I’m an orthopedic surgeon in Houston, and will review ASCs and spine surgery, some of the pros and cons and challenges of that.
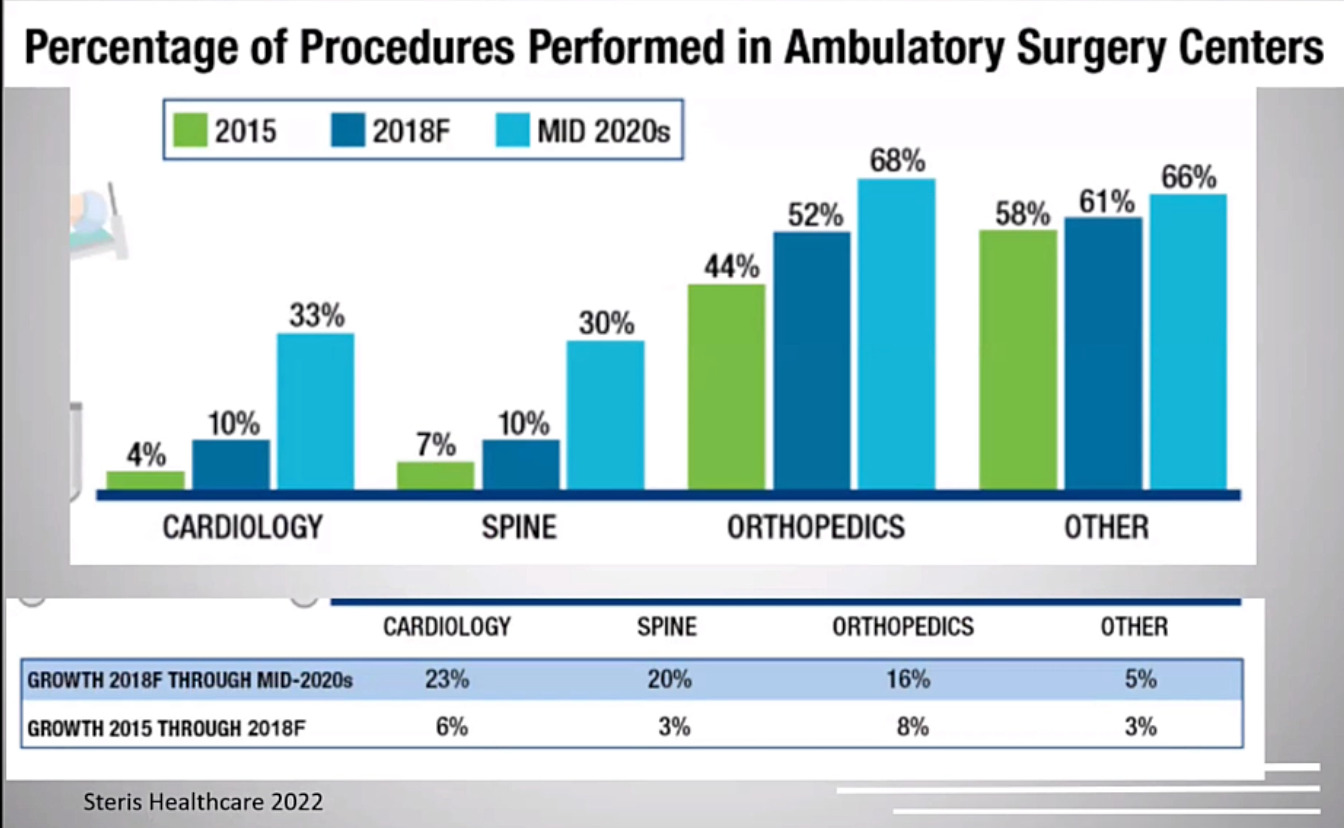
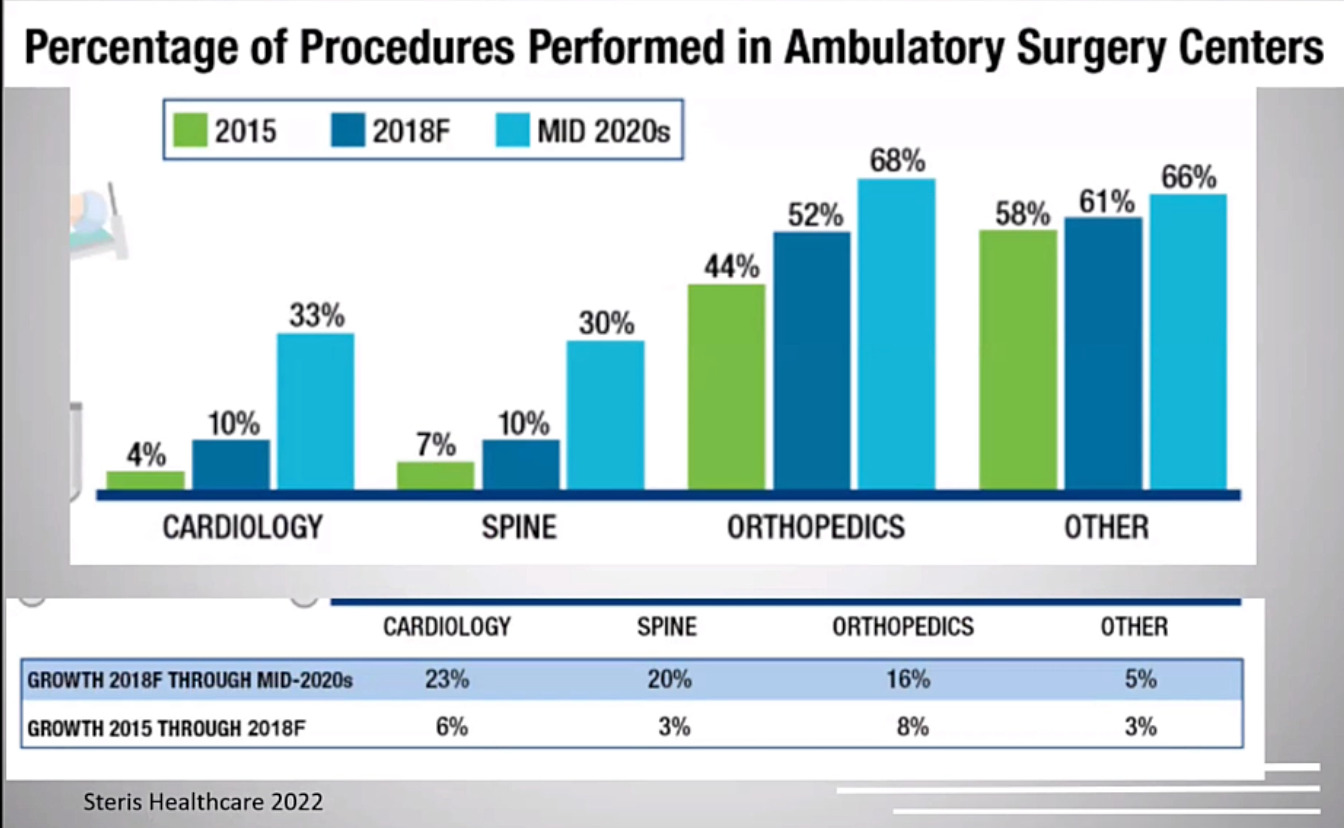
I was also the chief medical officer and part of the board of directors for a regional surgery center company for about five years, and we were publicly traded. My practice itself is a private practice. It’s very community based. We do a lot of outpatient care. I have a lot of sports partners, so this type of practice works well in a surgery center setting. We’re very dependent on the ancillary revenue from the surgery center to make our private practice feasible. Just as some background, as you probably all know, surgery centers and the surgery center industry have grown a lot in the last 10 to 20 years. We have better technology that allows us to operate more in the surgery center. It’s better for patients and physicians and it allows us to control some healthcare costs. This data just shows that we’re doing more cases in the surgery center over the years and that’s the case for all specialties, particularly spine going from about 7% to 30% in the last couple decades of cases done in the surgery center. (Figure 1)
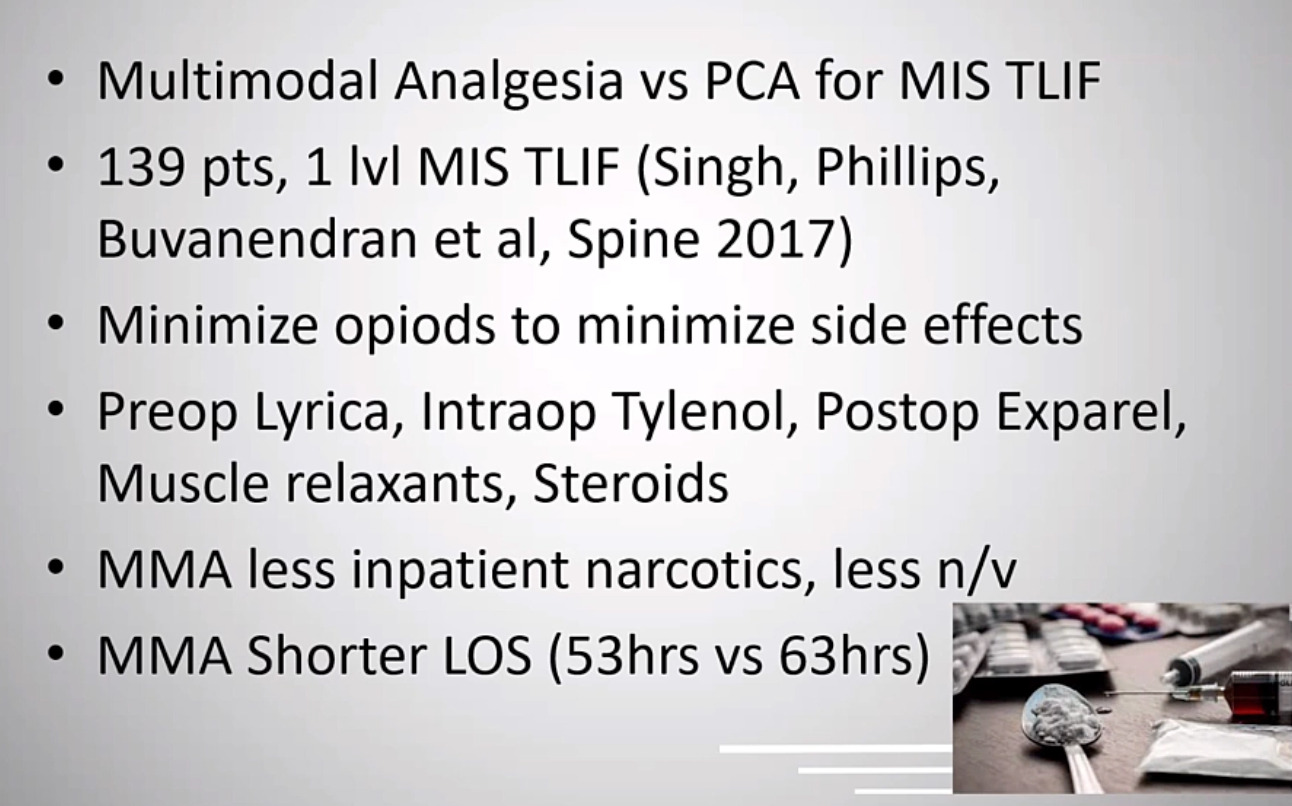
As a framework, we’re going to talk about the clinical and the financial aspects of ASC spine surgery. We’re going to talk about the benefits and the challenges from a clinical perspective, and the benefits and challenges from a financial perspective. That’s kind of how this will flow. So starting with kind of the clinical benefits of ASC spine surgery, the good stuff. So healthcare is becoming increasingly a consumer driven industry. We have an active, older population that has a lot of access to information through the internet and marketing and the financial burden of healthcare is being shifted to patients through higher deductibles and more copay. So our patients have higher expectations and want greater care. And the surgery center is really a consumer-oriented center of care, generally because of higher volumes and being specialized. We can do these cases in an efficient way with a more predictable schedule, and that results in better satisfaction for our patients. When we look at the data of the cases that we do in a surgery center, such as lumbar decompressions, laminectomy and discectomies, and cervical disc replacements and cervical fusions we can do those in a surgery center with equivalent outcomes to the hospital and some data even shows better rates in terms of complication and outcome.That’s often because we have patients in the surgery center that may be lower risk with less medical problems. But what we do know is we can do these cases just as well in a surgery center without compromising patient care. As a physician, when you work in a surgery center, you generally have control over the center. You’re treated more like a customer with a shorter turnover, better equipment and just generally a better work environment because we’re often invested in the center and we have a lot of efficiencies and surgeons like that environment. So what about the challenges of being in a surgery center as you migrate patients from inpatient to the outpatient? There are a lot of challenges to be aware of. Let’s start with what cases are best for the surgery center? So are not instrumented spine cases like laminectomies and micro discectomies are a good place to start. If we’re going to do cervical surgeries like an ACDF or cervical disc replacement one and two level surgeries for those are done well in a surgery center. Those are probably the best cases to start within a surgery center as you become more comfortable you can do possibly lumbar fusions particularly minimally invasive fusions like T-lifts or laterals.Those could all be done in a surgery center in the right situation. Obviously they are being done by a lot of people. As you transition to a surgery center, you want to keep a lot of things in mind. You have to select the right patients, be aware of comorbidities, like cardiac issues or sleep apnea that may prevent that patient from being a good candidate for the surgery center. We need to educate our patients from the beginning, discuss pain management, we want to make sure that they have help when they get back home after the case. My whole team needs to be involved, including people in my office and the anesthesia staff. Everyone needs to be sort of on board with the right environment so patients understand these cases can be done well in a surgery center. It’s good to have a backup plan if we need to admit a patient and we want to start slow. There’s always a learning curve when we do these things. That slide’s not too helpful. So, moving on, if we think about the reasons why patients do stay in the hospital overnight after spine surgery, it’s usually medical reasons like diabetes, heart disease and then other having a durotomy or severe pain afterward. So we kind of have to have a plan for each of these issues. If we’re going to do a case in the surgery center and a patient has sleep apnea or we get a durotomy, what is our plan in the surgery center?It’s best to kind of define these pathways when we’re doing these cases in a hospital and then as we transition to the surgery center kind of having all of those possible outcomes planned for. Pain management is a big issue. This is a study from Rush that shows using multimodal analgesia helped a lot with transitioning patients to the surgery center for minimally invasive lumbar fusions. (Figure 2)
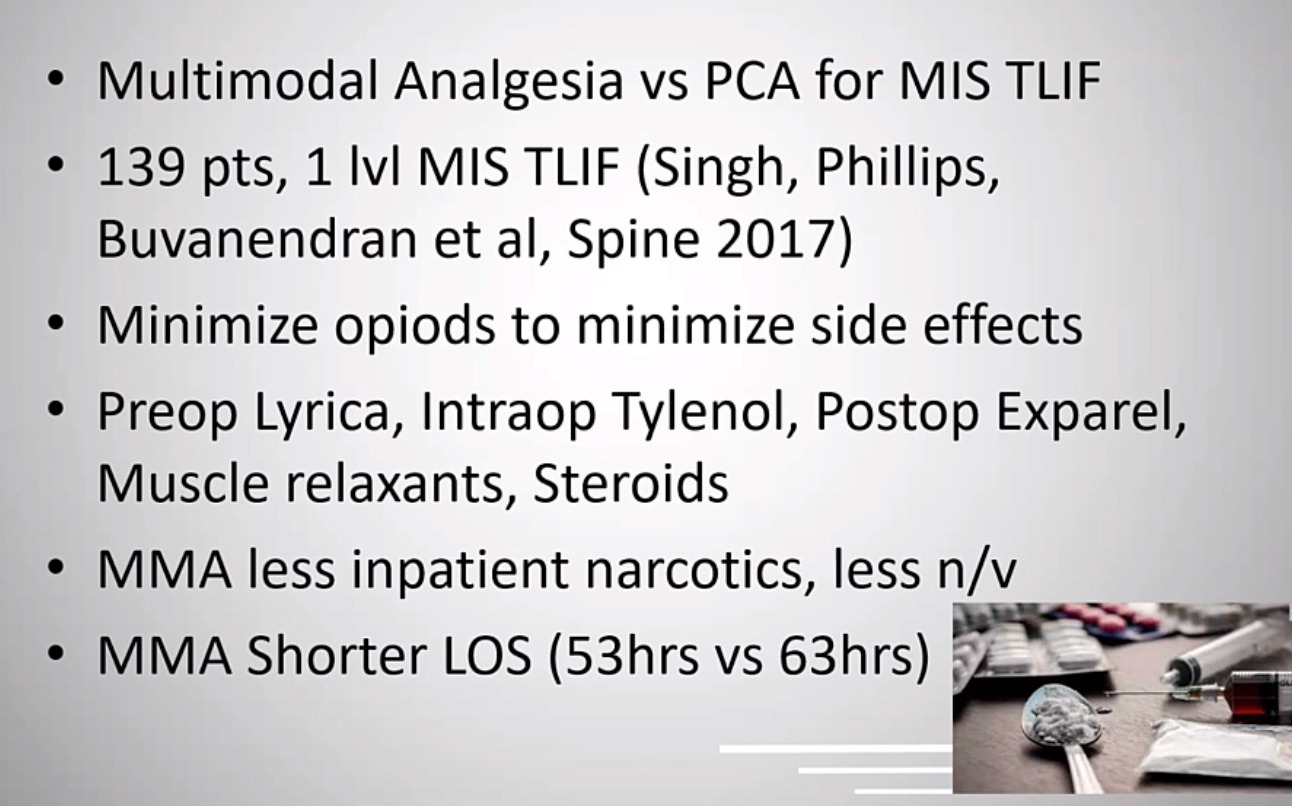
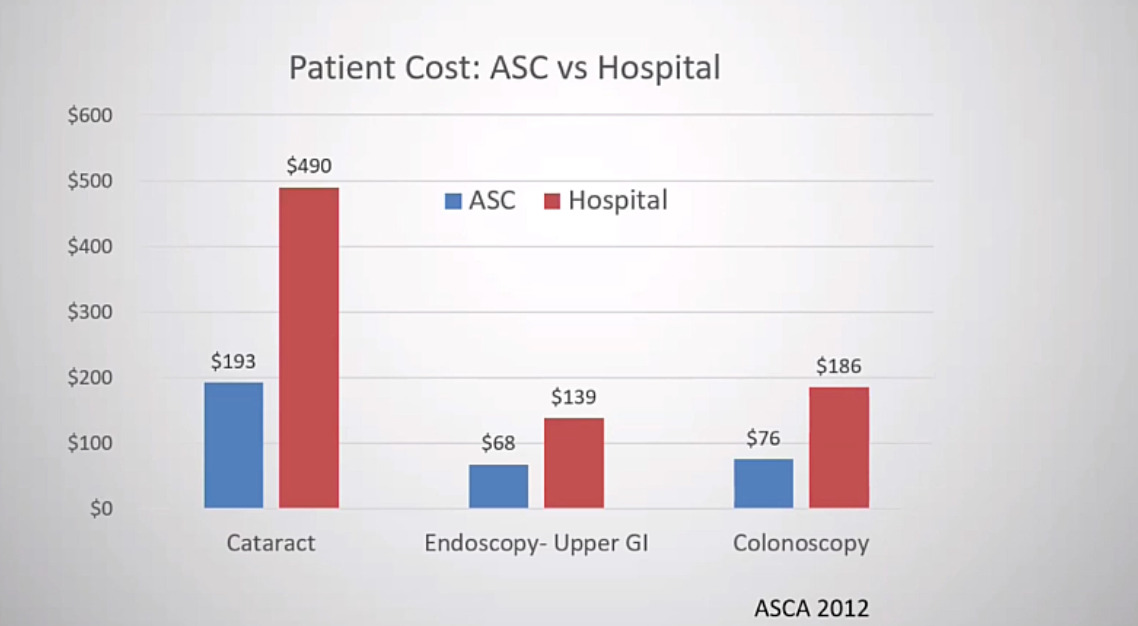
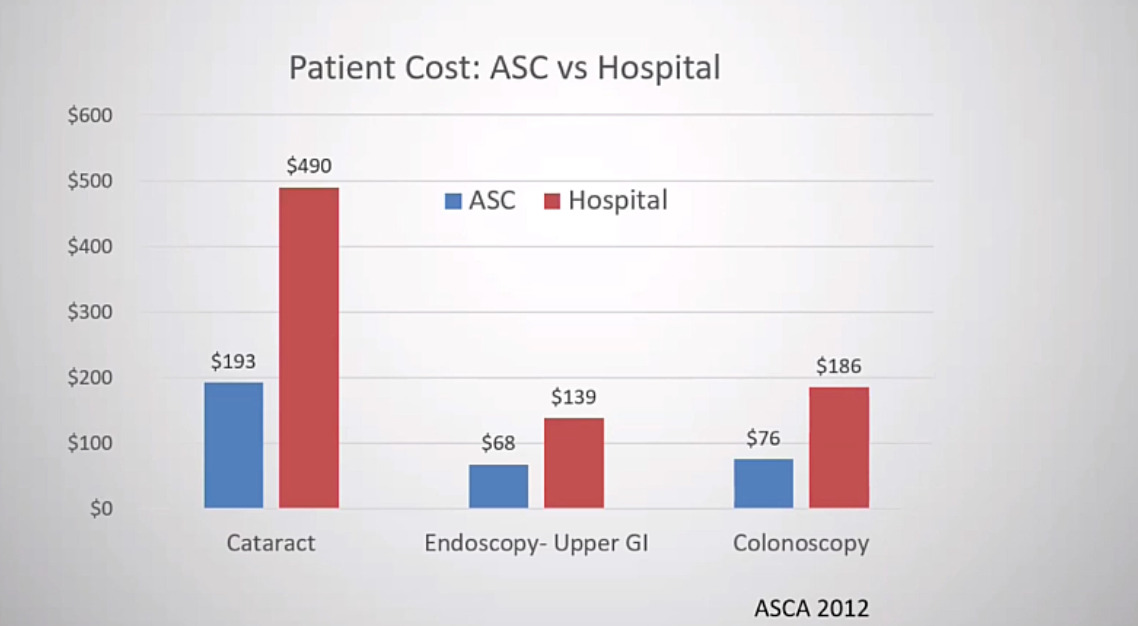
The key is minimizing opioids that decrease side effects and usually allows patients to mobilize more quickly. So using Lyrica, Tylenol, Exparel, all of these techniques together help decrease the need for narcotics and allow us to get patients out of the surgery center more quickly. So let’s shift gears now and talk about the economic side of things. So we’ll first, start with the positives of the surgery center from an economic perspective. The surgery center is, is lower cost. That’s really what it comes down to, so when patients are paying something out of pocket for their healthcare, if we do this in a surgery center, they generally pay less out of pocket and that’s the case for most of the data that we see. And that’s for eye surgery, for endoscopy and for spine surgery as well. (Figure 3)
Physicians can be involved in the ownership of the surgery center. That’s really the best economic benefit for us. Most surgery centers have physician ownership.
A lot of them are solely owned by physicians. They’re often joint ventures with management companies or hospitals. If this is something that you’re interested in you have to have an understanding of the management situation and the ownership model of the surgery center and have a good idea of what the buy-in is and what the return would be. But these can be profitable for physicians. There’s different types of ownership models. They can be physician owned, they can be a joint venture with management companies or hospitals. They’re all different types of arrangements with each one there’s usually a buy-in that the physician participates in and then an expected return, and that may be one year, two years, five years. It really depends on the situation. If it’s an established surgery center, the buy-in may be very high because it’s a multiple of earnings, and therefore would take a longer time to make that back. But you have the safety and security of a center that’s been around for a long time. If it’s a new surgery center, the buy-in may be lower, but there’s a potential that may not be financially successful in the long run.
There’s a one third rule, which means when we’re a part of the surgery center, we must do a third of our cases there and also be aware of non-competes. Once you buy into one surgery center, it may be difficult to buy into others because of non-competes. That’s really the way it should be. The surgery center works best when all the partners are invested in doing as many of their cases as they can there. As I said before, the big financial benefit of the surgery center is that it is a lower cost center than a hospital. It’s generally 55 to 58% the cost of doing the same case in a hospital. This leads to savings for healthcare dollars. We can save a lot of Medicare dollars by shifting more of our cases from hospitals to the surgery centers when appropriate. If we’re interested in saving money for the US healthcare system in general, this is probably the number one thing that surgeons can do in order to save money by shifting the site of surgery when possible. As I said before a lower cost center, 55 to 58% compared to the hospital, and the data shows that for things like laminectomy and ACDF, which we do in the surgery center.
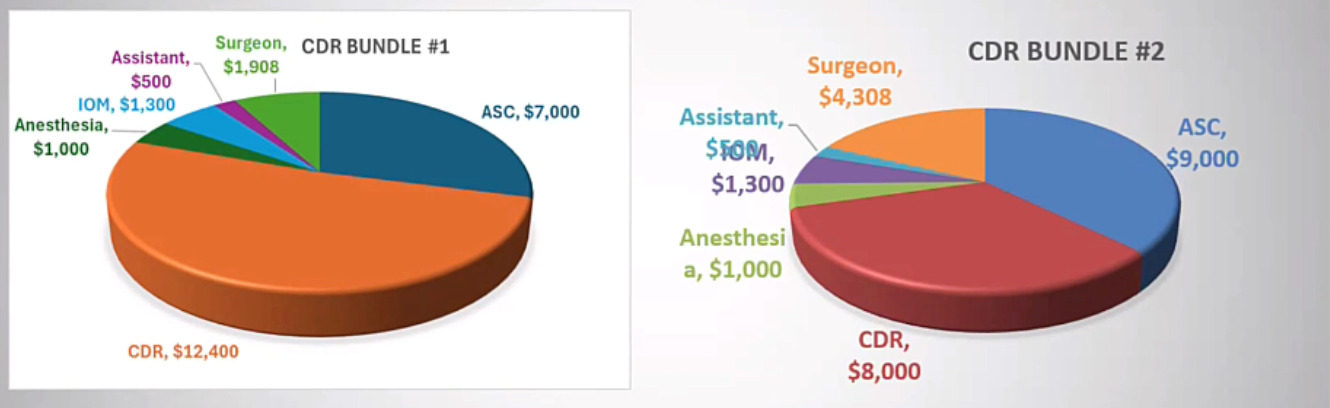
Another way that we can be aware of cost and control our cost is by looking at what we spend on implants. So I do some cases where I work directly with employers and they will give me a bundled payment to take care of the entire episode of care. So this is an example where I was given a bundle of approximately $24,000 for a two level cervical disc replacement. (Figure 4)
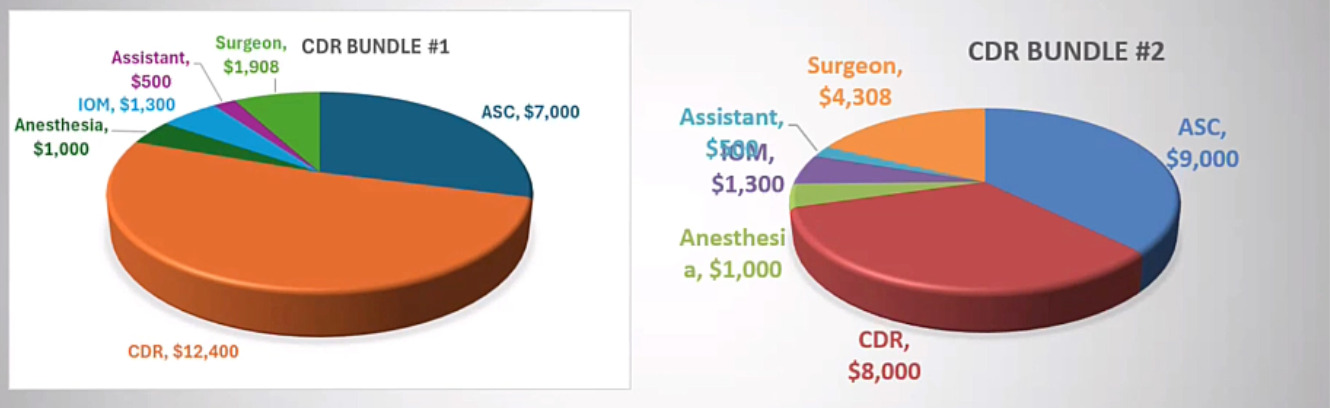
My initial implant cost for cervical disc replacement was around $6,000. So for two of those, that’s $12,000. So that’s really half of the bundle. In that scenario, it’s hard to make this profitable for the surgeon or the surgery center. But I was able to get our implant costs down with some national pricing through a group called Luminary and then at $4,000 in implant we’re able to make the case profitable for the surgery center and reasonable for the surgeon as well. So it is just important that we’re aware of all of the costs in order to continue to do these cases in a surgery center where we need to keep the costs lower to be profitable. There’s a shift in healthcare towards lower cost solutions. We often think about sustaining innovations, which are expensive things that often only improve care slightly. Things like navigation and robotic surgery total disc replacement itself. So all of these things are great for patients, but they cost a lot and they may not always make the clinical outcomes significantly better.
If we think more about disruptive innovations, these generally allow us to do things with a lower cost and the surgery center is really a great example of that. If we take cases from hospitals and we shift them to surgery centers it really leads to sort of a decentralization of healthcare and in many industries with better technology and better focus on cost control this leads to disruptive innovations, which leads to decentralization. That’s good for a lot of industries. If you just think about the computer industry as technology has gotten better, we’ve gone from large central mainframe computers to personal computers, to laptops, and now to phones. So just with better technology, everything is decentralized and more people can do the same thing on their own. So the last thing I’m going to talk about is the economic challenges of ASC spine surgery. When we get involved in a surgery center as a physician, there’s obviously some risk involved with making that investment. So we need to do some due diligence and have sort of a proforma and understand our investment in our potential return.
There are contracts with insurance companies that need to be procured. That’s often done by a partnership with a hospital or a surgery center company. Each investment has risk and has return and everyone’s different. Someone who may be established in practice for many years may be okay with making an investment that is riskier. When we’re new in practice, we may be afraid of that type of investment. There’s different risk in return for everyone. There’s no one right answer for what a buy-in should be or what a return should be. It’s really individualized to the patient and the situation. But it’s a good idea to just really understand what you’re getting involved in. From a legal perspective, we have the Stark laws, which essentially prohibit physician referrals to centers where we have ownership because it’s sort of a kickback, but there are a lot of exceptions to that. And surgery centers are really the biggest one. So if we have ownership in a surgery center, we can still have a profit from that ownership. But the profit has to be based on our equity, on our ownership not on the amount of cases we do specifically. It’s not based on the volume or value of referrals, it’s based on what we own in the surgery center. So it’s important to understand that.
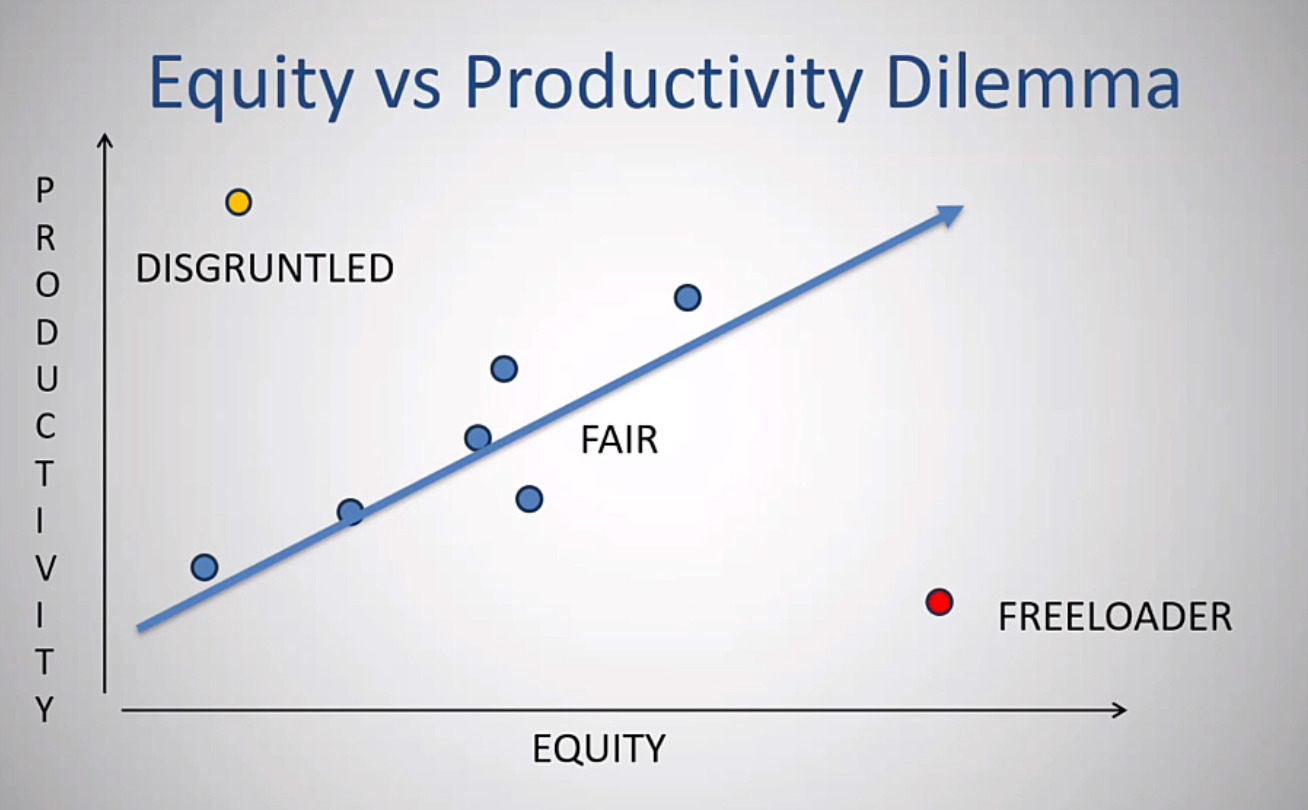
We also need to disclose ownerships to patients, and each state has different laws in terms of certificate of need. It may be easier to construct surgery centers in some state compared to others. From an ethical perspective, most guidelines recommend we use the surgery center only if we really believe the care is as good, if not better than the other options we need to disclose ownership to patients, as I mentioned, and be willing to sort of review our utilization. This is a graph that I created to show sometimes the dilemma that happens in a surgery center when everyone joins in. (Figure 5)
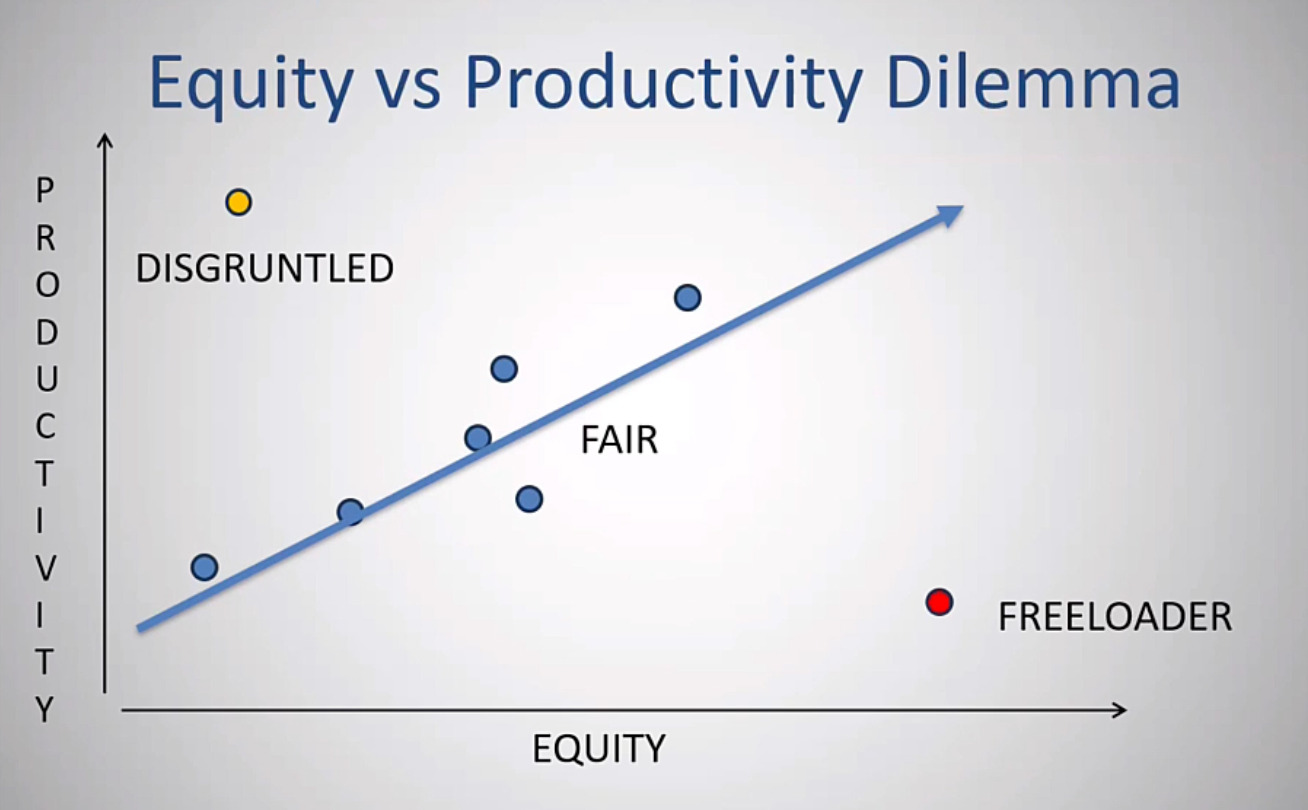
Because the reimbursement or the distribution that each physician gets is based on ownership and not necessarily their production it can create inequities. It is obviously best if our ownership and our production are similar. If I do 5% of the work, ideally I should have about 5% of the ownership and therefore receive about 5% of the distribution. It rarely works perfectly like that for everyone. If there’s a physician who’s very productive but has very little equity, they may become disgruntled on the other hand, if there’s a physician that has a lot of equity but under produces that that person is sort of taking advantage of the others and that can create a situation that breeds conflict among the physicians.
I’d suggest that when these partnerships are set up looking for as much as possible creating a fair situation where ownership and equity are similar that doesn’t mean that everybody has the same amount and it means that everyone should have an amount that’s in line with what they produce as much as you can. This starts from setting things up at the beginning the right way, having a culture of accountability. Physicians can sell equity to each other for a set price in order to even things out if there is a situation of conflict. To summarize, in the surgery center as physicians we generally have more control. We can improve the quality of care for our patients. It can be more convenient for ourselves and our patients. We can lower cost and we can provide competition to hospitals that’s often good for healthcare. All of these start with C, so it’s easy to remember. It’s our responsibility to be the leaders in these ventures, to select the right patients and think about their comorbidities, to set the right expectations for our patients and have our whole team involved in order to be successful. If this is something you’re interested in but haven’t gotten involved with be patient when you first start working in a surgery center. Look for the right types of partnerships and contracting. If you buy in make sure you do a good due diligence and create the right proforma and be a leader in the center.