure described in this case utilized one suture anchor for femoral graft fixation and two suture anchors for patella fixation. Similar to Beckert et al., a semitendinosus allograft was used with the lateral mimic of Schottle’s point identified for femoral graft fixation, and two points of fixation used on the patella. However, in our case, for the femur, we used a suture anchor while their case series used an endobutton secured to the medial femoral condyle. We also used two suture anchors for fixation to the patella while they used FibreWire fixation alone. At an average of 2.05 year follow-up, Beckert et al. report that out of 19 knees of 17 patients, none of their patients demonstrated medial patellar apprehension or objective exam findings of subluxation, with significant increases in outcome scores (Beckert et al. 2016). One of the proposed benefits of their patellar suture-fixation is the decreased risk of patellar fracture. Although most studies evaluating this have been with MPFL reconstruction, a greater association with fractures has been described with transosseous patellar tunnels as opposed to suture anchors (Figueras et al. 2022; Schiphouwer et al. 2017). Recent studies have also suggested suture anchor use is associated with improvement in patient-reported outcomes (Figueras et al. 2022; Heo et al. 2019). Our use of two suture anchors in the patella mirrors the two point fixation technique described by Figueras et al for MPFL reconstruction, with the goal of increasing contact area between the graft and patella, and thus fixation strength (Figueras et al. 2022). As described in anterior cruciate ligament reconstruction literature, it is well known the contact surface area between graft and bone is critical for the ligamentization process and formation of this tissue that allows for integration of the graft (Figueras et al. 2022; Nebelung et al. 2003). This phenomenon involves the integration of tendon grafts through tissue composed of fibers anchored to the mineralized bone in a Sharpey fiber–like pattern (Figueras et al. 2022; Nebelung et al. 2003). Therefore, it is reasonable to believe that increasing the contact surface area during LPFL reconstruction using two suture anchors can lead to an optimal environment for graft integration and increased patellar stability.
Conclusion
Idiopathic medial patellar instability is a rare knee pathology, and LPFL reconstruction using semitendinosus allograft with all suture anchor fixation is a viable surgical option.