INTRODUCTION
Total shoulder arthroplasty (TSA) has emerged as the fastest-growing major joint replacement procedure in the United States, with a 104% increase in primary shoulder arthroplasties from 2011 to 2017 (Wagner et al. 2020). In contrast, total hip arthroplasty (THA) and total knee arthroplasty (TKA) volumes increased by 29% and 18%, respectively, in the same period (Wagner et al. 2020). Recent advances in implant technology have also further accelerated TSA adoption (Best et al. 2021). The exponential rise in TSA is particularly linked to the broader use of RSA for a wider range of pathologies, including rotator cuff arthropathy, complex fractures, and failed prior repairs (Fornaciari et al. 2025). Optimizing perioperative management in this patient population remains critically important.
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) were initially developed for glycemic control in Type 2 DM but have rapidly expanded in use due to their efficacy in weight reduction and broader metabolic benefits (Drucker 2025). The literature demonstrates a marked increase in use among both diabetic and non-diabetic populations undergoing total joint arthroplasty, particularly total hip and knee arthroplasty. In a systematic review of 16,467 lower extremity arthroplasty patients on GLP-1 RAs, four of the seven included studies specifically analyzed both diabetic and non-diabetic users, reflecting the expanding adoption of these agents for weight management and glycemic control (Lee et al. 2025).
The role of GLP-1 RAs in mitigating disparities after total joint arthroplasty (TJA) remains under investigation, with most emerging results found in studies on hip and knee arthroplasty. One systematic review and one meta-analysis on hip and knee arthroplasty, both published in 2025, agree that GLP-1 RA use is associated with reduced rates of periprosthetic joint infection (PJI), but differed with their conclusions as to whether other postoperative complications were primarily improved or worsened among patients receiving GLP-1 RAs (Lee et al. 2025; Chan et al. 2025). Studies comparing patients undergoing TJA who were taking GLP-1 RAs to non-users have found no differences in surgical or medical complication rates, while others have raised concerns about potential risks such as malnutrition or perioperative aspiration, especially in non-diabetic populations using GLP-1 RAs for weight loss alone (Ramanathan et al. 2025).
Despite the increasing prevalence of GLP-1 RA use and the rising volume of TSA procedures, there is a limited amount of literature specifically addressing the effects of GLP-1 RAs on postoperative outcomes in the TSA population (Jacofsky et al. 2024). The distinct pathophysiology, surgical techniques, and complications associated with TSA underscore the need for targeted research to determine how the effects of GLP-1 RAs on outcomes in TSA may differ from THA and TKA (Fornaciari et al. 2025).
No systematic review has specifically examined the effects of GLP-1 RAs on postoperative outcomes following TSA. Given the growing use and potential impact on surgical outcomes, a comprehensive synthesis of the existing literature is warranted. This review aims to consolidate current studies on how GLP-1 RA use in patients undergoing TSA affects postoperative complications. A clear understanding of these relationships may enhance perioperative decision-making, guide clinical management strategies, and highlight key areas for future research.
METHODS
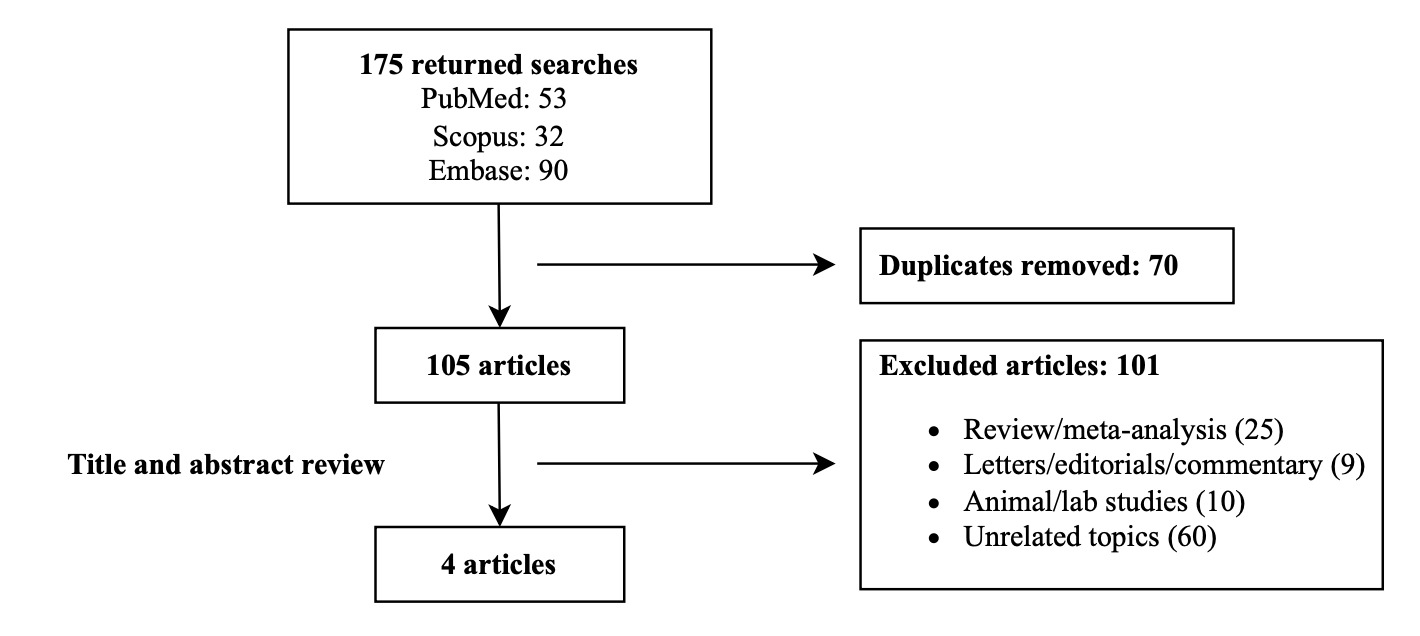
This systematic review adhered to the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework (Page et al. 2021). Relevant literature was searched for using PubMed, Scopus, and Embase from database inception through July 26, 2025. The following search strategy was used: ((GLP-1 OR Semaglutide) AND (TSA OR joint replacement OR arthroplasty)). The review was registered with the International Prospective Register of Systematic Reviews (PROSPERO; registration ID: CRD420251112989). A total of 175 studies were initially identified and underwent a four-step screening process: identification, screening, eligibility, and inclusion.
All retrieved citations were imported into Rayyan (Rayyan Systems Inc., Cambridge, Massachusetts, USA) for organization and screening. After removing 70 duplicates, 105 articles remained. Two reviewers (JA and VL) independently reviewed titles and abstracts, excluding 101 studies based on predefined eligibility criteria. This resulted in four full-text articles that met inclusion requirements (Figure 1). Any disagreement between the two reviewers was settled by a third author (RD).
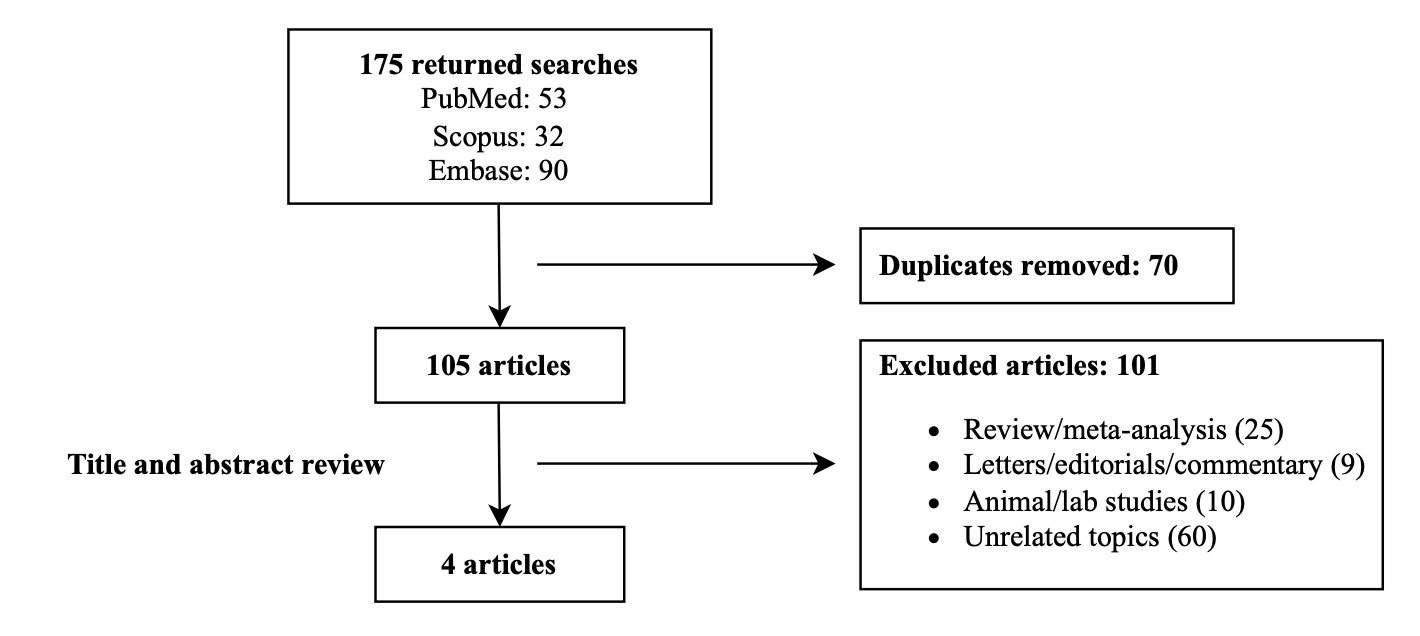
Included studies evaluated postoperative outcomes in patients undergoing TSA while receiving GLP-1 RA therapy, regardless of indication. Excluded studies were reviews, meta-analyses, letters, editorials, expert commentaries, and any animal or laboratory-based research. We also excluded studies that focused on non-TSA orthopedic procedures or did not focus on data pertaining to the postoperative period. Data extracted from eligible studies included: first author and year of publication, journal source, database utilized, size of the GLP-1 RA cohort, characteristics of the case and control groups, matching strategy, follow-up duration points, and main findings.
RESULTS
Study Characteristics
This systematic review incorporated four studies comprising a total of 7,406 patients who underwent TSA and were prescribed GLP-1 RAs. All four studies were published in 2024, and all four were from The Journal of Shoulder and Elbow Surgery (JSES) and its subsidiary journals. All studies utilized large-scale national databases, with two drawing data from PearlDiver and the other two from TriNetX.
Each study employed a case-control design comparing outcomes between GLP-1 RA users and matched non-user controls. Three of the studies included only patients with a diagnosis of DM in the GLP-1 cohort, whereas the fourth included both diabetic patients and obese individuals without DM. Of the four, three explicitly focused on individuals with Type 2 DM, while one included non-diabetic patients as well in the case group. None of the studies differentiated Type 1 DM as a subgroup.
All studies evaluated complications occurring within 90 days following as a common short-term metric. Additionally, two of the four studies reported longer-term postoperative outcomes up to two years. A detailed summary of each study’s design, patient population, and main findings is provided in Table 1.
Synthesis of Results
Choudhury et al. evaluated GLP-1 RA use in patients with Type 2 DM undergoing TSA (Choudhury et al. 2025). There were no differences between the postoperative outcomes studied, except for reduction in the 90-day mortality rate (Choudhury et al. 2025). Other 90-day postoperative complications evaluated included cerebrovascular accident, readmissions, acute kidney injury (AKI), pulmonary embolism (PE), deep venous thrombosis (DVT), surgical site infection (SSI), coma, emergency department (ED) visits, myocardial infarction (MI), sepsis, respiratory complications, urinary tract infection (UTI), wound dehiscence, and stroke (Choudhury et al. 2025). Longer-term complications assessed at two years included aseptic loosening, revision surgery, PJI, and periprosthetic fracture (PPF) and were found to be similar between users and non-users of GLP-1 RAs (Choudhury et al. 2025). Overall, the study found that GLP-1 RA users had lower 90-day mortality (OR 0.17) (Choudhury et al. 2025).
Elsabbagh et al. investigated the impact of GLP-1 RA use in patients with Type 2 DM undergoing TSA (Elsabbagh et al. 2025). The 90-day postoperative complications studied were DVT, cardiac arrest, MI, CVA, pneumonia (PNA), PE, UTI, SSI, readmission, hypoglycemic events, and sepsis (Elsabbagh et al. 2025). The 2-year postoperative complications studied were PJI, PPF, all-cause revision, and aseptic revision (Elsabbagh et al. 2025). The study reported no statistically significant increase in the risk of postoperative complications, including all 90-day and 2-year postoperative outcomes, when compared to patients with Type 2 DM not using GLP-1 RAs (Elsabbagh et al. 2025). Additionally, no difference in the length of hospital stay (LOS) was observed (Elsabbagh et al. 2025).
In contrast, Lawand et al. examined TSA outcomes in patients using GLP-1 RAs for either DM or obesity (Lawand et al. 2025). The 90-day postoperative complications assessed were blood transfusion, DVT, stroke, MI, PNA, kidney failure, postoperative anemia, PE, and hospital readmission, and the 2-year postoperative complications assessed were mechanical loosening, PPF, revision, and PJI (Lawand et al. 2025). Compared to non-users, GLP-1 RA users had higher 90-day rates of DVT (1.6 vs. 0.9%; OR 3.0), MI (1.6 vs. 0.9%; OR 2.84), PNA (3.34 vs. 1.5%; OR 2.25), transfusion (7.1 vs. 4.3%; OR 1.7), and hospital readmission (8.1 vs. 5.2%; OR 1.6) (Lawand et al. 2025). However, there were no differences between the groups in the rates of stroke, PE, postoperative anemia, or kidney failure (Lawand et al. 2025). Additionally, the 2-year revision rates did not differ between the groups (3.2 vs. 1.8%; OR 1.8) (Lawand et al. 2025). The data regarding 2-year rates for PPF, PJI, or mechanical loosening were either unavailable or insufficient (Lawand et al. 2025).
Seddio et al. assessed only 90-day outcomes in patients with Type 2 DM using semaglutide following TSA (Seddio et al. 2024). The outcomes of interest were categorized into the following groups: severe adverse events (SAEs), minor adverse events (MAEs), and health-care utilization (Seddio et al. 2024). SAEs consisted of SSI, cardiac events, venous thromboembolism (VTE), prosthetic shoulder dislocation, and sepsis (Seddio et al. 2024). MAEs consisted of PNA, UTI, wound complications, and AKI (Seddio et al. 2024). Healthcare utilization consisted of ED visits and readmissions (Seddio et al. 2024). Patients on semaglutide had lower odds of developing AAEs (OR 0.27), SAEs (OR 0.40), or MAEs (OR 0.27) (Seddio et al. 2024). Specifically, they had decreased rates of SSI, cardiac events, VTE, PNA, UTI, AKI, and ED visits (Seddio et al. 2024). However, there were no differences between the groups regarding sepsis, prosthetic shoulder dislocation, wound complications, or hospital readmission (Seddio et al. 2024).
DISCUSSION
Our study identified four retrospective database studies: two reported primarily improved postoperative outcomes, one demonstrated a worsened complication profile, and one found no difference. GLP-1 RAs are prescribed with increasing frequency with shoulder surgeons encountering a growing proportion of TSA candidates receiving these agents. The perioperative implications of GLP-1 RA therapy, however, remain unclear. Retrospective case reviews of THA and TKA patients with preoperative GLP-1 RA use showed a decreased 90-day risk of PJI as well as readmission, while others have raised concerns that continued therapy may be associated with higher odds of MI, AKI, and PNA (Buddhiraju et al. 2024; Magruder et al. 2023). The conflicting results indicate that conclusions from these studies cannot be extrapolated to TSA, warranting further investigation into GLP-1 RA usage in TSA patients, particularly considering the differences between different arthroplasties. Importantly, interpretation of the TSA-specific data is constrained by the small number of available studies, all of which are retrospective and database-driven. Given these conflicting findings, a practical interpretation is to view GLP-1 RA use as a risk marker that likely depends on patient context rather than a uniform effect. Clinically, surgeons may consider the indication for therapy (diabetes management vs. weight loss) and overall cardiometabolic risk when counseling TSA patients and coordinating perioperative care.
The use of GLP-1 RAs has rapidly expanded beyond the traditional indication for diabetes management. These medications are increasingly prescribed off-label for weight loss in patients with obesity or metabolic syndrome, due in part to demonstrated cardiovascular and metabolic benefits (Rohani et al. 2023; Wilding et al. 2021). GLP-1 RA prescriptions have seen a dramatic increase in utilization, with the Intelligence, Quality, Value, Information, and Analytics (IQVIA) InstituteTM reporting a 181% increase in new prescriptions across the United States from 2022 to 2024 (IQVIA Institute for Human Data Science 2024). This data calls into question the accessibility and cost of these medications as they remain expensive and often lack insurance coverage for non-diabetic indications. According to the Kaiser Family Foundation Health Tracking Poll conducted in 2024, approximately 54% of all adults that have taken a GLP-1 RA report it being difficult to afford (Montero et al. 2024). As the use of GLP-1 RAs continues to expand to other demographics, the cost will become increasingly important in orthopaedic surgery as many patients have comorbidities that these medications can be used to treat.
Cost barriers that disproportionately affect minorities may compound existing inequities in surgical outcomes, emphasizing the need for equitable drug affordability as part of a strategy to reduce disparities in orthopaedic care. African American patients in particular experience worse outcomes following TSA, with lower utilization rates, longer hospital stays, higher costs, and increased non-home discharges as well as 30-day readmission rates when compared to White patients (Ragland et al. 2025). Emerging data also indicates that racial and ethnic minority groups, specifically African American, Hispanic, and Asian individuals, have lower rates of GLP-1 RA utilization, despite being commercially insured (Bepo et al. 2024; Eberly et al. 2021). A JAMA Health Forum analysis of over 1.1 million commercially insured adults with Type 2 DM revealed that Asian, African American, and Hispanic patients all had lower odds of receiving GLP-1 RA prescriptions than their White counterparts despite similar comorbid conditions (Eberly et al. 2021). Even with comparable access to GLP-1 RAs, median out-of-pocket costs were approximately $40 per 30 days, and annual Medicare costs for specific agents exceeded $2,400, disproportionately affecting marginalized groups (Luo et al. 2020; Young et al. 2024). Given that TSA patients exhibit higher rates of comorbidities such as obesity and DM, equitable access to GLP-1 RAs may be impactful to mitigate adverse outcomes following the procedure, regardless of race.
Analysis of the demographic trends in patients undergoing orthopaedic procedures, particularly TSA, reveals an increase in age at utilization as well as in obesity and diabetes mellitus (Bixby et al. 2020; Dean et al. 2023). The use of GLP-1 RAs postoperatively could provide a promising avenue for minimizing the risk of complications following TSA. Patients undergoing TSA are generally older than those undergoing THA or TKA, with an average age of 69.3 years compared to 65.3 years and 66.9 years, respectively (Dean et al. 2023). Prevalence of DM also increases with age, with multiple databases reporting increased prevalence in diagnosed DM as well as prediabetes amongst aging Americans (Centers for Disease Control and Prevention 2024; Gwira et al. 2024). Obesity, diabetes, and metabolic syndrome are all associated with a pro-inflammatory state and abnormal bone mechanics, which may predispose patients to complications following surgery (Dandona et al. 2005; Rinonapoli et al. 2021). Understanding how GLP-1 RA therapy influences healing and implant integration could help improve long-term outcomes for higher-risk patients. Altered healing and collagen remodeling can cause soft tissue laxity, component loosening, and periprosthetic fracture following shoulder arthroplasty; thus, restarting GLP-1 RA postoperatively could potentially mitigate the risk of adverse outcomes through improvements in patients’ metabolic profile (Rohani et al. 2023; Kusin et al. 2019). With the demographic of patients undergoing TJA continuing to change, it is becoming increasingly important to understand how the use of GLP-1 RAs affects implant outcomes in these high risk cohorts.
Preclinical studies show that GLP-1 signaling stimulates osteoblast differentiation while suppressing osteoclastogenesis, yielding an overall anabolic effect on bone (Mabilleau and Bouvard 2024). Clinical meta-analyses mirror these findings, linking GLP-1 RA therapy to higher bone mineral density and fewer fragility fractures (Zhang et al. 2025). Because glenoid component loosening remains the leading cause of revision after TSA, strategies that improve periprosthetic bone quality are especially valuable (Lauck et al. 2025; Bohsali et al. 2017; Wolff and Rosenzweig 2017). Future trials could therefore stratify patients by glenoid morphology and collect bone-turnover markers to determine whether the skeletal benefits of GLP-1 therapy translate into lower rates of aseptic loosening or periprosthetic fracture.
GLP-1 RAs have been shown to improve systemic inflammation and glycemic variability, both of which are favorable for musculoskeletal healing in the perioperative setting (Ihnat et al. 2025). However, GLP-1 RAs induce weight loss that includes reductions in both fat and lean mass. Meta-analyses have shown that approximately 30% of GLP-1 RA-induced weight loss is lean mass, raising concerns about GLP-1-induced sarcopenia, particularly in procedures heavily reliant on muscle integrity, such as RSA (Linge et al. 2024). While the overall perioperative profile of GLP-1 RAs remains favorable, further investigation is warranted to determine how their effects on lean body mass may influence postoperative strength and functional recovery.
Consensus on cessation protocols for GLP-1 RAs prior to elective procedures remains divided. Despite potential benefits, concerns persist regarding delayed gastric emptying and an increased aspiration risk, along with gastrointestinal side effects such as nausea and bloating (Joshi et al. 2023; Klein and Hobai 2023). Current guidelines from the American Society of Anesthesiologists recommend withholding daily-dose GLP-1 therapy on the day of elective surgery and weekly formulations for seven days preoperatively, regardless of indication (Joshi et al. 2023). However, these guidelines have been called into question by recent meta-analyses and retrospective reviews. Elkin et al. conducted a retrospective review and meta-analysis on GLP-1 RA usage, concluding that while patients taking GLP-1 RAs are more likely to present to surgery with residual gastric contents, they are not at an increased risk of pulmonary aspiration (Elkin et al. 2025). In contrast, Holland et al. found that stopping Ozempic therapy at least 7 days prior to joint arthroplasty decreased the risk of delayed emergence from anesthesia and aspiration, and stopping at least 14 days prior to joint arthroplasty reduced the risk of aspiration as well as intubation post-procedure (Chokshi et al. 2025). At present, there is no gold standard for when to stop GLP-1 usage, likely due to diverse indications for the medication as well as differences in fasting guidelines and risk assessment among practitioners (Joshi et al. 2023; Elkin et al. 2025; Chokshi et al. 2025).
This study has potential limitations. All four retrospective studies relied on national databases, specifically TriNetX and Pearldiver. TriNetX is a clinical database that gathers de-identified patient information via electronic health records through healthcare organizations (Ludwig et al. 2025). Given the number of healthcare organizations involved with TriNetX, 128 globally, with 66 of them being in the United States, there are discrepancies in how data is collected across these different healthcare organizations (Ludwig et al. 2025). In contrast, PearlDiver is a claims database compiled from sources such as Medicare and Medicaid, along with commercial insurance companies such as Humana (Bolognesi and Habermann 2022). As a claims database compiled from billing data, it was not originally designed for clinical research, limiting its applicability for such clinical studies. Overall, these national databases have large patient numbers, but data are subject to low standardization and less nuanced patient factors. Data aggregated from many independent healthcare systems vary in coding practices and clinical documentation, which can introduce residual variability and bias. This highlights the need for future prospective studies with standardized data collection and outcome definitions, as well as greater data stratification to more accurately assess the impact of GLP-1 RA use on a growing demographic of TSA patients.
CONCLUSION
The available evidence on GLP-1 RA use in TSA remains limited and mixed. As usage of these medications continues to increase, a better understanding of implications with GLP-1 RA therapy on patients undergoing TSA is of clinical importance to orthopaedic surgeons. Future research should focus on clarifying perioperative protocols and stratifying outcomes by patient characteristics, medication use patterns, and surgical techniques to guide clinical decision-making.
ACKNOWLEDGEMENT
We would like to thank the Mercer University School of Medicine, the Tulane University School of Medicine, the Edward Via College of Osteopathic Medicine, and the Hughston Foundation for providing the resources to complete this systematic review.